
Abstract
BACKGROUND AND PURPOSE: There is wide discrepancy between common clinical and radiologic presentations of branchial sinuses arising from the pyriform fossa and the theoretic course of third and fourth branchial arch anomalies. The purpose of this study was to revisit the clinical presentations and imaging features of such anomalies in children.
MATERIALS AND METHODS: A retrospective review of institutional and diagnostic imaging data bases from 1998 to 2008 for reported cases of third and fourth branchial cleft anomalies was conducted. Clinical presentation, pharyngoscopy results, and imaging features in all the patients were evaluated. Surgical and histopathology correlation in patients who underwent excision of the tract was also obtained.
RESULTS: Twenty reported cases described as third or fourth branchial apparatus anomalies were identified. There were 12 females and 8 males with a mean age of 84.6 months. The most common presentation was an inflammatory neck mass (18/20, 90%) almost always involving the thyroid gland. Most lesions were on the left side (16/20, 80%). Pharyngoscopy showed a sinus opening at the piriform fossa in 18/20 (90%) cases. None of the cases followed the classic theoretic pathway of third and fourth arch remnants. Histopathology showed tracts lined with pseudostratified squamous epithelium or ciliated columnar epithelium often associated with inflammatory changes in 17 surgically resected cases.
CONCLUSIONS: Branchial sinuses arising from the pyriform fossa often present with an inflammatory neck mass involving the thyroid lobe, most often on the left side. Imaging and surgical findings suggest that they arise from the embryonal thymopharyngeal duct of the third branchial pouch, because they do not follow the hypothetic course of third or fourth arch fistulas.
Abbreviations
- Adj
- adjacent
- E
- epiglottis
- H
- hyoid bone
- Infl neck mass
- inflammatory neck mass
- L
- left side
- MRI
- MR imaging
- Noninfl
- noninflammatory
- Piriform S
- piriform sinus opening
- R
- right side
- SI
- signal intensity
- TC
- thyroid cartilage
- TG
- thyroid gland
- Thyroid Inv
- thyroid gland involvement
- US
- ultrasonography
Third and fourth branchial anomalies are reported to be rare, accounting for 3%–10% of all branchial lesions.1,2 They result from failure of obliteration of the third and fourth branchial remnants and, in theory, may follow a long and tortuous course in the neck and upper mediastinum. However, there is wide discrepancy between their common clinical and radiologic presentations and the possible theoretic pathways of occurrence as could be predicted by the embryology of these tracts.3,4 Persistence of the thymopharyngeal duct of the third pouch, frequently passing through or adjacent to the thyroid gland, most often on the left side, is thought to be the most suitable embryologic explanation of such sinuses.5
Considerable discrepancy in the definition and description of these lesions exists between the radiologic and surgical literature.4–6 At least some lesions may have been misrepresented in the radiologic literature without adequate supporting evidence from surgical or histopathologic results. These lesions can present, in theory, as a cleft sinus opening to the skin on the side of the neck, a cyst disconnected from the skin and pharyngeal mucosa, a pouch sinus connected to the piriform fossa or upper esophagus, or a through-and-through fistula connecting the skin and the pharyngeal mucosa.1 A more detailed illustrative description of the theoretic course of third and fourth branchial anomalies can be found elsewhere.4,5 However, these anomalies commonly present in children with recurrent neck abscesses or iatrogenic fistula formation following repeated incision and drainage.
This study retrospectively looks at the clinical presentation and imaging features in children with anomalies that may have arisen from the third or fourth branchial apparatus. The need for standardized nomenclature is emphasized to reduce the discrepancy between the radiologic and surgical literature of these lesions.
Materials and Methods
We retrospectively reviewed institutional and diagnostic imaging data bases of The Hospital for Sick Children, Toronto, from 1998 to 2008, for reported cases of third and fourth branchial cleft anomalies. The study was approved by the local research ethics board. Electronic patient records and PACS were used for obtaining details on clinical presentation, pharyngoscopy results and imaging features in all the patients with surgical findings, and histopathologic correlation in patients who underwent excision of the tract. Imaging features of interest included side, site, nature and extent of the neck lesion, evidence of neck infection or abscess formation, and thyroid gland involvement. Surgical notes were analyzed regarding the extent and anatomic relations of the duct remnant with pathologic correlation in all patients who underwent surgical excision of the tract.
Results
We identified 20 reported cases described as third or fourth branchial apparatus anomalies confirmed by pharyngoscopy and/or surgery and histopathology during the period of 1998–2008. There were 12 females and 8 males, with an age range of 9 months to 15 years 11 months (191 months) with a mean age of 84.6 months. Some of these cases have been included in a previously published surgical article.5 All except 3 patients had undergone contrast-enhanced CT study of the neck. Six patients had gadolinium-enhanced MR imaging, and 11 also had sonography of the neck. In addition, 1 patient underwent a barium study of the pharynx and upper esophagus; and another one, a nuclear medicine imaging of the thyroid gland. The demographics, clinical presentation, imaging, and direct pharyngoscopy findings are summarized in the Table.
Demographics, clinical presentation, pharyngoscopy findings, and imaging
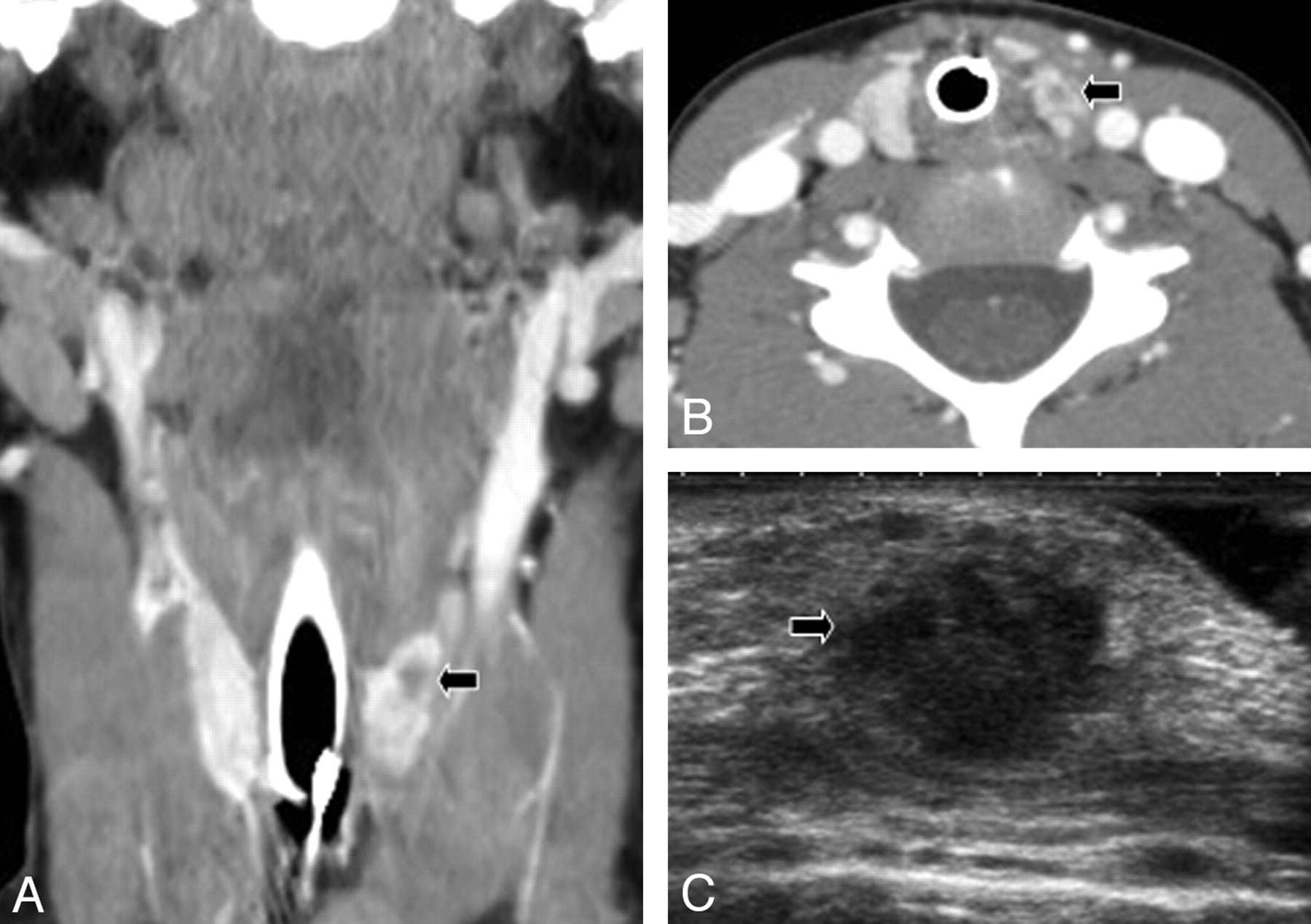
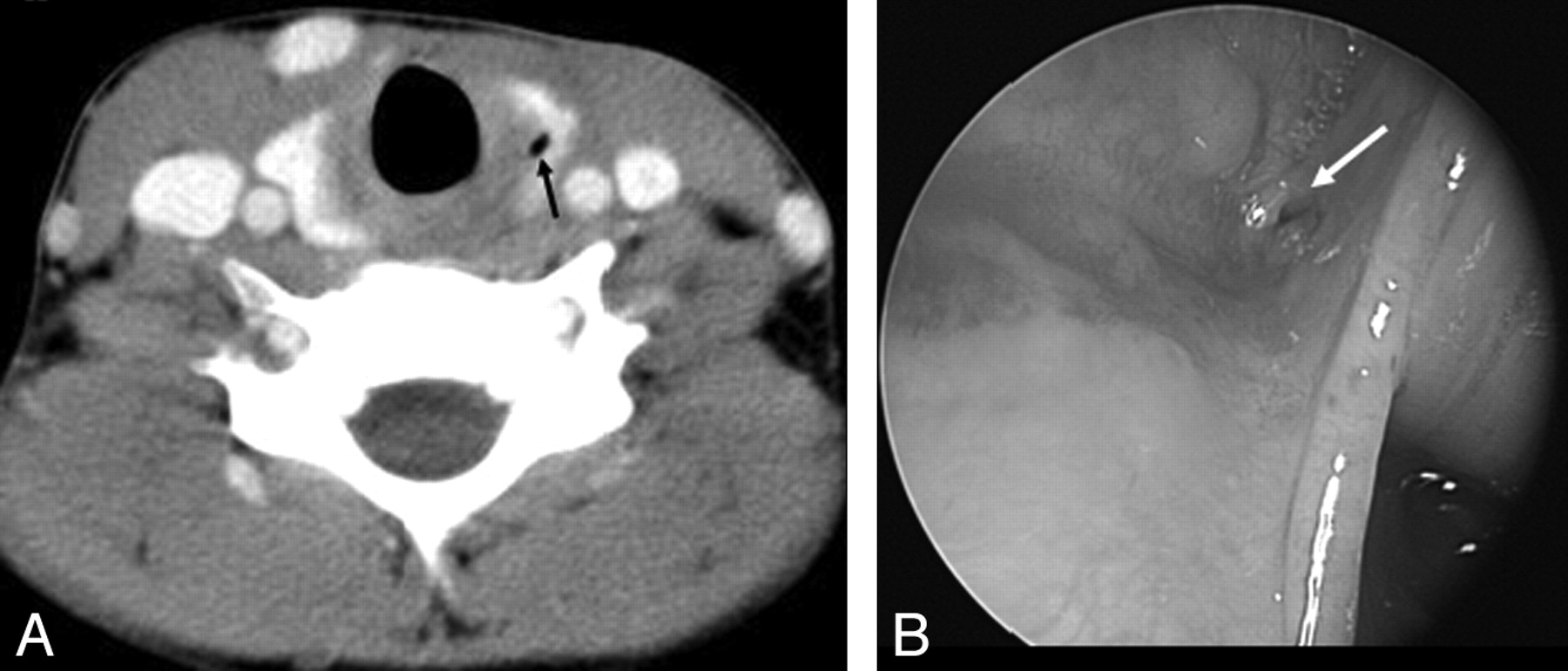
The most common presentation was an inflammatory neck mass (18/20, 90%), sometimes with abscess (10/20, 50%) and almost always involving the thyroid gland or remaining in close proximity to it (20/20, 100%). Most of the lesions were on the left side (16/20, 80%). Four patients (20%) presented with a right-sided neck mass. The lesions ranged from a small inflammatory focus confined to the upper pole of the thyroid (Fig 1) to large abscesses tracking from the piriform sinus to the thoracic inlet anterior and medial to the sternocleidomastoid muscle (Fig 2). Only 1 case showed the characteristic air pocket within the thyroid gland (Fig 3A). Two cases were not seen to be inflamed, both on the right side; and 2 were not traversing the thyroid lobe but remained in proximity. Many patients had been referred from outside institutions and had a history of recurrent neck abscesses for which multiple surgical procedures had been performed previously, including incision and drainage or incomplete excision of the mass.

Infective lesion involving the upper pole of left thyroid lobe (arrow) associated with a third/fourth brachial remnant. Contrast-enhanced coronal CT reformation of the neck (A), contrast-enhanced coronal axial CT scan at the level of the thyroid gland (B), and a sonogram of the left thyroid lobe (C) show the phlegmonous lesion. Pharyngoscopy (not shown) revealed an opening at the apex of the left piriform sinus.

Extensive left-sided neck infection with abscess (thin black arrow) formation and involvement of the left thyroid lobe (thick arrow). Contrast-enhanced coronal T1 fat-saturated MR image of the neck (A), contrast-enhanced axial T1 fat-saturated MR image (B), and contrast-enhanced axial CT scan at the level of the thyroid gland (C) demonstrate the lesion well.

A, Contrast-enhanced axial CT scan at the level of the thyroid gland shows a small air pocket within the left lobe of the thyroid gland (black arrow), which is thought to be characteristic of a branchial sinus remnant. B, Pharyngoscopy photograph shows the opening (white arrow) of the branchial pouch sinus in the apex of the pyriform fossa.
All patients had undergone a direct pharyngoscopy with a straight blade laryngoscope at the time of the initial incision and drainage of the neck abscess or before definitive surgical excision of the tract. Pharyngoscopy showed a unilateral sinus opening at the piriform fossa, commonly on the left (same side-of-the-neck lesion) in 14 cases (Fig 3B). Three of the right-sided lesions had a right piriform sinus pit, and the fourth right-sided lesion had bilateral piriform fossa sinus openings. The piriform sinus opening could not be demonstrated in 2 patients, and in both patients, the nature of the lesion was confirmed by surgery and histopathology. All of the sinus tracts exited the pharynx at a level caudal to the superior laryngeal nerve.
Surgery for the sinus tracts was performed with almost a bloodless microbipolar dissection technique, which allowed excellent surgical visualization and verification of the tract. Exploration of levels 4 and 5 of the neck was routinely performed after mobilizing the ipsilateral hemithyroid and exploring the great vessels and very carefully searching for any tract or remnant extending laterally either superficial or deep to the great vessels. None were found, and none followed the theoretic course of a third or fourth arch fistula around the carotid or subclavian artery/aortic arch. All except 3 patients had undergone definitive surgical excision, often with ipsilateral thyroid lobectomy; and the others are being evaluated for possible surgical excision. Histopathology showed evidence of a tract lined with pseudostratified squamous epithelium or ciliated columnar epithelium often associated with inflammatory changes and fibrosis along the resected thyroid tissue. One left-sided intrathyroid cystic lesion showed evidence of a branchial cleft lining without any duct remnant extending to the piriform sinus.
Discussion
Anomalies that are thought to arise from third or fourth branchial remnants are typically found in the neck as a sinus tract communicating with the piriform sinus of the hypopharynx. In children, they commonly present with recurrent neck infections or abscesses, most often occurring on the left. There is considerable discrepancy noted between the usual clinical and radiologic presentation and the theoretic embryologic course of these remnants.4,5
These embryonal pouch remnants often present with recurrent neck infections, mainly on the left side, with associated thyroiditis or abscess following bouts of upper respiratory infection.3–15 The sinus opening acts as a conduit for the spread of infection from the pharynx. Eighty percent of the lesions in the current study were on the left side, in agreement with the previous reports.3–7 This is perhaps due to the asymmetric vascular development of these branchial arches.16 Many of these patients had recurrent neck infections with a history of multiple occurrences of surgical abscess drainage and antibiotic therapy. Infected lesions were often associated with significant inflammatory adenopathy in the neck (90%).
Only 2 patients in our series presented without infection, and both anomalies were on the right side, remaining adjacent to but not traversing the thyroid gland. Direct pharyngoscopic examination showed a pit or sinus opening in the piriform fossa in all except the 2 noninfected patients. It has been claimed that the third pouch remnant will leave a rostral pit and the fourth pouch will have an apical opening in the piriform fossa and that this information can potentially differentiate them.16 However, more recent reports negate this claim and show that considerable overlap exists.4 All suspected cases of neck and thyroid infection in children, especially on the left side, should undergo a direct pharyngoscopic examination, which could potentially demonstrate the branchial pouch origin of these lesions and hence aid in planning for early definitive surgery. This is especially important because several published reports note the presence of significant delay between the initial clinical presentation and definitive surgery.3–6,17
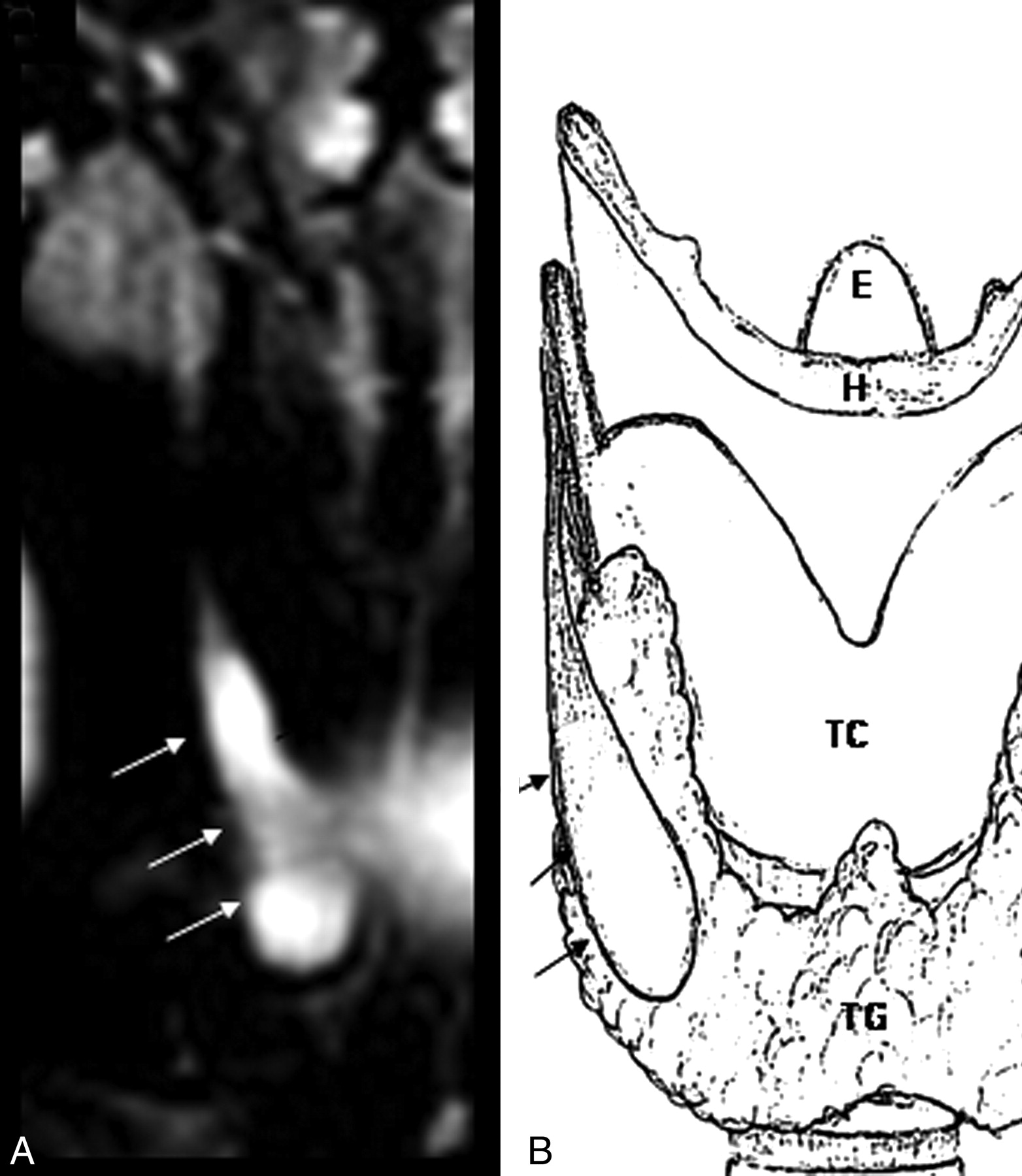
Evaluation of branchial embryology assists understanding of the nature of these anomalies. The primitive pharynx has ectodermal branchial clefts and endodermal branchial pouches separated by mesenchymal branchial arches.4–6 The thymus develops from the ventral component, and the inferior parathyroid gland originates from the dorsal component of the third pouch, whereas the superior parathyroid sprouts from the dorsal expansion of the caudal pharyngeal complex of the fourth pouch and the rudimentary fifth pouch.2,3 The fourth branchial pouch may contribute to thyroid development (the ventral portion forms the ultimobranchial body) and also the thymus gland.7 The lumen of the thymus primordia from the third pouch is initially patent and usually closes after the fusion of the thymic tissues from either side. Failure of this lumen to close may result in persistence of the thymopharyngeal duct (Fig 4), thus leading to a branchial sinus in communication with the pharynx.5 The close proximity of the duct remnants to the thyroid gland can also be explained by descent of the thyroid and the thymic glands in the neck at around the same time (the seventh and eighth weeks of gestation).6

Noninfected third branchial cleft cyst on the right side of the neck following the course of the embryonal thymopharyngeal duct (arrows). A, Coronal T2 fat-saturated image. B, Schematic representation of the course of the thymopharyngeal duct.
Although terminology is often used interchangeably in the radiology literature,18,19 as emphasized by Rea et al,4 it is important to use standardized nomenclature in the description of the branchial apparatus anomalies. A “sinus” is a blind-ending tract. A “branchial cleft sinus” connects to the skin, whereas a “branchial pouch sinus” connects to the pharynx, neither of them arising from the mesenchyme of the branchial arch.4 A “true fistula” is a communication between 2 epithelialized surfaces; a “congenital branchial fistula” should be present at birth and should communicate between a persistent pouch and a cleft. Most of the branchial fistulas reported in the literature are actually pseudofistulas, formed between a pouch remnant and a skin opening produced following an infection or a surgical incision, or are just sinuses. There was no true congenital fistula in our series, as also noted in previous studies.4,5 One should adhere to strict definitions of these terms in reporting these lesions to avoid further confusion in the literature.
None of the cases in the present series followed the classic description of the course of the third and fourth branchial remnants found in the literature.4 This was also noted by previous investigators, and a third or fourth branchial pouch remnant following the complete classic course passing above the hypoglossal nerve or winding down around the aortic arch or subclavian artery is yet to be demonstrated.3–5,17 We suggest that the explanation for the discrepancy between the theoretic and observed courses of the branchial anomalies arising from an opening in the piriform fossa is that they do not arise from true third or fourth arch fistulas but that they are sinuses arising from persistence of a patent thymopharyngeal duct. A true fistula from endodermal mucosa to ectodermal skin would be expected to follow the more convoluted courses around structures of the third and fourth arches, but it appears that such true fistulas across these arches are exceptionally rare, or possibly nonexistent. In our surgical experience, all lesions arising from the piriform sinus passed caudal to the superior laryngeal nerve. This is taken as demonstrating the route of descent of the thymus from the third pouch down through the fourth arch into the mediastinum, so it does not indicate that the anomaly is of fourth-pouch origin as has been suggested previously.4
A contrast-enhanced CT study has been considered as the investigation of choice in demonstrating the site and extent of the lesion. The presence of air within a left-sided infected lesion in relation to the thyroid gland is thought to be characteristic of a branchial pouch sinus as the underlying cause; however, this is seen in only a very few cases. MR imaging can also show the inflammatory lesion but may not be adequate to demonstrate the presence of air in the lesion. Sonography with a “trumpet maneuver” may also demonstrate the sinus.19
A barium study of the pharynx is considered essential by some authors, who suggest that it should be performed after the acute inflammation is over to reduce the false-negative results.20,21 However, another study has reported only a 50% sensitivity for barium examination compared with pharyngoscopy.18 In our experience, a barium study is not required to diagnose these lesions, and all the suspected cases should undergo a rigid pharyngoscopy with a straight blade laryngoscope, in an attempt to improve the sensitivity of detecting a piriform sinus opening. The only case in our series in which a barium study was available failed to demonstrate the piriform sinus pit seen on pharyngoscopy.
There were 2 cysts in our series (10%) that failed to show a pyriform sinus opening and presumably did not have any sinuses passing from the pyriform sinus through the thyroid gland. We postulate that these could be cysts in which the sinus opening has closed over spontaneously with time, obliterated by recurrent inflammation, or that the cysts were presumed to be different from the other lesions that were associated with sinuses. The lining of these cysts indicates that they arise from the endoderm of a branchial pouch, but we cannot be certain whether they arise from the third or fourth pouch. One case showed bilateral pits, but the inflammatory neck lesion was unilateral.
Histopathologic demonstration of the sinus tract lined with squamous or respiratory epithelium in the resected specimen is important for the diagnosis of branchial cleft lesions and for ensuring complete surgical excision. However due to chronic inflammation and recurrent scarring, it may not always be possible to demonstrate it. The presence of inflammation and fibrosis of the adjacent thyroid tissue can also be seen quite often.
Conclusions
Lesions frequently described as third or fourth branchial anomalies typically arise from the piriform sinus of the hypopharynx. They often present with inflammatory neck masses involving the thyroid lobe, most often on the left side. Imaging studies, especially contrast-enhanced CT, are important to assess the site, size, and thyroidal involvement of the lesion accurately. However, imaging alone cannot differentiate lesions of third and fourth branchial remnant origin. A standardized nomenclature for reporting these diverse lesions should be used to avoid confusion in the radiology literature. Imaging and surgical findings together suggest that branchial anomalies arising from the piriform fossa are sinuses arising from the embryonal thymopharyngeal duct because they do not follow the classic and hypothetic course of third or fourth arch fistulas. Use of the term “third branchial sinus” is, therefore, most appropriate for branchial lesions involving the thyroid gland.
Footnotes
-
Paper previously presented in part at: Annual Meeting of the American Society of Head and Neck Radiology, September 10–14, 2008; Toronto, Ontario, Canada; and Annual Meeting of the American Society of Neuroradiology, May 16–21, 2009; Vancouver, British Columbia, Canada.
References
- Received April 29, 2009.
- Accepted after revision August 31, 2009.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}