
Abstract
Summary: Astrocytoma, or pituicytoma, of the posterior pituitary is a relatively rare entity consisting of poorly characterized glial tumor cells. We report two cases of posterior pituitary astrocytomas in middle-aged women presenting as focal lesions of the neurohypophysis. A review of the literature reveals only a few reports of this tumor, and there has been scanty discussion of the imaging findings of posterior pituitary astrocytomas compared with lesions of the anterior pituitary gland. This report reviews the clinical characteristics and imaging findings and discusses the differential diagnosis of these two cases.
The pituitary gland is unique because of its dual embryologic cell lineage. Both components of the gland are contained in the same anatomic compartment but differ in many respects. The anterior pituitary, as well as the pars intermedia and pars tuberalis, originates from the primitive stomodeum, which ascends cranially to the sell turcica. It also contains neuroectodermal derivatives. The neurohypophysis, or posterior pituitary, is an inferior extension of the hypothalamus, which descends to lie in close proximity to the anterior pituitary. The cellular composition of the neurohypophysis is that of specialized glial cells (pituicytes) together with their axons. Although the anterior lobe completely loses its connections with the primitive nasopharynx, the posterior lobe maintains its relationship with the hypothalamus throughout life. On the basis of these facts, it is understandable that the hypophyseal stalk or posterior pituitary can be a host to all the neoplastic processes that originate from the glial cell series.
Case 1
A 36-year-old female patient presented with uncontrollable chronic headaches and amenorrhea. The clinical examination did not reveal any abnormality. Laboratory tests revealed mild prolactinemia. On MR imaging, a posterior pituitary mass, isointense on T1-weighted images (T1WI) and hyperintense on T2-weighted images (T2WI), was identified, without significant involvement of the stalk. Postcontrast scans showed attenuated heterogeneous enhancement of the mass. The patient underwent trans-sphenoidal surgery (TSS), with some residual tumor being seen on postoperative imaging. A progressive increase in the bulk of the residual tumor was noted on follow-up MR examinations during the next 5 years. The imaging study performed before this admission demonstrated a bulky pituitary mass, as well as a bulky stalk with suprasellar extension and attenuated nonhomogenous enhancement. In the meantime, she also had developed fatigue and unbearable headaches. The patient underwent a second TSS, and histology of the specimen revealed neoplastic proliferation of astrocytes and spindle-shaped cells with fascicles. The nuclei had generally maintained their ovoid shapes, with stippled to hyperchromatic chromatin and fusiform piloid cytoplasm. There were foci of eosinophilia, stellate cytoplasm, and occasional gemistocytic morphology, and many cells were positive for glial fibrillary acidic protein (GFAP). There was no significant mitotic activity. This histology was interpreted as consistent with a posterior pituitary astrocytoma.
Case 2
A 45-year-old female patient presented with uncontrollable chronic bitemporal, occipital, and frontal headaches. She also complained of nausea and episodes of blurry vision. Neurologic examination was normal. The MR imaging revealed a small pituitary mass with suprasellar extension, isointense on T1WI and slightly hypointense on T2WI. Postgadolinium-enhanced scans demonstrated nonhomogeneous enhancement. This mass was resected via a transspenoidal approach, and histology revealed a moderately cellular astrocytomas with compact fibrillated cells in a fascicular pattern. GFAP highlighted the fibrillary aspect. This was also interpreted as consistent with a posterior pituitary astrocytoma.
Discussion
The anterior and posterior lobes constitute 2 distinct parts of the pituitary gland and have distinct embryologic backgrounds. The posterior pituitary, being part of the neurohypophysis, harbors specialized glial cells named “pituicytes.” They are modified glial cells of empendymal cell lineage located in the neurohypophysis and pituitary stalk. Five different types of pituicytes have been identified on the basis of their cytoplasmic characteristics (1), and attempts are presently underway to characterize and classify each type as a progenitor of a separate type of neurologic tumor. The cell types are as follows (2, 3):
Major cells: These cells contain electron lucent cytoplasm with oval or irregular nuclei. There are distinctive nucleoli and variable numbers of organelles.
Dark cells: These cells have the same ultrastructure but with an electron-attenuated matrix. Most pituicytomas are believed to arise from the two cell types mentioned above.
Oncocytic cells: These cells have a high mitochondrial content.
Ependymal cells: These cells show rudimentary ependymal patterns.
Granular cells: These cells contain numerous electron-attenuated granules, which are periodic acid shift–positive and are otherwise known as brown cytoplasmic cells. It is believed that they give rise to granular cell tumors or choristomas (4).
Although sometimes clinically indistinguishable from other tumors of the region, pituicytomas are histologically distinctive because of the spindled appearance of the cells on light microscopy as well as lack of immunoreactivity for neuroendocrine markers and pituitary hormones. In the largest series of these tumors, reviewed by Brat et al (5), most pituicytomas of the posterior pituitary have been found to demonstrate the presence of GFAP immunoreactivity as well as intermediate filaments on ultrastructural analysis.
Although much rarer than the tumors of the adenohypophysis, commonly described posterior pituitary tumors include metastases, choristomas, hamartomas, craniopharyngiomas, germinomas, gangliogliomas, teratomas, schwannomas (6), and astrocytomas. The tumor previously described as a pituitary myoblastoma is now considered to have been inappropriately identified, because no myoblasts are present in the pituitary gland. Choristoma is also probably a misnomer, this term being more appropriate for granular cell tumors found outside the pituitary. The term has been largely replaced by granular cell tumor, on the basis of a microscopic picture of cytoplasm, which is rich in granules (4). Needless to say, adenoma still remains the most common tumor of the pituitary gland as a whole. Tumors of the posterior pituitary should always be considered in the list of differential diagnosis in an appropriate clinical setting with suggestive imaging features. Because of their rarity, it is difficult to ascertain the exact incidence of these tumors. The usual presentation is that of a young to middle-aged woman with signs of an intracranial focal lesion causing headaches and endocrine hypofunction. Visual symptoms as a result of compression of the optic chiasm are probably less common because of the anatomic location of the mass in the posterior pituitary. They may also be asymptomatic and discovered incidentally.
MR imaging findings are usually that of a focal well-circumscribed solid posterior intrasellar mass with suprasellar extension without a bulky pituitary stalk. These masses usually manifest with low signal intensity on T1WIs, low to intermediate intensity on T2WIs, and fairly homogenous enhancement on postcontrast T1WIs. Meticulous attention to the posterior pituitary is the key to diagnosing these rare tumors, and the orientation and bulk of the stalk should be carefully assessed.
Contrast-enhanced CT probably has little role in imaging of the pituitary astrocytoma unless MR is contraindicated. Pituitary astrocytoma is a distinct and important entity to be considered in the differential diagnosis of posterior pituitary masses. Radiologic/pathologic correlation is critical. It is important that a precise histologic diagnosis be established by immunohistochemistry and electron microscopy as cure can be achieved by means of total excision, whereas, if untreated, these tumors can grow to become extremely large.
- Received April 21, 2004.
- Accepted after revision September 17, 2004.

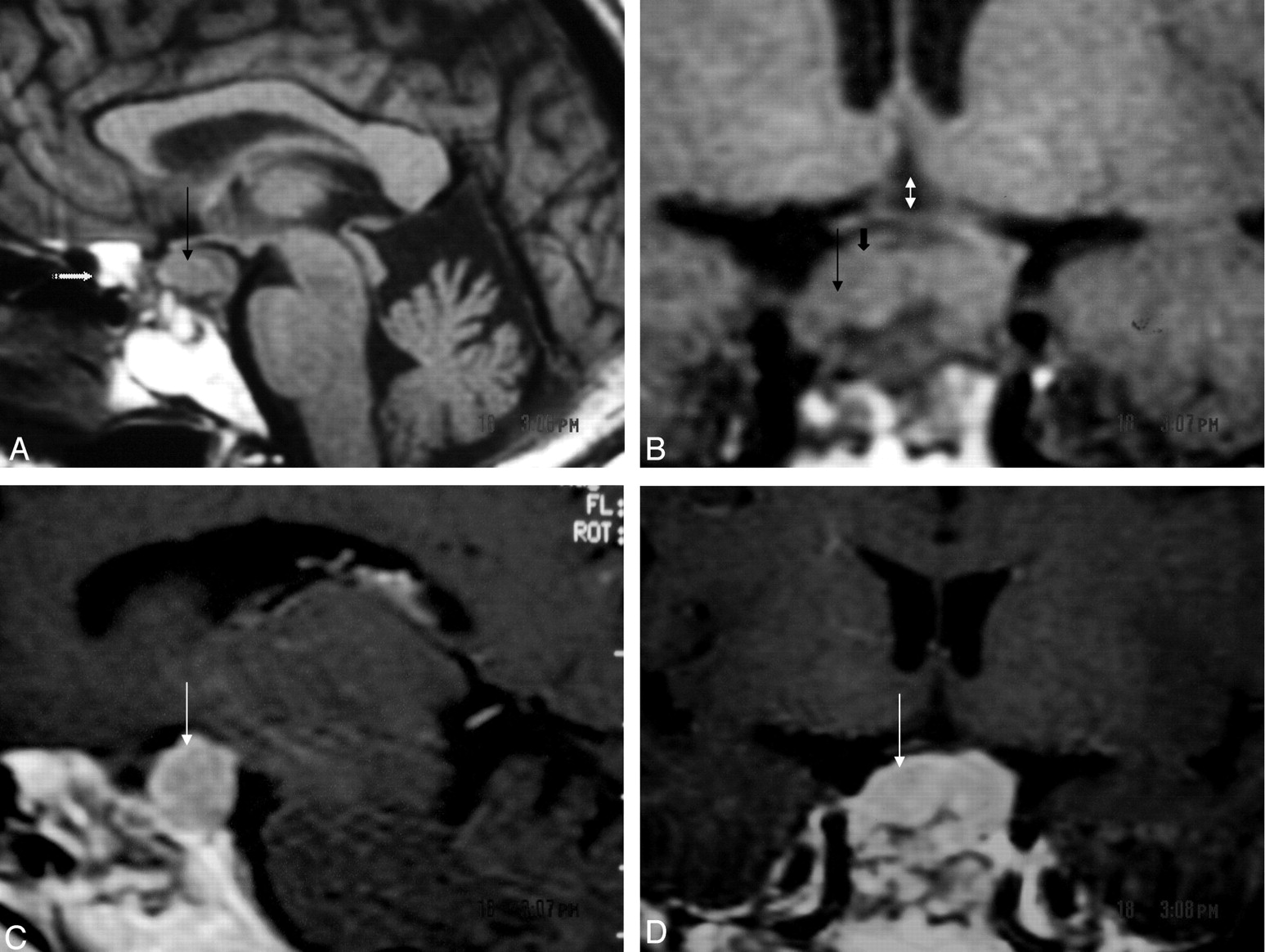
Case 1, a 32-year-old woman with chronic headaches and amenorrhea.
A, T1-weighted (TR, 760; TE, 15) sagittal MR demonstrating an intrasellar tumor with suprasellar extension (thin black arrow). There is evidence of previous surgery, as seen by fat packing in the sphenoid sinus (stippled white arrow).
B, T1 weighted (TR, 760; TE, 15) coronal MR showing the sellar mass (thin black arrow) with suprasellar extension (short black arrow) of tumor causing chiasmal (double-headed white arrow) compression.
C and D, T1-weighted contrast-enhanced sagittal and coronal MR showing dense heterogeneous enhancement of the tumor (thin white arrow).

Case 1.
A, Histology with H & E stain and 100× magnification reveals a tumor composed of spindle-shaped cells with elongated nuclei arranged in fascicles. Focal infiltrates of mature lympocytes are present.
B, Although Rosenthal fibers were not observed, hyaline bodies were focally seen (upper left).

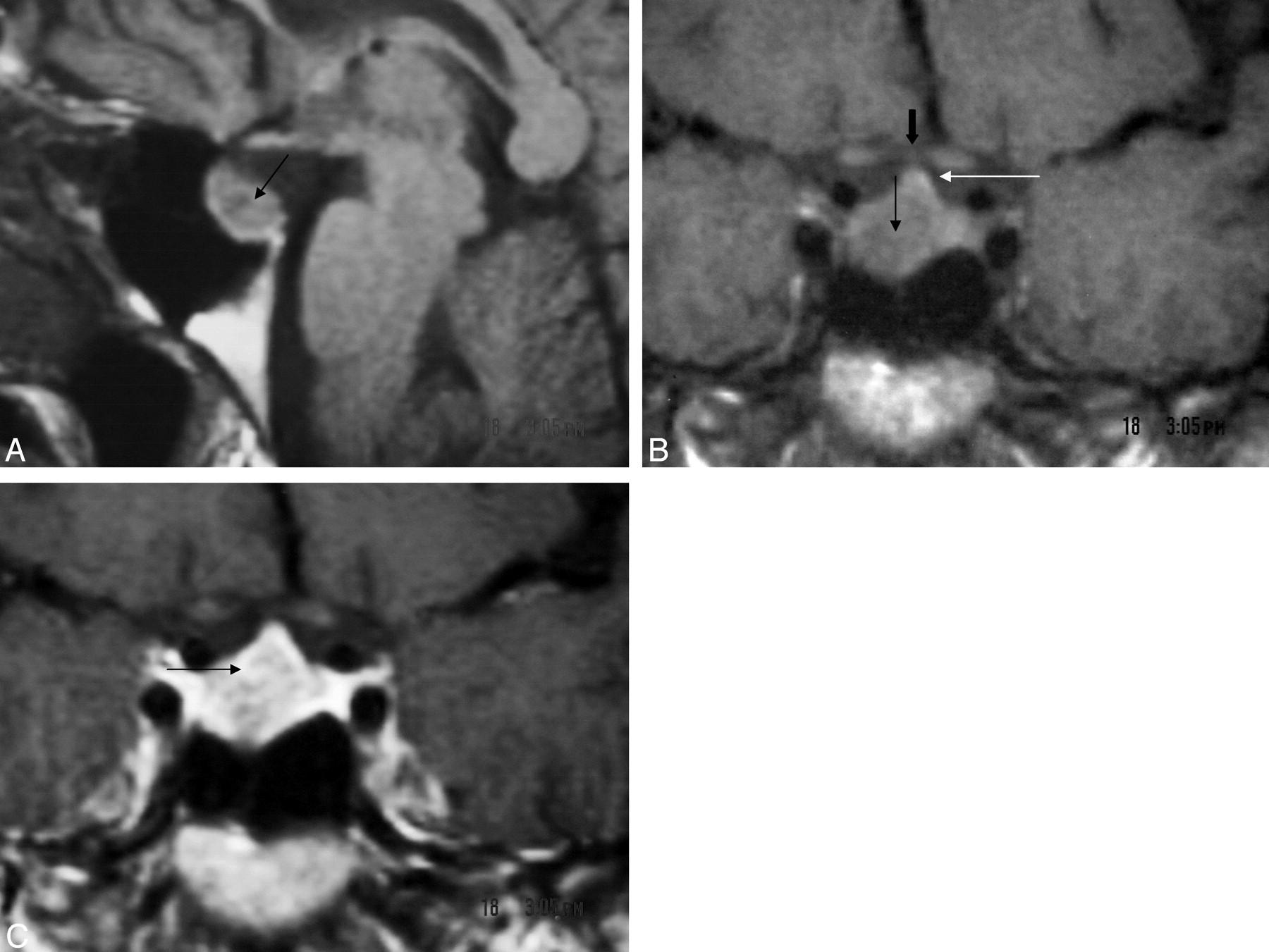
Case 2, a 45-year-old woman with uncontrollable chronic headaches.
A, T1-weighted coronal MR demonstrates suprasellar extension of the mass (thin black arrow), pituitary stalk (thin white arrow), and optic chiasm (bold black arrow).
B, T1-weighted (TR, 760; TE, 15) sagittal MR showing an intrasellar mass (thin black arrow).
C, T1-weighted contrast-enhanced coronal MR shows dense nonhomogenous enhancement of the tumor (thin black arrow).

Case 2.
A, H & E stain and 100× magnification shows compact areas of spindle cells with oval to fusiform nuclei.
B, GFAP immunohistochemical (100× magnification) highlights the fibrillary cellular processes.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}