
Abstract
BACKGROUND AND PURPOSE: Arterial spin-labeling (ASL) with image acquisition at multiple delay times can be exploited in perfusion MR imaging to visualize and quantify the temporal dynamics of arterial blood inflow. In this study, we investigated the consequences of an internal carotid artery (ICA) occlusion and collateral blood flow on regional timing parameters.
MATERIALS AND METHODS: Seventeen functionally independent patients with a symptomatic ICA occlusion (15 men, 2 women; mean age, 57 years) and 29 sex- and age-matched control subjects were investigated. ASL at multiple delay times was used to quantify regional cerebral blood flow (CBF) and the transit and trailing edge times (arterial timing parameters) reflecting, respectively, the beginning and end of the labeled bolus. Intra-arterial digital subtraction angiography and MR angiography were used to grade collaterals.
RESULTS: In the hemisphere ipsilateral to the ICA occlusion, the CBF was lower in the anterior frontal (31 ± 4 versus 47 ± 3 mL/min/100 g, P < .01), posterior frontal (39 ± 4 versus 55 ± 2 mL/min/100 g, P < .01), and frontal parietal region (49 ± 3 versus 61 ± 3 mL/min/100 g, P = .04) than that in control subjects. The trailing edge of the frontal-parietal region was longer in the hemisphere ipsilateral to the ICA occlusion compared with that in control subjects (2225 ± 167 versus 1593 ± 35 ms, P < .01). In patients with leptomeningeal collateral flow, the trailing edge was longer in the anterior frontal region (2436 ± 275 versus 1648 ± 201 ms, P = .03) and shorter in the occipital region (1815 ± 128 versus 2388 ± 203 ms, P = .04), compared with patients without leptomeningeal collaterals.
CONCLUSION: Regional assessment of timing parameters with ASL may provide valuable information on the cerebral hemodynamic status. In patients with leptomeningeal collaterals, the most impaired territory was found in the frontal lobe.
An obstructive lesion in the internal carotid artery (ICA) causes a reduction of the perfusion pressure in the cerebral circulation. As the cerebral perfusion pressure decreases, pressure is initially maintained by a compensatory vasodilation of the arterioles, followed by an increase in the oxygen extraction fraction.1 Regionally, the cerebral hemodynamic status depends not only on the degree of carotid obstruction but also on other factors, such as the contribution of collateral pathways.2,3
The collateral circulation can provide alternative routes for oxygenated blood to reach the brain tissue, either through the primary pathways via the circle of Willis or the secondary pathways via leptomeningeal and ophthalmic collaterals.4 The combination of a decreased cerebral perfusion pressure and an insufficient primary collateral blood supply may lead to hemodynamic impairment, which eventually can result in a limited clearance of emboli and ischemia.5,6 Recruitment of the secondary collaterals is associated with further impairment, and its presence may be considered a marker of inadequacy of the primary collateral pathways.7,8 Because the recruitment of collateral perfusion in patients with an ICA occlusion will lead to longer blood flow routes and a delayed arrival time of the blood, regional knowledge of the arrival times of arterial blood may provide additional information to characterize the collateral flow and may potentially be used to identify hemodynamically impaired regions. The most widely used methods to measure arrival times of blood use dynamic sampling of an injected bolus of contrast agent. However, due to the current concerns regarding contrast use in patients with poor renal function9 and ionizing radiation, an alternative without detrimental effects would be of great benefit.
Recently, arterial spin-labeling (ASL) was introduced as a noninvasive method capable of assessing cerebral perfusion and the temporal dynamics of arterial blood inflow.10 The purpose of our study was, first, to investigate hemodynamic parameters in different areas of the brain in patients with an occlusion of the ICA and, second, to evaluate the effect of collateral flow on regional hemodynamics. We used an ASL MR imaging technique with image acquisition at multiple delay times to quantify regionally cerebral blood flow (CBF) and arterial timing parameters (transit and trailing edge times).
Materials and Methods
Patients
The institutional review board approved the study protocol, and written informed consent was obtained from all participants. Seventeen functionally independent patients (15 men and 2 women; mean age, 57 ± 8 years) with an ICA occlusion were included in the study. All patients had transient or minor-disabling neurologic deficits (modified Rankin Scale score of 0–2) on the side of the occlusion11 and were referred to the department of radiology by vascular surgeons or neurologists for diagnosis and grading of the ICA obstruction. Patients who had experienced a severe stroke causing major disability (modified Rankin Scale score of 3–5) in the past were not included. Diagnosis of the ICA obstruction was performed with intra-arterial digital subtraction angiography (DSA), and the presence of a contralateral obstruction was graded in accordance to the North American Symptomatic Carotid Endarterectomy Trial criteria.12 In 11 patients, the ICA occlusion was located on the right side, and in 6 patients, on the left side.
The presence of collateral flow was assessed with intra-arterial DSA and MR angiography (MRA). The direction of blood flow in the circle of Willis was assessed according to a previously published imaging protocol,13 with 2 consecutive 2D phase-contrast MR imaging measurements, of which 1 was phase-encoded in the left-right direction and 1, in the anteroposterior direction. Anterior collateral flow was defined as flow across the anterior communicating artery with retrograde flow in the precommunicating part (A1 segment) of the anterior cerebral artery (ACA). Posterior-to-anterior flow in the posterior communicating artery was considered to represent posterior collateral flow. Leptomeningeal collaterals were judged as present if intra-arterial DSA showed cortical branches extending from the posterior cerebral artery that supplied the flow territory of the middle cerebral artery (MCA) or ACA.
The control group consisted of 29 volunteers (25 men and 4 women; mean age, 57 ± 9 years) without a history of neurologic disease, vascular pathology on T1- or T2-weighted MR imaging or MRA scans, or an ICA stenosis of >30%. The control subjects were matched to the patient group for sex and age. All control subjects were recruited from a vascular screening MR imaging study involving subjects with symptomatic atherosclerosis or risk factors for atherosclerosis.14
MR Imaging
MR imaging investigations were performed on a 1.5T system (Gyroscan ACS-NT; Philips Medical Systems, Best, the Netherlands). For all MR imaging acquisitions, a quadrature head coil was used for radio-frequency transmission and signal-intensity reception. For perfusion MR imaging, a pulsed ASL transfer insensitive labeling technique was used.15 A single-perfusion imaging section was planned just above the ventricles through the centrum semiovale and aligned parallel to the orbitomeatal angle (Fig 1). Labeling was achieved by applying 2 consecutive section-selective 90° radio-frequency pulses in a 140-mm-thick labeling slab 10 mm proximal to the imaging section. For image acquisition, a series of thirteen 35° excitation pulses was applied, with increasing delay times from 200 to 2600 ms with a constant interval of 200 ms, followed by single-shot gradient echo-planar imaging readout. The ASL signal was corrected for imperfections in section profiles.16 Other MR imaging parameters for perfusion imaging were the following: TR, 3000 ms; TE, 5.6 ms; 62% partial Fourier acquisition; averages, 50; FOV, 240 × 240 mm; 64 × 64 matrix; scanning time, 5 minutes.

A, sagittal orientation image illustrating the planning of the imaging section (1) and the arterial spin-labeling slab (2) parallel to the orbitomeatal angle. B, regions of interest used for quantification of the hemodynamic parameters. In each hemisphere, 2 regions of interests were drawn in the frontal lobe, and 1, in the frontal parietal, parietal occipital, and occipital regions.
Cerebral Blood Flow, Transit, and Trailing Edge Quantification
Perfusion-weighed images were obtained by subtracting the labeled images from the control images. In addition to quantifying CBF, ASL can also be used for the measurement of arterial timing parameters. By acquiring a series of perfusion images, it is possible to follow the inflow of labeled blood into the vascular exchange site. The obtained kinetic data of blood inflow can be used to calculate the transit time and trailing edge times. These are physiologic parameters that reflect the time needed for the labeled arterial blood to reach the brain tissue. Transit time is the duration between labeling and the first arrival of the magnetized blood into the imaging voxel. The trailing edge time is the duration needed for the end of the labeled bolus to reach the imaging voxel.
To quantify CBF, transit, and trailing edge time, we fitted the perfusion signal intensity (ΔM) at varying delay times (t) to the kinetic perfusion model of Buxton et al,17 with the adaptations as proposed by Gunther et al18:  (1) where f is the perfusion value CBF in milliliters/minute/100 g, τa is the transit time, τd is the trailing edge time, δR = R1a − R1app, eff and R1app, eff = R1 + f/λ− ln(cosα/ΔTI), λ is the brain/blood partition coefficient, α is the flip angle, ΔTI is the time between consecutive readouts, R1a is the longitudinal relaxation rate of arterial blood, R1 is the longitudinal relaxation rate of tissue, and Ma,0 is the equilibrium magnetization in a blood-filled voxel, estimated by fitting the unlabeled signal intensity in the sagittal sinus to a saturation-recovery curve. The following physical constants were obtained from the literature: R1 = 1000 ms; R1a = 1400 ms; λ (brain/blood partition coefficient of water) = 0.9 mL/g.19,20
(1) where f is the perfusion value CBF in milliliters/minute/100 g, τa is the transit time, τd is the trailing edge time, δR = R1a − R1app, eff and R1app, eff = R1 + f/λ− ln(cosα/ΔTI), λ is the brain/blood partition coefficient, α is the flip angle, ΔTI is the time between consecutive readouts, R1a is the longitudinal relaxation rate of arterial blood, R1 is the longitudinal relaxation rate of tissue, and Ma,0 is the equilibrium magnetization in a blood-filled voxel, estimated by fitting the unlabeled signal intensity in the sagittal sinus to a saturation-recovery curve. The following physical constants were obtained from the literature: R1 = 1000 ms; R1a = 1400 ms; λ (brain/blood partition coefficient of water) = 0.9 mL/g.19,20
Data Analysis
Data were analyzed with mathematic software (Matlab; MathWorks, Natick, Mass). On the basis of the ASL control images, regions of interest were drawn according to a standardized template symmetrically in both hemispheres, in distinct areas of gray matter (Fig. 1). For statistical analysis, the Statistical Package for the Social Sciences for Windows, Version 12.0.1 (SPSS, Chicago, Ill) was used. Mean CBF, transit, and trailing edge times were calculated over all regions of interest in the hemisphere on the side of the symptomatic and contralateral asymptomatic hemispheres. Because no differences were found in CBF, transit, and trailing edge times between the left and right hemisphere in control subjects, values for both hemispheres were averaged for analysis. Differences in CBF, transit, and trailing edge region-of-interest measurements between the hemispheres ipsi- and contralateral to the ICA occlusion and the control group were evaluated by using a 1-way analysis of variance with a Bonferroni correction for multiple comparisons. To examine the influence of collateral flow patterns, we evaluated differences between CBF, transit, and trailing edge times in the hemisphere ipsilateral to the ICA occlusion by using the Student t test. A P value < .05 was considered to indicate a statistically significant difference. Values are expressed as mean ± standard error of the mean (SEM).
Results
The baseline characteristics of the patients are given in Table 1. An example of an ASL MR imaging investigation of a patient with a symptomatic left-sided ICA occlusion is shown in Fig 2. Decreased CBF and increased timing parameters, resulting from a delayed arrival of the magnetically labeled bolus, can be appreciated in the left hemisphere.

Measured perfusion images of a 53-year-old man with a unilateral left-sided ICA occlusion. The images show the absolute cerebral blood flow (A), transit time (B), and trailing edge (C) maps. Decreased cerebral blood flow, increased transit time, and increased trailing edge can be appreciated in the left hemisphere.
Patient characteristics
Regional Quantification of CBF, Transit, and Trailing Edge Time
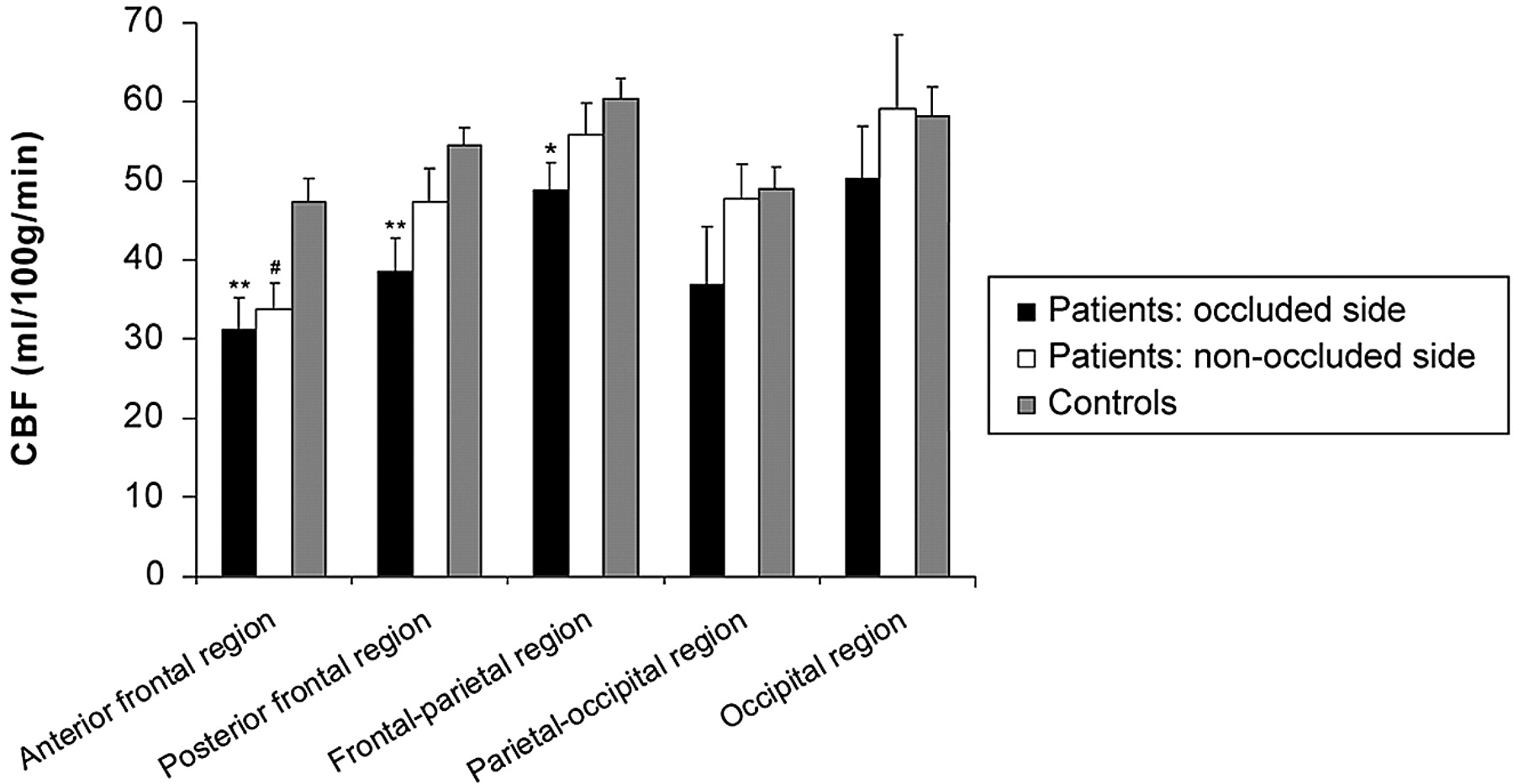
In the hemisphere ipsilateral to the ICA occlusion, the CBF was significantly lower than that in the control subjects in the anterior frontal region (31 ± 4 versus 47 ± 3 mL/min/100 g, P < .01), posterior frontal region (39 ± 4 versus 55 ± 2 mL/min/100 g, P < .01), and in the frontal parietal region (49 ± 3 versus 61 ± 3 mL/min/100 g, P = .04) (Fig 3). In the hemisphere contralateral to the ICA occlusion, CBF in patients was significantly lower in the anterior frontal region than that in control subjects (34 ± 3 versus 47 ± 3 mL/min/100 g, P = .02).

Cerebral blood flow (mean ± SEM) in the regions of the hemisphere ipsi- and contralateral to the occlusion and of the control group. Asterisk indicates P < .05; double asterisks, P < .01, a significant difference between the hemisphere ipsilateral to the ICA occlusion and the control subjects; number sign, a significant (P < .05) difference between the hemisphere contralateral to the ICA occlusion and the control subjects.
The transit time in the posterior frontal region ipsilateral to the ICA occlusion was prolonged (138 ± 52 ms, P = .03) compared with that in the control group (41 ± 11 ms) (Fig 4). In the frontal parietal region ipsilateral to the ICA occlusion, the transit time (158 ± 49, P < .01) and the trailing edge time (2225 ± 167, P < .01) were prolonged compared with the control subjects (respectively, 7 ± 4 ms and 1593 ± 35 ms) (Fig 4). In the hemisphere contralateral to the ICA occlusion, the trailing edge time of the occipital region was significantly shorter in patients than in control subjects (1859 ± 122 ms versus 2289 ± 89 ms, P = .02).

Transit time and trailing edge time (mean ± SEM) in the regions of the hemisphere ipsi- and contralateral to the occlusion and of the control group. Asterisk indicates P < .05; double asterisks, P < .01, a significant difference between the hemisphere ipsilateral to the ICA occlusion and the control subjects; number sign, a significant (P < .05) asymmetry between the hemisphere contralateral to the ICA occlusion and the control subjects; dagger, a significant (P < .01) difference between the hemisphere ipsi- and contralateral to the ICA occlusion.
Patients with leptomeningeal collateral flow (53%, n = 9) had a lower CBF in the posterior frontal region (29 ± 5 mL/min/100 g) than patients without leptomeningeal collaterals (47 ± 6 mL/min/100 g, P = .04) in the hemisphere ipsilateral to the ICA occlusion (Table 2). Furthermore, the trailing edge was longer in the anterior frontal region (2436 ± 275 versus 1648 ± 201 ms, P = .03) and shorter in the occipital region (1815 ± 128 versus 2388 ± 203 ms, P = .04) than that in patients without leptomeningeal collateral flow. No differences in hemodynamic parameters were found for the presence or absence of collateral flow via the anterior (71%, n = 12) or posterior (65%, n = 11) collateral pathways.
Hemodynamic values for the hemisphere ipsilateral to the occlusion in patients with (n = 9) and with leptomeningeal collateral vessels
Discussion
The most important findings of our study were twofold. First, we found significant heterogeneity of regional cerebral hemodynamics in patients with a symptomatic ICA occlusion, with decreased CBF and increased timing parameters in the hemisphere ipsilateral to the occlusion. Second, in patients with leptomeningeal collateral flow, there was a prolonged trailing edge in the anterior and a decreased CBF in the posterior frontal region ipsilateral to the occlusion in comparison with patients without leptomeningeal collateral flow.
Most of the techniques that can assess CBF in patients are invasive and require the injection of a radioactive tracer or contrast agent.21 ASL MR imaging has been developed to measure cerebral perfusion noninvasively by using magnetically labeled blood as an endogenous contrast agent.10 Most current ASL approaches acquire the imaging at a single inversion time point, which, in healthy volunteers, is sufficient for an adequate exchange of the label with the brain tissue water. However, in patients with an occlusion of the ICA, collateral blood flow recruitment may result in increased transit times of the labeled blood to the brain tissue,22 resulting in an underestimation of CBF.23,24 If one performs multiple ASL experiments at various delay times, all labeled spin contributes to the perfusion signal intensity and no prior knowledge of individual transit times is needed. An additional advantage of this acquisition method is that it can be used to visualize and quantify the temporal dynamics of blood inflow and tissue perfusion.18,25 Although previous studies have demonstrated the ability of ASL at multiple delay times to measure timing parameters and the effect of brain activation on timing parameters,15,26–28 this is the first study to investigate the consequences of an occlusion of the ICA and collateral blood flow patterns on regional ASL timing parameters and CBF.
In this study, we found a significant decreased CBF in both frontal and the frontal parietal regions in the hemisphere ipsilateral to the ICA occlusion, which is in agreement with previous positron-emission tomography (PET), 133Xe inhalation, and MR imaging–based studies.29–33 Furthermore, we demonstrated that the time needed for the labeled bolus to travel to the affected hemisphere was increased in patients with a symptomatic ICA occlusion, in regions corresponding to the anterior borderzone and the flow territory of the MCA. In previous studies, researchers found similar regional heterogeneity in hemodynamic parameters with ASL.25 Roughly, measures comparable with the ASL timing parameters are the arrival time and time-to-peak in dynamic contrast-enhanced MR and CT perfusion imaging. In contrast-enhanced perfusion studies of patients with an ICA occlusion, researchers have demonstrated increased time-to-peak times and reduced CBF in the gray and white matter of the affected hemisphere,34–36 which was thought to be caused by decreased flow in the arteries and increased dispersion in the microvasculature. This finding corresponds with our finding of a delayed arrival of arterial blood in the hemisphere ipsilateral to the ICA occlusion.
With the 10-mm gap between the imaging and labeling section, the time needed for the blood from the upper site of the labeled volume to travel to the brain tissue will depend on the vascular pathways distal to the circle of Willis. In contrast, the lower edge of the labeling volume is below the level of the circle of Willis. Therefore the trailing edge time will depend on the vascular pathways both proximal and distal to the circle of Willis. In the evaluation of the impact of collateral flow on the delay of arterial blood, the trailing edge will consequently be the most informative parameter of the 2. Furthermore, the transit and trailing edge times do not necessarily have to show a combined increase in patients with a vascular obstruction because the increase of timing parameters may, for instance, mainly depend on the rerouting of the labeled arterial blood proximal from the circle of Willis.
In our analysis of the role of collateral blood flow, we found that neither flow via the anterior or posterior collateral pathways had an effect on regional hemodynamic parameters in patients with ICA occlusion. Previous studies have indicated that hemodynamic and metabolic changes are more severe in patients without primary collaterals than in patients with primary collaterals,3,37 and that the presence of secondary collateral flow is associated with an impaired hemodynamic status.38,39 In this study, we found that patients with leptomeningeal collaterals and an occlusion of the ICA had a lower CBF and a prolonged trailing edge in the frontal lobe. No differences were found in symptoms between patients with and without leptomeningeal flow. Although the CBF measured in the frontal regions was low, it is above the value of 20 mL/min/100 g, which is considered to indicate tissue at risk.40 We hypothesize that the increased trailing edge time reflects the elongated path that the bolus of magnetically labeled blood has to travel through the leptomeningeal collaterals from the posterior circulation to the frontal lobe.
A disadvantage of using ASL at multiple delay times is the longer scanning duration compared with single-delay experiments. In this study, we used a Look-Locker-like sampling strategy to acquire the series of perfusion images at increasing delay times to decrease scanning time. Although this makes it more practical for clinical use in patients, the train of small flip angle gradient echoes decreases the perfusion signal. Due to this loss and additionally the decrease of signal due to the natural T1 decay of the magnetized blood, we were not able to use crusher gradients. Therefore, a limitation of this study is that due to the presence of magnetic label within the vasculature, there may possibly be a regional overestimation of CBF. Although this is a well-recognized problem of ASL, the CBF values found in both the patient group and the control subjects were within the reported range of previous PET studies.1,30 In the present study, 2 of the 17 patients with an occlusion of the ICA had a contralateral stenosis of ≥70%, which could have affected the hemodynamic measurements in the contralateral hemisphere. Furthermore, the DSA examinations, which were used to judge the presence of leptomeningeal collaterals, were not specifically performed to visualize these collaterals. Therefore, an underestimation of the prevalence of leptomeningeal collaterals is possible. In our study, 9 of the 17 patients (53%) had collateral flow through leptomeningeal vessels. Although there is a large interindividual variability in the number and size of leptomeningeal anastomoses, this is in accordance with previous reported prevalences.41
Conclusion
ASL with image acquisition at multiple delay times can be used to quantify the temporal dynamics of arterial blood inflow and identify brain regions with impaired hemodynamics. In this study, we found significant heterogeneity of regional cerebral hemodynamics in patients with a symptomatic ICA occlusion. In patients with leptomeningeal collaterals, the most impaired region was found in the frontal lobe.
Footnotes
J. Hendrikse was supported by a grant 916-76-035 from the Netherlands Organization for Scientific Research.
References
- Received January 31, 2008.
- Accepted after revision June 2, 2008.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cerebral Perfusion After Repair of Congenital Diaphragmatic Hernia with Common Carotid Artery Occlusion After ECMO Therapy
- Noninvasive Evaluation of CBF and Perfusion Delay of Moyamoya Disease Using Arterial Spin-Labeling MRI with Multiple Postlabeling Delays: Comparison with 15O-Gas PET and DSC-MRI
- Arterial Spin Labeling Magnetic Resonance Imaging Estimation of Antegrade and Collateral Flow in Unilateral Middle Cerebral Artery Stenosis
- Regional Cerebral Arterial Transit Time Hemodynamics Correlate with Vascular Risk Factors and Cognitive Function in Men with Coronary Artery Disease
- Cerebrovascular Collaterals Correlate with Disease Severity in Adult North American Patients with Moyamoya Disease
- Hemodynamic Alterations in Vertebrobasilar Large Artery Disease Assessed by Arterial Spin-Labeling MR Imaging
- Assessment of Cortical Hemodynamics by Multichannel Near-Infrared Spectroscopy in Steno-Occlusive Disease of the Middle Cerebral Artery
- Systematic Review of Methods for Assessing Leptomeningeal Collateral Flow
- Cerebral Perfusion Long Term after Therapeutic Occlusion of the Internal Carotid Artery in Patients Who Tolerated Angiographic Balloon Test Occlusion
- Multiple Inflow Pulsed Arterial Spin-Labeling Reveals Delays in the Arterial Arrival Time in Minor Stroke and Transient Ischemic Attack
- Noninvasive MR imaging of cerebral perfusion in patients with a carotid artery stenosis
- Simultaneous Measurement of Arterial Transit Time, Arterial Blood Volume, and Cerebral Blood Flow Using Arterial Spin-Labeling in Patients with Alzheimer Disease