
Abstract
SUMMARY: Palatal involvement in chronic lymphocytic leukemia (CLL) is rare and has only been reported 3 previous times in the non-radiology literature. To our knowledge this is the first imaging description of this entity. Based on our experience, when smoothly lobulated, homogeneous masses are identified on the oral surface of the hard palate, the diagnosis of CLL should be considered.
Chronic lymphocytic leukemia (CLL) is a B-lineage neoplasm of prefollicular center cells that is usually associated with circulating neoplastic small lymphocytes. From a morphologic and immunophenotypic perspective, the malignant cells of CLL are identical to those of nodal-based small lymphocytic lymphoma (SLL), and these 2 malignancies are thought to represent different manifestations of the same disease.1 CLL is the most common type of leukemia in the Western hemisphere; its prevalence in Europe and America ranges from 29% to 38% of all leukemias. Ninety percent of patients with CLL are older than 50 years of age.2 The most common oral manifestations of the leukemias are gingival hypertrophy, petechial hemorrhage and ecchymosis, infection, ulceration, and necrosis. Less commonly, as a result of leukemic infiltrates, multiple localized tumorlike growths can occur in the gingiva.3 Similar localized leukemic infiltrations occurring elsewhere in the oral cavity have only rarely been reported in the literature.3–5 In this article, we report on a patient with CLL who presented with bilateral masses on the oral surface of the hard palate. This represents only the fourth such reported case and the first documented with imaging.3–5
Case Report
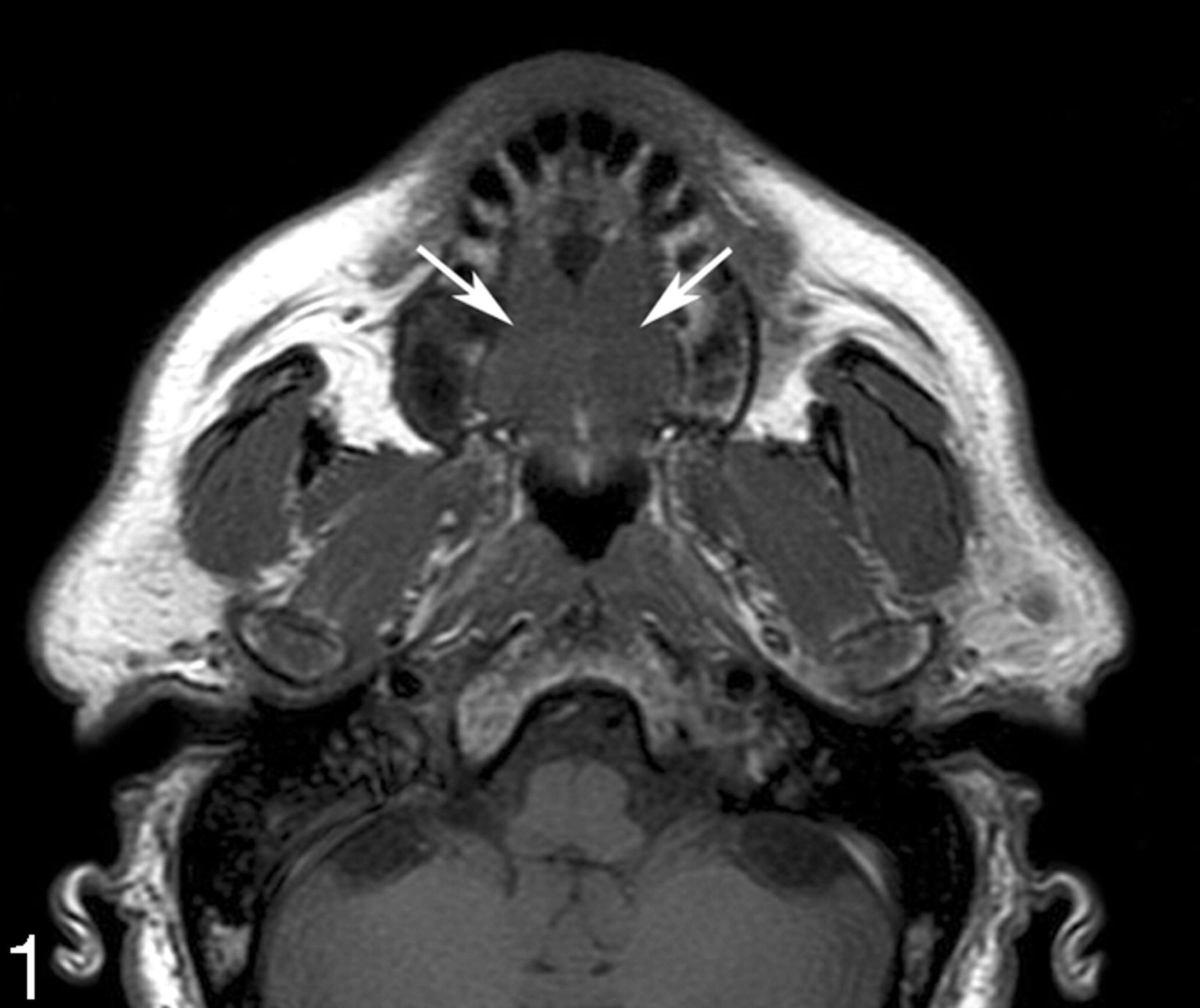
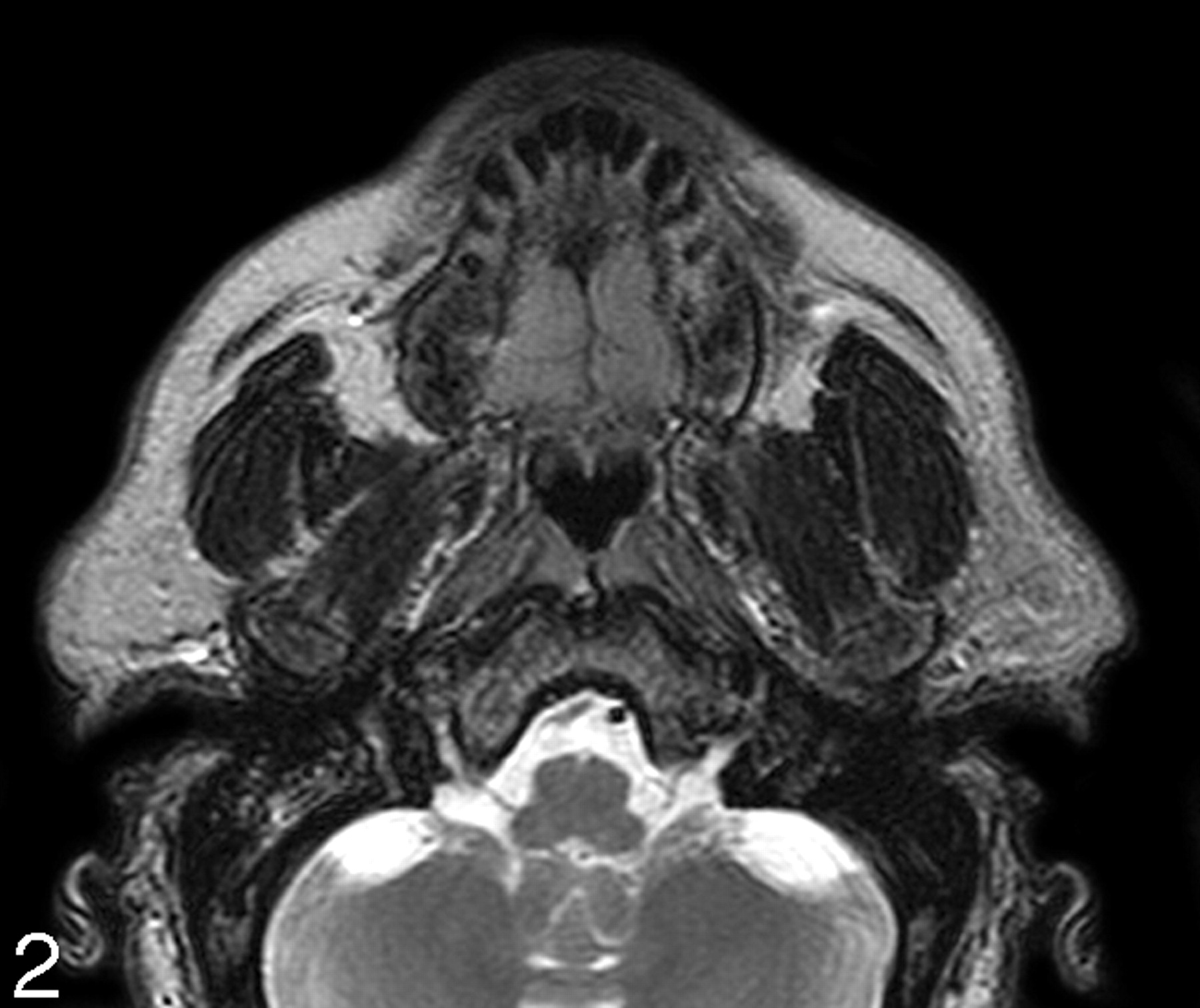
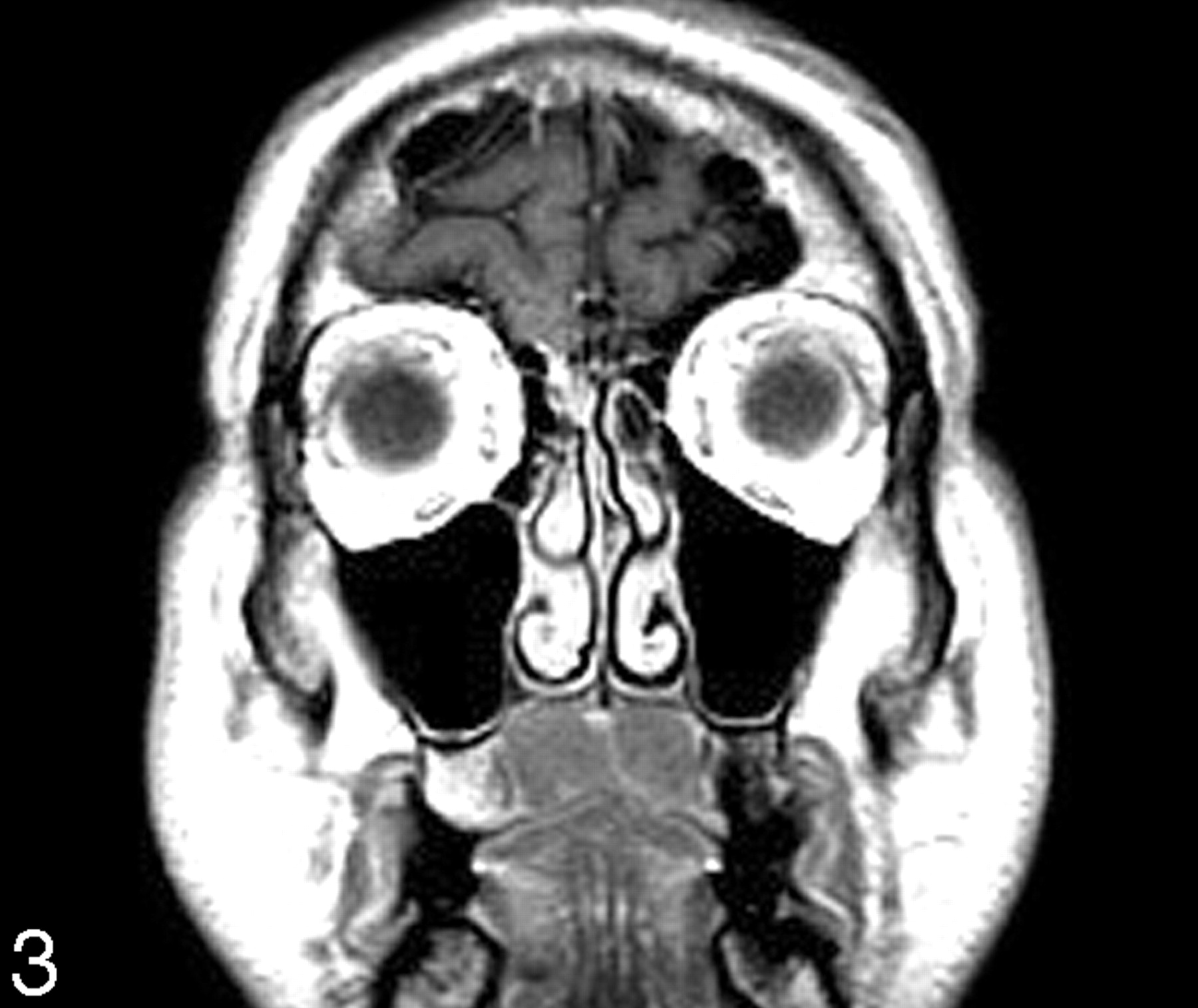
A 62-year-old man presented with a 3-week history of bilateral neck fullness and a mass in his palate. He had no pertinent prior medical history. Physical examination showed bilateral multiple nontender lymphadenopathy and a large firm palatal mass with a midline ridge. Blood work revealed leukocytosis and he was diagnosed as having chronic lymphocytic leukemia, stage 1. MR imaging showed smoothly lobulated soft tissue masses confined to the oral surface of the hard palate on either side of the midline. Compared with the skeletal muscle, the masses had overall intermediate T1-weighted (Fig. 1) and moderately high T2-weighted (Fig 2) signal intensity and enhanced uniformly (Fig 3). The patient also had diffuse homogeneous discrete lymphadenopathy. At this time, he is being clinically watched for any progression of disease, which would signal the initiation of appropriate therapy.

Axial T1-weighted MR image shows nodular soft tissue masses (arrows) of low-intermediate signal intensity along the oral surface at the level of hard palate.

Axial T2-weighted MR image shows that the masses have an intermediate signal intensity that is higher than in Fig. 1. The smoothly lobulated nature of the masses with a midline cleft can be well appreciated.

Coronal contrast enhanced T1-weighted MR image shows uniform enhancement of the masses confined to the oral surface of the hard palate with an incomplete midline furrow.
Discussion
The leukemias are divided into acute and chronic forms based on their clinical course, and the cell line involved further classifies them into myelocytic and lymphocytic types. The immunologically incompetent small neoplastic lymphocytes replace the bone marrow and infiltrate lymph nodes and various organs. The marrow replacement leads to a gradual loss of other cell lines, which manifests clinically as malaise (anemia), hemorrhage (thrombocytopenia), and infection (loss of competent white blood cells). The recirculating neoplastic lymphocytes, which make up more than 90% of the peripheral blood white cell count, infiltrate and enlarge the lymph nodes and visceral organs.4
The most common oral manifestations in leukemia, in order of frequency, include gingival hemorrhage, mucosal ulcers, infections, and gingival hyperplasia in tooth-bearing areas.6 Tooth loosening can occur from loss of the periodontal membrane. Leukemic infiltration of the tonsils and salivary glands can lead to their enlargement.4 In the head and neck, CLL most commonly presents as diffuse lymphadenopathy, often with quite large nodes. The oral manifestations of the chronic leukemias are less common than those associated with the acute leukemias.3, 5 In turn, the oral manifestations associated with CLL are the least common of all the chronic leukemias.
Palatal enlargement secondary to leukemic infiltration is rare. To our knowledge, there are only 3 prior, similar cases in the English language literature; none had CT or MR imaging studies.3–5 In these 3 prior patients, as with our patient, the palatal swelling was a painless, soft to firm, lobular mass with an overlying intact mucosa and an incomplete midline furrow. The relatively symmetric configuration of this process makes other palatal masses such as squamous carcinoma and minor salivary gland tumors quite unlikely.
Benign follicular lymphoid hyperplasia (FLH) affecting the oral surface of the hard palate is morphologically identical and, therefore, confusing in appearance and presentation. FLH in this location may present as a slowly growing, smoothly lobulated submucosal mass. Associated multicentric oral lesions and lymphadenopathy may also be present. Because isolated palatal enlargement can be the presenting feature of both CLL and FLH, and because FLH can recur after excision, it is important to distinguish these entities through pathologic examination.4, 7 Unlike CLL, which is a monoclonal leukemic infiltrate, FLH is characterized by an attenuated follicular lymphoid infiltrate within the lamina propria, replete with germinal centers.7, 8 These patients with either CLL or FLH palatal disease are typically asymptomatic for the palatal enlargement, except for ill-fitting upper dentures.4, 8,9
Other diagnostic considerations should include lymphomas of all grades, whether primary nodal or extranodal.4, 7, 9 Even though palatal involvement by lymphomas can present as soft, nontender, bilateral palatal swellings, in many cases, the palatal disease is unilateral, hard, painful, and accompanied by bone destruction.7 The final diagnostic differentiation between CLL, FHL, and the lymphomas can only be accomplished by pathologic examination.
Although a variety of other lesions (such as minor salivary gland neoplasms, torus palatinus, and infections and abscesses) can affect the hard palate, they are easily distinguished clinically and histologically from CLL.7
No prior description of the imaging findings of palatal involvement in CLL is available in literature. In our case, the MR imaging showed smoothly lobulated, uniformly enhancing soft tissue masses on either side of the midline confined to the oral cavity surface of the hard palate. There was overall intermediate T1-weighted and moderately high T2-weighted signal intensity (compared with skeletal muscle). These signal intensities are nonspecific with regard to the cell type that composes the mass. However, they suggest that this is not an inflammation-related process, because these latter conditions usually have higher T2-weighted signal intensities. In addition, the patient had the typical diffuse lymphadenopathy associated with CLL.10 The imaging findings correlated well with the clinical description of this lesion found in the literature.3–5
Summary
Palatal involvement in CLL is rare and has only been reported 3 previous times in the nonradiology literature. To our knowledge this is the first imaging description of this entity. Based on our experience, when smoothly lobulated, homogeneous masses are identified on the oral surface of the hard palate, especially in a patient who has a diffuse lymphadenopathy, the diagnosis of CLL should be considered.
- Received April 14, 2005.
- Accepted after revision September 30, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.