
Abstract
SUMMARY: In this report, we present a case of a patient with CT angiographic artifacts related to left-sided venous injection resulting in a striking pattern of enhancement simulating vascular abnormalities, which prompted additional diagnostic imaging. To our knowledge, no similar case has been reported in the published literature to date.
With the development of high-speed multidetector CT units, CT angiography is increasingly becoming a primary tool for evaluation of the vasculature of the head and neck. Although a major advantage is its relative noninvasiveness compared with conventional catheter-based vascular imaging, disadvantages and pitfalls do exist. Failure to recognize these at the time of acquisition and interpretation can lead to poor-quality examinations or, worse, incorrect diagnoses and additional potentially unnecessary imaging or other work-up.
We present a case of a patient with artifacts related to left-sided venous injection resulting in a striking pattern of enhancement simulating vascular abnormalities, which prompted additional diagnostic imaging. To our knowledge, no similar case has been reported to date.
Case Report
A 59-year-old man with a prior sternotomy for mitral valve repair presented to the emergency department with acutely worsened intermittent vertigo. The possibility of vertebrobasilar ischemia was raised, and a CT angiogram of the neck and head was obtained on a 64-row multidetector CT scanner (Definition; Siemens Medical Systems, Erlangen, Germany) by using a timing bolus triggered from the left internal carotid artery. In this case, venous access was in the left antecubital vein. Contrast injection was 100 mL of iohexol (Omnipaque 350; GE Healthcare, Giles, UK) at 5 mL per second with a 27-second scanning delay.
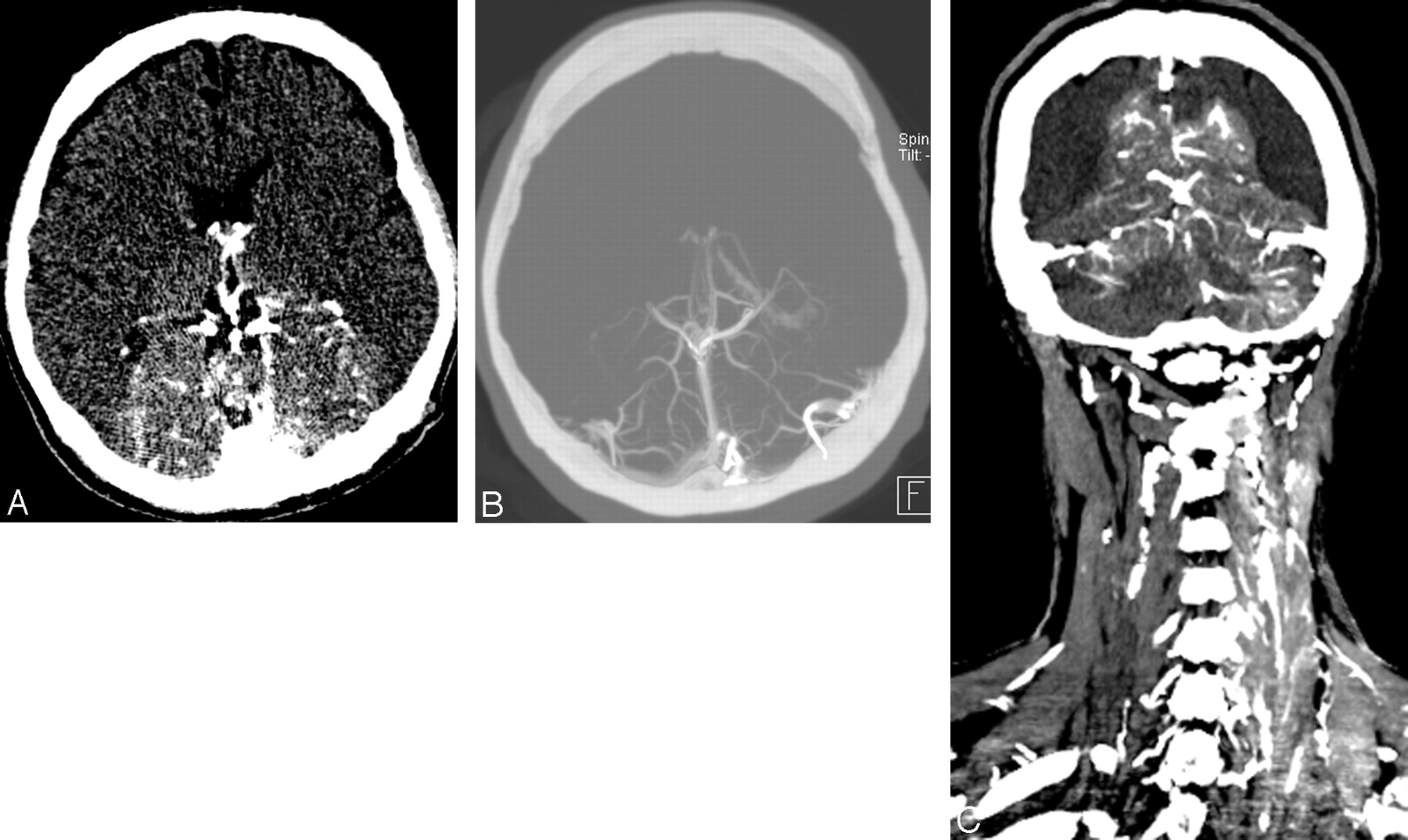
The CT angiogram demonstrated marked parenchymal enhancement in the posterior fossa, medial occipital, and parietal lobes; and opacification of the transverse and sigmoid sinuses and deep venous structures, generally corresponding to posterior circulation territories (Fig 1 A–C). Venous enhancement was also prominent in the left neck more than the right, including the bilateral internal jugular, subclavian, and brachiocephalic veins; the superior vena cava; and the epidural venous plexus and cervical venous plexus, obscuring vertebral artery enhancement. Parenchymal enhancement was evident in the dorsal cervical spinal cord and the left lobe of the thyroid gland. Arterial enhancement in the head and neck was suboptimal, generally less than that of the venous structures detailed above.

A, Source image from the CT angiogram of the brain demonstrates abnormal parenchymal enhancement corresponding to the posterior cerebral circulation territories. B, Maximum-intensity-projection image of the CT angiogram of brain demonstrates abnormal parenchymal enhancement and attenuated opacification of the deep cerebral veins and straight and transverse sinuses. C, Coronal reconstruction from the CT angiogram of the head and neck demonstrates abnormal parenchymal and venous enhancement corresponding to posterior circulation territories. There is also enhancement in the left paraspinal muscles and veins.
To evaluate further for structural or vascular abnormalities, we performed an MR imaging of the brain with MR angiography. Contrast-enhanced 3D MR angiography of the neck demonstrated prominent enhancement of the cervical venous plexus on arterial and delayed phases, without a clear vascular malformation or arterial feeder. Findings of brain MR imaging, MR angiography, and MR venography were unremarkable. Findings of conventional angiography were normal. CT angiography of the head and neck was ultimately repeated by using a right-sided venous injection, the findings of which were within normal limits.
Discussion
Both original CT and MR angiograms were obtained with left-sided venous injections. Further review of the initial CT angiogram revealed narrowing of the retrosternal distance (Fig 2) to 0.2 cm and narrowing of the brachiocephalic vein ipsilateral to the side of injection, which was redemonstrated on MR angiography.

Axial source image from the CT angiogram of the neck demonstrates narrowing of the brachiocephalic vein between the brachiocephalic artery and the sternum, with a wire from a prior sternotomy. Retrosternal distance measures 2 mm at this level.
With normal conventional angiography and CT angiography by using a right-sided injection, the most likely explanation for the abnormal pattern of enhancement on the initial studies was functional and/or structural narrowing of the left brachiocephalic vein related to a narrowed substernal distance. We propose that this resulted in preferential retrograde flow into the left jugular vein and intracranial venous system with reflux through the transverse and sigmoid sinuses to the right intracranial and cervical venous system, in this case overwhelming vascular autoregulation such that parenchymal enhancement occurred. The mechanism for the left thyroid gland enhancement is less clear, though elevated venous pressures may be an explanation.
Artifacts related to left-sided venous injection for cross-sectional angiographic studies are well-documented in the literature. These may include attenuated contrast in the brachiocephalic vein obscuring adjacent arteries,1 reflux of contrast into the jugular veins simulating filling defects, and simple reflux into the internal jugular vein and/or vertebral veins or vertebral venous plexus2 reaching the dural venous sinuses.3,4 None, however, have demonstrated retrograde brain parenchymal enhancement.
There are multiple suggested etiologies for the left-sided predominance of venous reflux. Anatomic differences in the course of the brachiocephalic veins may be a factor.5 The right brachiocephalic vein is more parallel to the ascending aorta, whereas the course of the left crosses the aorta and is, therefore, more susceptible to anatomic compression. An aberrant right subclavian artery may compress the left brachiocephalic vein.4 Hypertension or age-related ectasia and tortuosity of the aorta may also compress the brachiocephalic vein.
Retrosternal narrowing was evident in this case, which has been found to predispose to jugular venous reflux with left-sided injections. Tseng et al3 found that patients who were scanned serially with injections on both sides had no reflux when the retrosternal distance was 1.3 cm but did reflux with retrosternal distances of 0.65 cm. Our patient's retrosternal distance was 0.2 cm. The phase of respiration during contrast injection may also affect the retrosternal distance inversely with thoracic volume.4 Also, the jugular venous valves may be absent, more often on the left than the right in autopsy series.6 When present, venous valves may become incompetent, especially in patients with long-standing severe tricuspid regurgitation7 or after thoracoabdominal trauma.8 In addition to left-sided reflux, general venous return from injection of the upper extremities can be decreased by increased intrathoracic pressure, mediastinal masses, occlusion or stenosis of the superior vena cava, arm positioning, or congestive cardiac failure.9–12 Any of these concomitant conditions may contribute to venous reflux or delay of the arterial phase of enhancement.
The best explanation for this unusual pattern of enhancement on our patient's initial CT and MR angiographic studies is retrograde flow into the cervicocranial venous system, due to left-sided injection with impaired venous flow at the level of the left brachiocephalic vein related to narrowing of the retrosternal distance. This explanation confirms and reinforces existing recommendations that CT or MR angiography be performed with right-sided injection when possible, to minimize venous reflux.
References
- Received April 15, 2009.
- Accepted after revision April 20, 2009.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Pseudopathologic vertebral body enhancement
- Author Response: Teaching NeuroImages: Pseudopathologic Brain Parenchymal Enhancement due to Vascular Compression in Parotid Tumor
- Teaching NeuroImages: Pseudopathologic brain parenchymal enhancement due to vascular compression in parotid tumor
- Suboptimal Contrast Opacification of Dynamic Head and Neck MR Angiography due to Venous Stasis and Reflux: Technical Considerations for Optimization