
Abstract
BACKGROUND AND PURPOSE: Evaluation of temporomandibular joint (TMJ) soft tissue injuries after condylar fractures remains a challenge with use of conventional radiography and CT. The aim of this study was to explore MR imaging in the assessment of TMJ soft tissue injuries after condylar fractures.
MATERIALS AND METHODS: Eighty subjects (118 TMJs) with condylar fractures were examined with sagittal and coronal MR imaging. Proton attenuation and T2-weighted sequences were the key sequences in our imaging protocol. All of the condylar fractures were classified into condylar fractures with dislocation (group 1, 108 TMJs) and without dislocation (group 2, 10 TMJs).
RESULTS: MR imaging demonstrated the following TMJ soft tissue injuries: 1) disk displacements (91.5%, 105 [97.2%] in group 1 and 3 [30%] in group 2; P < .01). Almost all disk displacements in group 1 were in the anteroinferior direction; 2) abnormal signal intensities of retrodiskal tissues (87.3%, 98 [88.3%] in group 1 and 5 [50%] in group 2; P < .05); 3) joint effusion (85.6%, 95 [88%] in group 1 and 6 [60%] in group 2; P > .05); 4) abnormal inferoposterior attachments of disks (87.3%, 96 [88.9%] in group 1 and 7 [70%] in group 2; P > .05) and joint capsules (85.6%, 94 [87%] in group 1 and 7 [70%] in group 2; P > .05).
CONCLUSIONS: There were significant differences of disk displacement and signal intensities of retrodiskal tissues between both fractures. Most dislocated condylar fractures were characterized with anteroinferior disk displacements along with the fractured fragments. MR imaging could provide additional information of TMJ soft tissue injuries after condylar fractures.
The mandibular condyle fracture is a common mandibular injury that may result in severe changes of the soft tissue structures in the temporomandibular joint (TMJ) and furthermore can affect functions of the joint. Condylar fractures can be classified into fractures with dislocation (fractured fragment outside of the glenoid fossa) and without dislocation (fractured fragment within the glenoid fossa). Because the soft tissue structure is a functionally integrated part of the TMJ, understanding the effects of condylar fractures on the disk, joint capsule, and retrodiskal tissue can assist clinicians to make the best treatment decisions.1-3 In addition, surgical reductions of the hard and soft tissue structures of the TMJ are treatment options for the functional recovery of the joint after condylar fracture.1,4 Statuses and locations of the TMJ soft tissues could provide detailed information for surgical procedures.
Conventional radiography and CT examinations can demonstrate the presence of both dislocated and nondislocated mandibular condylar fractures. However, radiography and CT are not effective in revealing soft tissue changes of the TMJ. Investigators5 believed that damage to the TMJ could be seen more clearly on MR imaging than on clinical and radiographic examinations. Recently, many studies1-12 used MR imaging to evaluate soft tissue changes of TMJ traumatic injuries. Most of them found that MR imaging was helpful in the diagnosis of soft tissue changes after an acute condylar traumatic injury. However, no studies have compared the differences of MR imaging findings in TMJ soft tissue structures between dislocated and nondislocated condylar fractures. The aim of this study was to use MR imaging to assess and compare TMJ soft tissue changes after dislocated and nondislocated condylar fractures. The study would provide anatomic information of TMJ soft tissue injuries for the management of different types of condylar fractures.
Materials and Methods
Subjects
From 2003 to 2007, a total of 81 subjects with 120 fractured condyles of the mandible (confirmed on conventional radiographic or CT examinations) were consecutively referred to our hospital for treatment. MR imaging examinations were performed for all subjects within 1 month after the injuries before management. There were 80 subjects with 118 TMJs who were selected for this study, and 1 remaining subject with bilateral mandibular condylar fractures was excluded because of the poor quality of the MR imaging. The 80 subjects included 50 boys and men and 30 girls and women, ranging in age from 5 to 69 years, with a mean age of 30.6 years. On the basis of the position of the fractured condyles, 118 condylar fractures were divided into 2 groups: group 1, fractures with dislocation (108 TMJs, Figs 1–3) and group 2, fractures without dislocation (10 TMJs, Fig 4).

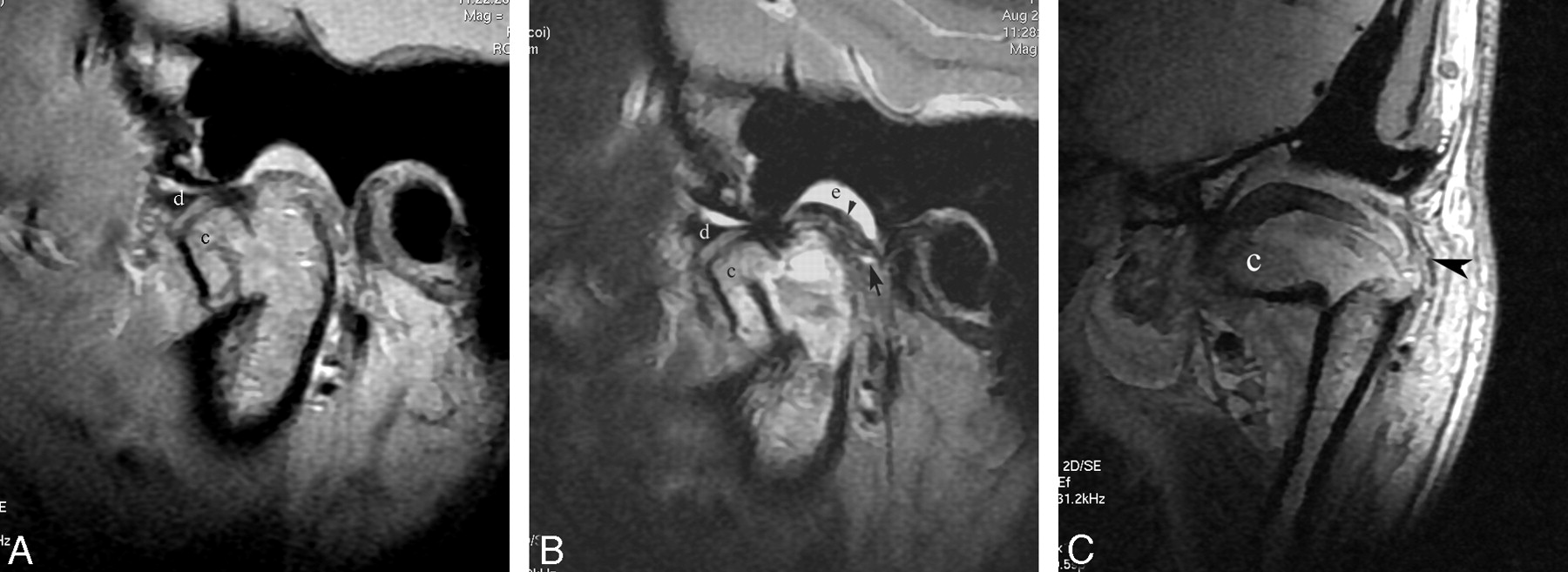
Patient with dislocated mandibular condylar fracture. Sagittal proton attenuation-weighted image (A) and T2-weighted image (B) demonstrate that the fractured condyle (c) is displaced in the anteroinferior direction and out of the glenoid fossa. The TMJ disk (d) is also displaced in the same direction as the fractured fragment. On T2-weighted image (B), the joint effusion (e) is only identified in the upper joint space, and the dotted high signal intensity is found in the retrodiskal tissue (black arrow). The faint inferoposterior attachment and well-defined superior posterior attachment (black arrowhead) of the disk are visible. Coronal proton attenuation-weighted image (C) shows the fractured fragment (c) and well-defined joint capsule (black arrowhead).

Patient with dislocated mandibular condyle fracture. Sagittal proton attenuation-weighted image (A) and T2-weighted image (B) demonstrate that the fractured condyle (c) is anteroinferiorly displaced. The TMJ disk (d) is located superior to the fractured fragment but is anteroinferiorly displaced relative to the remaining mandibular ramus. The tear of the inferoposterior attachment of the disk (black arrow on A) is shown. T2-weighted image (B) demonstrates the dotted high signal intensity of retrodiskal tissue (black arrow), joint effusion of the upper joint compartment (e), and well-defined superior posterior attachment (black arrowhead) of the disk. Coronal proton attenuation-weighted image (C) reveals the tear of the joint capsule (black arrows) and fractured fragment (c) located on the medial side of the mandibular ramus.

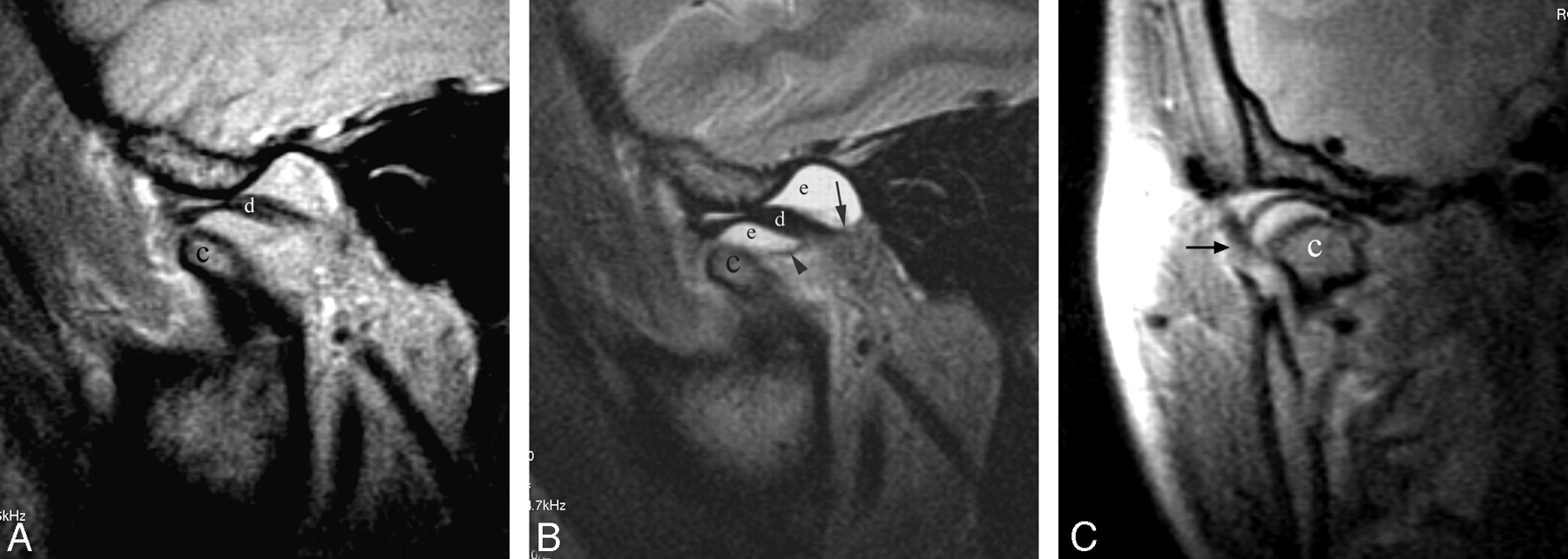
Patient with a dislocated mandibular condylar fracture. Sagittal proton attenuation-weighted image (A) and T2-weighted image (B) demonstrate that both the fractured condyle (c) and the TMJ disk (d) are displaced in the same direction (anterior and inferior direction). The joint effusion (e) with well-defined superior (black arrow) and inferior (black arrowhead) posterior attachments is identified in both the upper and lower compartments of the TMJ on T2-weighted image (B). Coronal proton attenuation-weighted image (C) shows the ill-defined joint capsule (black arrow) and fractured condyle (c) located in the medial side of the mandibular ramus.

Patient with nondislocated mandibular condyle fracture. Sagittal proton attenuation-weighted image (A) demonstrates interrupted cortical bone (white arrowhead) of the condyle (c) and avulsion of the TMJ disk (white arrow). However, the location of the TMJ disk is normal. Coronal proton attenuation-weighted image (B) shows a condylar head fracture (c). The outline of the lateral side of the joint capsule is completed (white arrow).
MR Imaging
MR imaging examinations of the TMJs were performed on a 1.5T Signa TwinSpeed system (GE Healthcare, Milwaukee, Wis). The dual TMJ array coil was applied in this study. Oblique sagittal MR imaging was performed with proton attenuation-weighted and T2-weighted fast spin-echo sequences. Oblique coronal MR imaging was performed with proton attenuation-weighted fast spin-echo sequence. The parameters of the proton attenuation-weighted fast spin-echo sequence were TR, 1360 to 2000 ms; TE, 20 to 26 ms; 3 acquisitions; FOV, 10 × 10 cm; bandwidth, 31.2 Hz; matrix, 320 × 192; section thickness, 2 mm (oblique sagittal) and 1.5 mm (oblique coronal); and spacing, 1 mm (oblique sagittal) and 0.5 mm (oblique coronal). The parameters of the oblique sagittal T2-weighted fast spin-echo sequence were TR, 3760 to 4300 ms; TE, 82 to 90 ms; 3 acquisitions; FOV, 10 × 10 cm; bandwidth, 31.2 Hz; matrix, 320 × 192; section thickness, 2 mm; and spacing, 1 mm.
Criterion and Statistical Analysis
The location of the normal TMJ disk was defined by the posterior band of the disk at the superior (12 o'clock) position relative to the top of the condyle in the glenoid fossa in the closed-mouth position. On T2-weighted images, the increased signal intensity that appeared in the bilaminar zone was defined as an abnormal signal intensity of the retrodiskal tissue. Joint effusion was identified as an area of high signal intensity in the joint space at least in 2 consecutive sections.13 The absence of a biconcave shape of the disk was depicted as a disk deformity. Disk perforation or avulsion was established when the disruption of the disk was shown on MR imaging. An abnormal joint capsule and superior and inferior posterior attachments of the disk were delineated as a tear and were ill defined. The former (tear) was clarified as the disconnection of the joint capsule and posterior attachments of the disk; the latter (ill definition) as the irregular or faint contour of the joint capsule and posterior attachments of the disk.
Three blinded radiologists visually and independently inspected all of the MR imaging studies of 118 TMJs. The opinions were accepted when 2 or 3 observers achieved consensus. The Bonferroni correction was used to compare differences between condylar fractures with dislocation and without dislocation. A P value of less than .05 was considered as a statistically significant difference.
Results
MR imaging demonstrated the following soft tissue changes after fractures of the mandibular condyles: disk displacements (Figs 1–3), joint effusion (Figs 1–3), disk deformation, disk perforation or avulsion (Fig 4), abnormal signal intensity of retrodiskal tissue (Figs 1–2), abnormal superior posterior attachments of the disks, abnormal inferior posterior attachments of the disks (Figs 1–2), and abnormal joint capsules (Figs 2–3). Detailed MR imaging findings of the 2 groups of condylar fractures are listed in the accompanying table.
Different soft tissue changes of TMJ between group 1 and group 2 on MR images
Disk displacements were seen in 108 (91.5%) of 118 TMJs (105 in group 1 and 3 in group 2). There was a significant difference between the 2 groups (P < .01). In group 1, 104 (99%) of 105 disks were anteroinferiorly displaced relative to the remaining mandibular condyle or ramus. The remaining disk was anteriorly displaced. In group 2, only 3 of 10 TMJs had disk displacements. They were all anteriorly displaced, and no anteroinferior displacements were seen.
Joint effusion was identified in 101 (85.6%) of 118 TMJs (95 in group 1 and 6 in group 2). There was no significant difference between the 2 groups (P > .05). Of 101 TMJs, 24 (20 in group 1 and 4 in group 2) had effusions only in the upper joint compartments on T2-weighted imaging (Figs 1–2). The remaining 77 joints had effusions (75 in group 1 and 2 in group 2) in both upper and lower joint compartments (Fig 3).
Abnormal signal intensities of the retrodiskal tissues were revealed in 103 (87.3%) of 118 TMJs (98 in group 1 and 5 in group 2). There were significant differences between the 2 groups (P < .05).
On MR imaging, 45 TMJs were seen with abnormal superoposterior attachments of the disk and 103 TMJs with abnormal inferoposterior attachments of the disk. There was a statistically significant difference between the abnormal superoposterior and inferoposterior attachments of the disks (P < .05). Of 45 abnormal superoposterior attachments, 15 (33.3%) appeared as a tear and 30 (66.7%) were ill-defined. Of 103 abnormal inferior posterior attachments, 28 (27.2%) appeared as a tear (Fig 2) and 75 (72.8%) were ill-defined (Fig 1). Furthermore, 103 abnormal inferoposterior attachments were found (96 in group 1 and 7 in group 2). There was no significant difference between the 2 groups of condylar fractures (P > .05).
Abnormal joint capsules were demonstrated in 101 (85.6%) TMJs (94 in group 1 and 7 in group 2). There was no significant difference between the 2 groups (P > .05). Of 101 abnormal joint capsules, 21 (20.8%) appeared as a tear (Fig 2) and 80 (79.2%) as faintness (Fig 3). There were 4 (3.4%) of 118 mandibular condyle fractures accompanied with fractured glenoid fossa of the temporal bones.
Discussion
Previous MR imaging studies1-12 indicated that the soft tissue changes included abnormal disk locations, disk shape, disk avulsion, retrodiskal tissues, joint spaces, and joint capsules. The current study demonstrated that the TMJ soft tissue changes were mainly with disk displacements, joint effusion, abnormal retrodiskal tissues, and joint capsules. There were statistically significant differences of the soft tissue changes between the dislocated and nondislocated condyle fractures in disk positions and signal intensities of retrodiskal tissues.
Abnormal TMJ Disk
An abnormal TMJ disk shown on MR images refers to the disk displacement, deformity, and perforation. The anterior or anteromedial displacement of the disk after TMJ injury has been reported in previous literature1-4,6-8,11 since Schellhas6 described the sign in 1989. However, Westesson et al7 depicted that the TMJ disk was located superiorly to the fragment of the condyle and was anteriorly and inferiorly displaced relative to the remaining condyle on sagittal MR images. Takaku et al2 pointed out that all disks were displaced in an anteromedial direction along with the fractured condylar fragments. Oezmen et al1 and Gerhard et al8 found a low rate of disk displacement in patients with a condylar injury. Bergman et al11 reported that there was no significantly increased incidence of disk displacement, joint effusion, or any other injury to the TMJ between patients with whiplash trauma and volunteers.
Our findings on sagittal MR images indicated that almost all of the TMJ disks in dislocated condylar fractures were anteriorly and inferiorly displaced relative to the remaining mandibular condyle, whereas the TMJ disks in nondislocated condylar fractures were in the normal position or displaced anteriorly. There was a statistically significant difference between these 2 groups of condylar fractures in disk displacements. The sign of disk displacement in the anteroinferior direction was infrequently described. The TMJ disks in group 1 cases were always displaced in the same direction as the fractured fragments of condyles. Dislocated condylar fractures always presented with anteroinferiorly displaced disks because of the contraction of the lateral pterygoid muscles, which could pull the fractured mandibular condyle and disk forward.
Sullivan et al10 found that the condylar fracture was associated with a high incidence of disk avulsion, accounting for 77%, whereas other studies failed to correlate the sign of disk avulsion with the condylar fractures.2,9 The differences might be related to the discrepancies of the diagnostic criteria of condylar injuries, types of condylar fractures, and disk avulsion applied in the respective studies.8-9 The disk perforation or avulsion and disk deformity were infrequently visible in our study. We considered that a low rate of disk perforation or avulsion may result from the lower spatial resolution of MR imaging.
Joint Effusion after TMJ Injuries
Joint effusion after TMJ injuries has been reported in previous literature.1-2,6-12 Takahashi et al12 suggested that MR evidence of joint effusion might serve as a marker for the detection of severe intra-articular damage to the TMJ after mandibular condylar fractures. However, another study11 found no significant difference in joint effusion between patients with TMJ injury and volunteers. Our results showed that most joint effusions were present with most traumatic TMJ injuries. Although there was no statistically significant difference of TMJ effusion between both groups, the dislocated condylar fractures with joint effusion were more frequently seen than nondislocated condylar fractures, which seemed to imply a relationship between the severity of the traumatic injury and joint effusion. Fractures with dislocated condylar fragments usually have more severe damage to TMJs than those fractures without dislocated condylar fragments. Therefore, we see more joint effusion in group 1. Furthermore, Emshoff et al9 found that effusion in the superior joint space was seen more often compared with the inferior space. A similar result was also found in our study. We assumed that this phenomenon might be related to the complete or incomplete tear of the inferoposterior attachment of the disk, which could result in overflow of the effusion from the inferior compartment of the TMJ.
Abnormal Joint Capsule
On the basis of the MR imaging findings in our study, abnormal joint capsules included tears of the joint capsule and ill-defined joint capsules. Takaku et al2 depicted the tear of the joint capsule as a dotted high-signal intensity area. They also noticed that the contour of the joint capsule was irregular. The tear of the joint capsule shown on MR imaging was also discussed in other investigations.8-10 We considered that the tear capsule should appear as a disruption of the joint capsule on MR imaging, which might be separated by a dotted high-signal intensity area on sagittal and coronal proton attenuation–weighted or T2-weighted images. Absence of a smooth contour or an irregular shape should be considered as the ill-defined or faint joint capsule. Our data demonstrated that the ill-defined capsules were more often visualized than the tears on MR imaging. This finding might be related to the fact that most small splits of joint capsules (incomplete tear) were difficult to identify on lower spatial resolution of MR imaging.
Abnormal Posterior Attachments of the Disk
From an anatomic standpoint, the posterior attachments of the TMJ disk are composed with the superior and inferoposterior attachments. The retrodiskal tissue tear has been delineated in previous investigations.2,9 In our study, although there was no statistically significant difference between group 1 and group 2 with regard to abnormal posterior attachments of the disk, the abnormal inferoposterior attachments of the disk were more often seen than the abnormal superior attachments. This finding might be because of the close anatomic relationship between the inferoposterior attachments of the disks and the fractured condyles. On sagittal MR images, the abnormal posterior attachments of the disks were recognized as both a tear and faintness on the basis of the evaluating standard of our study. The incomplete tear of the posterior attachment of the disk, which was similar to the incomplete tear capsule and disk perforation, was also infrequently identified because of the lower spatial resolution of MR imaging.
Abnormal Signal Intensity of Retrodiskal Tissue
Using T2-weighted imaging, Sano et al14 pointed out that high signal intensity of the retrodiskal tissue often has a close relationship to severe joint pain. The previous literature2 has evidenced the existence of abnormal signal intensity of retrodiskal tissue after a TMJ injury, suggesting the presence of injury-induced inflammation. In our study, we found a statistically significant difference of abnormal signal intensity in the retrodiskal tissue between group 1 and group 2. This result indicated that the traumatic degree of the retrodiskal tissue was different between the fractured condyles with dislocation and those without dislocation. A parallel relationship between traumatic severity and increased signal intensity of TMJ soft tissue might exist. Dislocated condylar fractures would most likely result in more severe injury of retrodiskal tissue than nondislocated condylar fractures.
Conclusions
Our study demonstrated soft tissue changes of the TMJ after 2 different types of condylar fractures and found differences between the condylar fractures with and without dislocation. On sagittal MR images, the condylar fractures with dislocation were characterized by anteroinferior disk displacement relative to the remaining condyle, which followed the same direction as the fractured fragments. Abnormalities in signal intensities of the retrodiskal tissues, joint effusion, inferior posterior attachment of the disk and joint capsule were more frequently visible in condylar fractures with dislocations.
MR imaging is effective in demonstrating TMJ soft tissue changes of dislocated and nondislocated condylar fractures. Detailed information of the soft tissue injuries might assist clinicians to make an accurate diagnosis as well as the best treatment decisions, provide guidance for any surgical procedures, and monitor recovery of these injuries.
References
- Received March 15, 2008.
- Accepted after revision August 10, 2008.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.