
Abstract
BACKGROUND AND PURPOSE: The dural sinus occlusion has been shown to be effective in the treatment of some dural arteriovenous shunts (DAVS). No long-term results are available, however, regarding the significance of occlusion of a dural sinus. If the disease will stop or if other events will occur later in the remaining sinuses are not well known yet. Careful analyses of our cases led us to discover that, in some instances, the shunt involves only a single portion or compartment of a sinus. In this report, we describe our results in the treatment of these lesions: occluding only the involved compartment while preserving patency of the remainder of the sinus and the angiographic signals, thus allowing diagnosis of the presence of a compartment.
METHODS AND RESULTS: From 1996 to October 2002, we found 12 cases of DAVS (among 40 news cases of DAVS) with two types of compartments—one inside the sinus, which we call “septation” (nine cases), and the other outside the sinus, which we call “accessory sinus” (three cases). It was possible to occlude completely the lesion superselectively in nine cases. In two cases, it was necessary to occlude the entire sinus secondarily, and in one case the sinus was occluded because was impossible to catheterize the septation. Two cases with recanalization on the control were treated by additional arterial and arterial and venous approach.
CONCLUSION: It is very important to diagnose the presence of a compartment in dural arteriovenous shunts during the diagnostic angiography. In most cases, it allows curative treatment of the lesion by occluding only the compartment while preserving patency of the remainder of the sinus.
The first published case of transvenous approach to occlude a carotid-cavernous fistula was performed at our institution in March 1983 (1). After that, we have treated some cavernous sinus dural arteriovenous shunts (DAVS) by venous approach throughout the superior ophthalmic vein (by surgical dissection and, more recently, by femoral-facial vein catheterization) and throughout the inferior petrosal sinus. After 1995 we began to treat widespread DAVS located on the lateral and sigmoid sinuses by venous approach, occluding the diseased part of the sinus after a careful analysis of the normal brain venous drainage with detachable platinum coils, as described elsewhere (2). This technique was later employed to treat DAVS in other locations (3, 4).
The therapeutic occlusion of dural sinuses is efficient but very expensive when necessary to occlude a large segment of the sinus. Another question concerns what will happen to the other sinuses over the long term. Another dural shunt can develop later, or thrombotic phenomena can occur.
This practice led us to discover in 1996 our first case of a dural sinus compartment, and it was occluded superselectively by using detachable coils with cure of the lesion, preserving the sinus lumen. Fewer coils are necessary to occlude the compartment than would be used to occlude the entire sinus.
Here we describe the two types of compartments we found in our 12 cases of compartments in DAVS, the angiographic signals to identify them and the results of the superselective transvenous dural sinus occlusion treatment.
Patients and Techniques
Our study is based on 213 adult patients with 220 DAVS studied angiographically at our institution by the same staff between November 1986 and October 2002. DAVS in children were excluded from this study. The decision of the treatment strategy was made by us in 123 patients with the following approaches: arterial, 70; arterial and venous, 9; venous, 20; venous superselective, 12; arterial and surgery, 3; surgery, 6; radiosurgery, 3.
The diagnostic angiographic study in cases of DAVS included injections in internal carotid arteries (ICAs), vertebral arteries (VAs), and selective catheterization of branches of both external carotid artery (ECA) and injection in the common carotid artery (CCA) on the same side of the lesion. Since 1995, with the introduction of the venous approach to treat lesions in sinuses other than the cavernous sinus, we began to superpose the early arterial phase with the full venous phases of the CCA angiogram (Fig 1E). Another procedure is to compare the arterial phase of the ECA with the venous phase of the ICA in the same projection. Oblique views were included systematically in our protocol after 1996 and have been performed in the best feeder to disclose the dural sinus compartment from the normal sinus (Fig 2B).


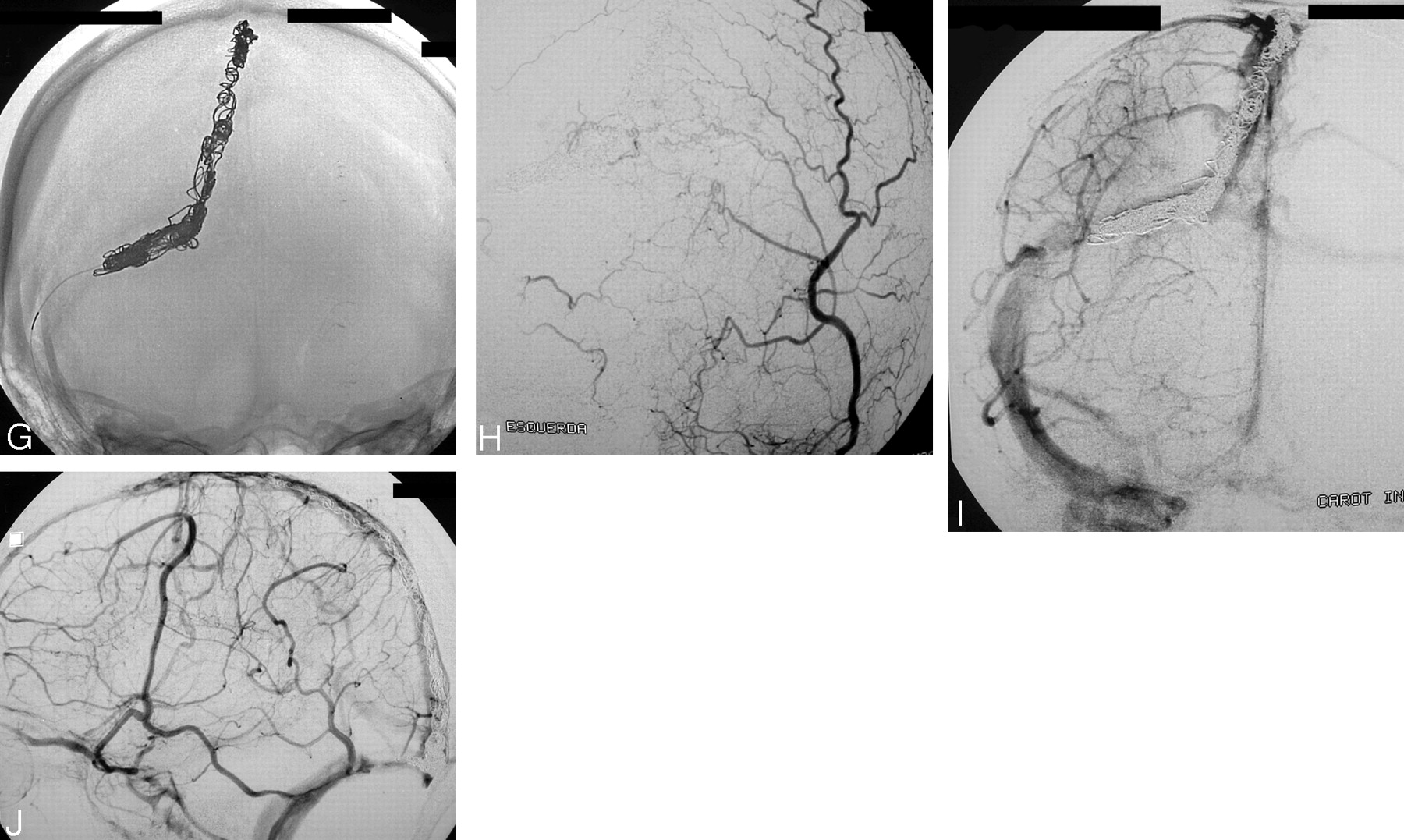
Case 4.
A and B, Right ECA and left occipital artery injections in AP view, showing DAVS in the superior sagittal sinus (SSS) and right transverse sinus (TS). Partial opacification of these sinuses is shown (arrows).
C and D, Right CCA angiograms, in arterial (C) and venous phase (D). In panel C, the arrow indicates a early partial filling of the SSS and right TS. In panel D, the arrow indicates a nonopacified area of these sinuses.
E, Superposition of the arterial and venous phases of the right CCA injection, showing in black the shunt and in white the normal venous drainage of the brain.
F, Injection into the septation (black) during the venous phase of the right ICA.
G, Conventional radiographic image, showing coils into the septation.
H, Left occipital artery injection in AP view posttreatment, showing complete occlusion of the shunt.
I and J, AP and lateral view (venous phase) of the right ICA angiogram, showing patency of the SSS and right TS.

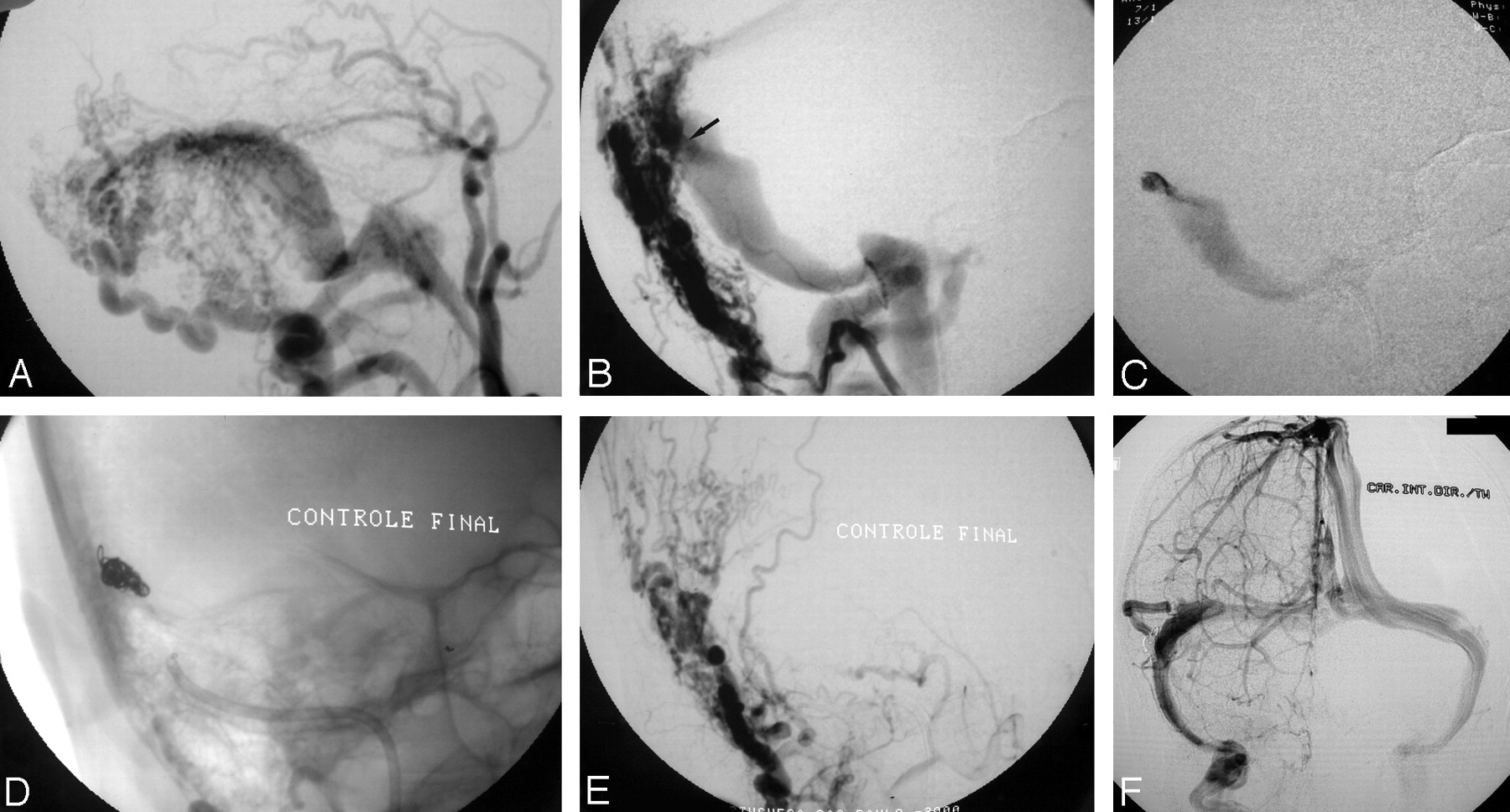
Case 2.
A, Right ECA in lateral view shows a DAVS in the distal transversal sinus. Note the convergence of the feeders toward a point.
B, Right occipital artery injection in oblique view shows the shunt is located only over an accessory sinus that has a “tubular hyperdensity” (arrow).
C and D, Superselective injection (C) and coil occlusion (D) of the dural sinus compartment.
E and F, Right occipital and right ICA angiograms, showing complete occlusion of the DAVS, while preserving patency of the lateral and sigmoid sinuses.
Angiographic Technique.
The diagnostic angiographic study is done by use of general anesthesia in all patients; we have a suspicion of this diagnostic on the basis of other studies (CT or MR). It is very important to have images without movement artifacts, because we need to inject ECA branches and have the same projection for different arteries to be able to compare and superimpose the images. Careful analysis of venous phases is very important to plan the treatment. We use always a transfemoral approach to these studies.
Technical Aspects of the Treatment
The embolization procedure is done under general anesthesia, by approaching the jugular vein with a 5F guiding catheter introduced throughout the right common femoral vein. The angiographic controls are done by a 5F diagnostic catheter (vertebral catheter; Cordis Endovascular, Miami Lakes, FL), introduced throughout the left femoral artery and positioned in the artery that gives the best visualization of the compartment. Depending on the situation, injections in the ICA are done to control the normal vein and sinus. A bolus of 5,000 IU of heparin is administrated intravenously after the arterial and venous punctures and reinforced if the procedure is longer than 2 hours. The heparin is discontinued after completion of the procedure, and no antiplatelet drug is used in these cases. For catheterization of compartments, we use regular microcatheters and microguidewires (Excel 14, Boston Scientific, Fremont, CA; and Rebar 14 with Silver Speed 14, Dendron-MTI, Bochum, Germany), as used in aneurysm treatment. The follow-up of the treatment is done by angiography in our department, in all cases with gentle sedation.
We attempt to occlude the entire septated area, starting with the most proximal part of the sinus by using small, soft coils. Because the distal extremity of the septation (distal part of the sinus) can become larger, we often have to use larger coils. The DAVS can extend to outside of the septation or accessory sinus (cases 7 and 8, respectively [Table 1]) and total occlusion of the sinus could be necessary. In other cases, the embolization had to be completed by arterial approach. In some accessory sinuses, the channel containing the shunt is very short, and it is better to use soft coils to do a compact cast of coils to achieve total occlusion (Fig 2D).
Summary of patients with superselective transvenous embolization of compartment
From 1996 to October 2002, we have studied 40 patients with DAVS and found a dural sinus compartment in 12 of them (30%). The dural sinus compartment corresponds either to an arteriovenous (A-V) shunt that is restricted to a part of the dural sinus, which we will call “septation” and found in nine of our cases, or to an A-V shunt restricted to a venous channel located outside the sinus, which we call “accessory sinus” and found in three of our cases.
Patients included six women and six men and their ages ranged from 23 to 76 years, with a mean of 48 years. Pulsated tinnitus was the most frequent symptom, present in 10 patients. One patient presented with headache and coma, and the other patient developed unilateral exophthalmia and chemosis.
The first choice of treatment in these cases was super-selective trans-venous dural occlusion, by using electrically detachable coils (Guglielmi detachable coils in most cases).
Results
Angiographic Findings
As a rule, we make injections in the CCA, a global injection at the origin of the ECA, and, afterward, selective injections in occipital, ascending pharyngeal arteries, and distal ECA, as well as in the ICA and VA in the same anteroposterior (AP) and lateral view on the side of the lesion. Contralateral arteries are injected in the AP view. We superimpose the arterial with the venous phase of the CCA injection to analyze the normal brain venous drainage and the drainage of the shunt.
Additional oblique views will be done when any angiographic signal intensity suggesting a dural sinus compartment is found, to separate the shunt from the sinus (Figs 2A and B). The angiographic signals of dural sinus compartment include the following:
Convergence of the feeders—The multiple meningeal feeders are converging toward a point (Fig 2A). This is easily identified in the early arterial phase of the angiogram. It is found in both types of dural sinus compartment.
Partial opacification of the sinus—This angiographic signal appears in the very early arterial phase of the angiogram, when the opacification of only a part of the sinus is seen (Figs 1A, -B, and -C). Full opacification of the sinus can occur in the following frames (this and the next two signals occur in cases of “septation”):
Nonopacified area of the sinus—This occurs in the venous phase of the normal brain drainage. The normal brain drains around the septation as a separate structure into the same sinus where the shunt is (Fig 1D). There is no mixture between the compartments. In the arterial phase of the CCA injection, we have the opacification of the part of the sinus with the shunt (Fig 1C), and during the venous phase, this part is not opacified (Fig 1D). Superposing the arterial phase with the venous phase of the CCA angiogram (Fig 1E), we can see that the septated part of the arterial phase corresponds exactly to the nonopacified area of the venous phase.
Septation—This is a line inside the sinus, identified in the arterial phase, when the entire sinus is opacified (Fig 3A). The visualization of the septation depends on its position in relation to the radiographic beam.

Case 3.
A, Left CCA angiogram shows DAVS in the SS. Arrow shows a line, which corresponds to a septation.
B, Left occipital artery angiogram after superselective transvenous dural sinus occlusion, showing complete occlusion of the shunt.
C, Venous phase of left ICA angiogram in lateral/oblique view showing coils in the septatio, and preservation of the lumen of the SS.
Tubular hyperdensity—This is an area of hyperdensity created by superimposition of the accessory sinus over the normal sinus (Figs 2B and 4A). This signal intensity appears in cases of “accessory sinus.”

Case 1.
A, Right ascending pharyngeal artery angiogram in AP view: DAVS in the foramen magnun region, draining retrogradely toward inferior petrosal sinus and sylvian superficial vein and toward the jugular bulb. Arrow shows hyperdensity.
B, Left ascending pharyngeal artery angiogram in AP view shows that the shunt is located over an accessory sinus.
C, Left ascending pharyngeal artery angiogram in AP view after superselective transvenous dural sinus occlusion, showing complete occlusion of the shunt.
D, RICA angiogram in venous phase, in AP view, showing patency of the normal sinuses.
Special angiographic maneuvers: oblique view—After the identification of the signals described above, oblique view will help to disclose the compartmentalization of the DAVS by separating the shunt from the sinus (Fig 2B); contralateral branches of the ECA—In the lesions close to the midline the selective injection of branches of the contralateral ECA in AP view is particularly helpful. The shunt is clearly identified through collaterals that cross the midline (Fig 4B). In these cases, the homolateral ECA branches frequently hide the exact point of the shunt and give an unreal wider aspect of it (Fig 4A). In fact, the shunt is restricted to a small part of the sinus wall, and a careful analysis of the angiogram is necessary to disclose these cases of dural sinus compartment.
Rapid angiographic series—To better evaluate the very early arterial findings, we have been doing fast angiographic sequences of 3–7 frames/s.
Intracompartment injection—An intracompartment injection can clearly demonstrate cases of dural sinus compartment. In cases of accessory sinus it is evident that we are outside the sinus (Fig 2C). In cases of septation, the contrast does not fill all width of the sinus (Fig 1F). The limit of the septation can be determined when all width of the sinus becomes opacified by the contrast. This determines the part of the sinus to be occluded.
Table 1 summarizes the location of the DAVS, types of compartment, treatment, result, numbers of coils used, and follow-up of the 12 cases of dural sinus compartment in this series.
Anatomic cure of the lesions was achieved in all patients. We did not have any complication in these cases. In nine patients, the cure was achieved with superselective transvenous dural sinus occlusion only. In two patients (7 and 8), it was necessary to occlude the sinus totally after superselective transvenous dural sinus occlusion—one with a septation and the other with an accessory sinus. In one case (11), it was not possible to catheterize the septation and the sigmoid sinus was completely occluded.
The number of coils necessary to occlude the lesion when superselective catheterization was possible was lower than we have to occlude completely the sinus, which is larger (cases 7, 8 and 11).
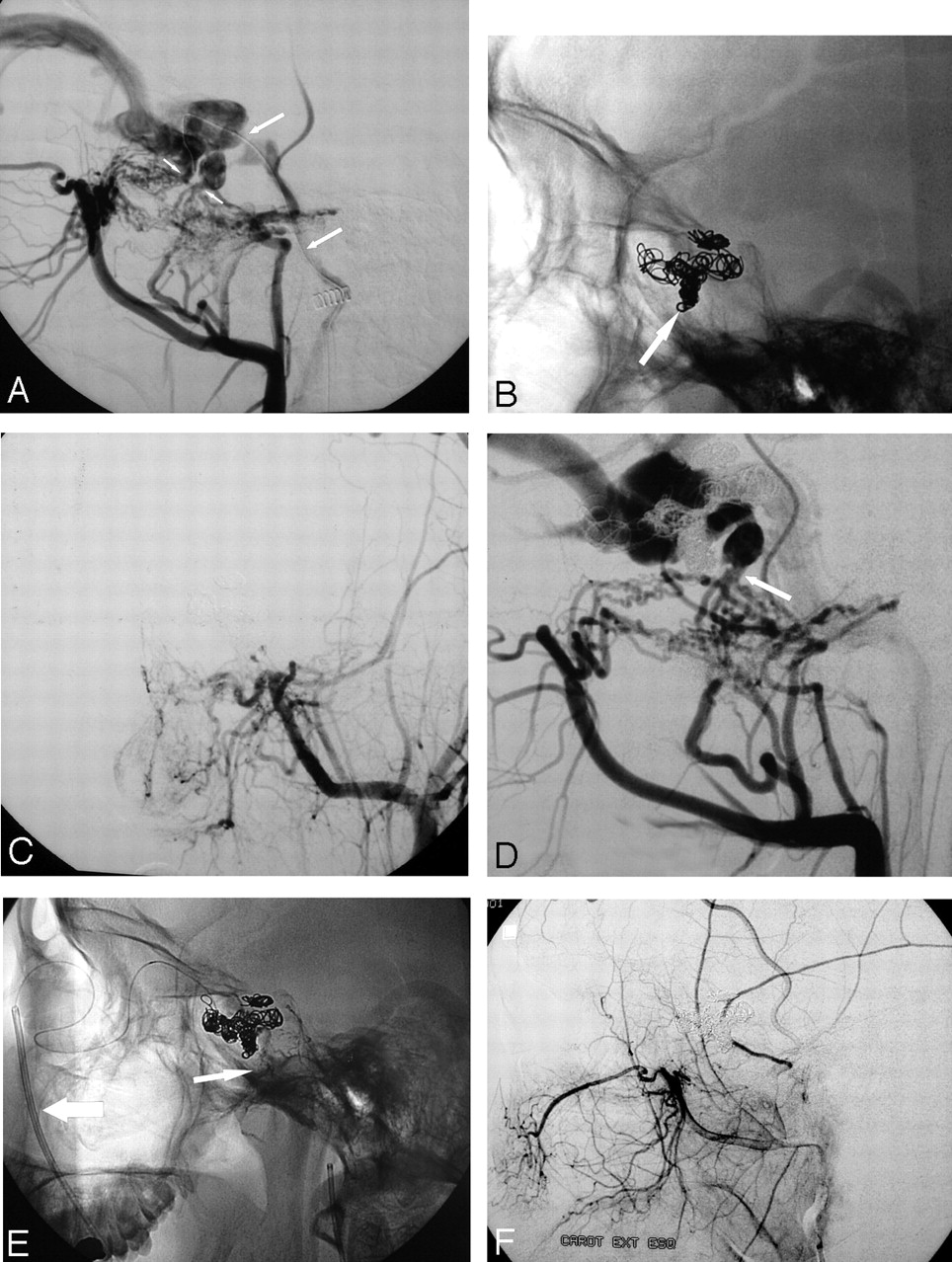
Recurrence of the shunt occurred in two cases of septation. One of them (case 9) was treated by additional arterial and venous approach, and the other (case 10) by additional arterial approach. In case 9, there were two different septations in the cavernous sinus, communicating with the rest of the sinus (Fig 5A). One septation could be catheterized superselectively and occluded completely. It was impossible to occlude superselectively the other septation, and we then performed the occlusion of a pouch continuous to it, preserving patency of the most part of the sinus (Figs 5B and -C). Recurrence of symptoms occurred 3 weeks after, and a new angiogram showed recanalization of this second septation; the other was occluded (Fig 5D). We tried—without success, because of an anastomosis—to treat it by glue injection in the accessory middle meningeal artery. Total occlusion was achieved by the transvenous approach: catheterization of cavernous sinus by a femoral to facial vein route, entirely occluding the cavernous sinus with coils (Figs 5E and -F).

Case 9.
A, Left ECA angiogram in lateral view. There is convergence of feeders toward two points of the cavernous sinus (small arrows). Long arrow is showing a microcatheter into the cavernous sinus (through the inferior petrosal sinus).
B, Conventional radiograph, showing high-density cast of coils into the most anterior septation (arrow) and low-density cast in a portion of the cavernous sinus.
C, Left ECA angiogram in AP view after embolization, showing total occlusion of the DAVS.
D, Left ECA angiogram in lateral view 1 month after embolization, showing recurrence of the shunt only in the posterior septation (arrow). There is no more drainage toward the inferior petrosal sinus.
E, Conventional radiograph at the end of the second session of embolization. Large arrow show 5F guide catheter into the facial vein (transfemoral approach). Arrow shows fragments of NBCA injected in the accessory meningeal artery.
F, Left ECA injection in lateral view after embolization, showing complete occlusion of the DAVS.
In case 10, a small shunt recurred on the outlet of the septation into the sinus and was treated with n-butyl 2-cyanoacrylate (NBCA) diluted to 20% injected in the meningeal branch of occipital artery, occluding totally the shunt. This patient moved to another city and could not come back for angiography in our institution. We have a report of another angiographic service performed at our institution, with total occlusion of the lesion and he was asymptomatic (without bruit).
Recurrence occurred in case 9 probably because there was not enough compaction of the coils, or perhaps secondary thrombosis of the cavernous sinus occurred during the procedure that was caused by lengthy manipulation of the microcatheter and microguidewire in the sinus. In case 10, recurrence was probably due to progression of thrombosis from the coils at the outlet of the septation. We stopped the procedure at this time to avoid thrombosis of the entire sinus.
Discussion
Dural sinus occlusion is a therapeutic option, achieving anatomic cure in some cases of widespread DAVS, if the number of feeders is large or unsuitable for embolization by arterial approach (5, 6).
On the other hand, the venous approach with occlusion of the compromised sinus carries some theoretic risk to the patient, who can develop other pathologies in the remaining sinus—thrombosis or a new DAVS. Venous sinus thrombosis is evidence of the pathophysiology of some dural shunts, as its etiology or natural evolution (7), and what will happen in the long term with the remaining “normal” dural sinus after endovascular occlusion of the diseased one is not well known yet. Will the endothelial cell dysfunction stabilize after the occlusion of the lesion? Will late recanalization of the occluded sinus occur? We have two cases with late recanalization. Will spontaneous thrombosis occur? Will the dysfunction progress with the development of a new shunt? As yet, there are no answers to these questions.
The concept of dural sinus compartment is a new angioarchitectural feature of the DAVS and should be known by the physicians implicated in the treatment of this disease, as the patency of the sinus can be preserved. We do not know the exact mechanism evolving the development of the compartments in DAVS. Even the exact etiology of most of DAVS is not yet known. We can only make some speculative suggestion about their physiopathology.
The compartment inside the sinus (“septation”) seems to be related or even generated by partial thrombosis of the sinus, where the AVS is established in the thrombosed segment after clot reabsorption and recanalization, creating a double channel (Figs 1 and 4). In some cases, the septation seems to be created after total sinus thrombosis and recanalization, which will create a sort of a tubular structure inside the sinus, with a very irregular wall. In most of the cases the septated area presented several trabeculae, which made it difficult to determine and catheterize its communication with the normal sinus (the entrance or exit of the septation), as in our case 11.
When the compartment is outside the sinus, the mechanism seems to be different and the shunt is established on a tubular structure communicating with the sinus, probably representing an accessory dural sinus (Figs 2 and 3). There was no angiographic evidence (collateral circulation or thrombophlebitic pattern of cortical veins in the region of the shunt) of a previous connection of these structures with pial veins. In our three cases of accessory sinus, there was neither reflux to pial or dural veins nor evidence of previous cortical vein thrombosis. There is also no evidence that these accessory sinuses communicated previously with extracranial veins, representing an emissary vein with their outlet thrombosed. The pathophysiology of these shunts is uncertain, as in other cases without evidence of previous venous thrombosis. Their origin is probably not similar to the so-called extra sinusal dural arteriovenous shunts but, rather, similar to the shunts occurring in the edge of the tentorium or in other places where there is embryologic sinus (8).
There is no clear description or reference to these architectural findings in literature, though some authors have published selective transvenous embolization and showed cases that clearly correspond to a septation or an accessory sinus. Mironov described two cases of selective trans-venous embolization of DAVS (9). His first case was a shunt located over a parasagittal vein, draining inferiorly in the superior sagittal sinus. His second case is clearly a case of an accessory sinus type of dural sinus compartment. He described that the “venous conduit” was the mastoid emissary vein, but this emissary vein is located more inferiorly. Other authors describe selective transvenous embolization of DAVS of the cavernous sinus as a partial occlusion of a partially thrombosed sinus.
Retrospectively, it is difficult to find other cases in our series, because the diagnosis of these lesions depends on the angiographic study, and, in most cases, we need oblique views to disclose the compartment (10; Fig 2B). After our first case, we systematically have been performing the angiographic study with oblique views and other maneuvers trying to make this diagnosis. We found a dural sinus compartment incidence of 30%, which is very high. As the treatment of such types of lesion is easier, safer, and less expensive, the interventional neuroradiologists have to be aware of the existence of this type of lesion, providing a better care to their patients.
Conclusion
We presented a new angioarchitectural feature of DAVS in adults, describing the angiographic signals and maneuvers that allow us to identify these lesions during the diagnostic angiographic study. The presence of a compartment allows us to occlude, in most of the cases, only the shunt, by using the superselective transvenous dural sinus occlusion, preserving patency of the sinus.
Footnotes
Presented in part at the 6th Congress of the Word Federation of Interventional and Therapeutic Neuroradiology, Seoul, Korea, September 22–26, 2001.
References
- Received November 21, 2004.
- Accepted after revision January 26, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Toward a Better Understanding of Dural Arteriovenous Fistula Angioarchitecture: Superselective Transvenous Embolization of a Sigmoid Common Arterial Collector
- Endovascular Treatment of Dural Arteriovenous Fistulas Using Transarterial Liquid Embolization in Combination with Transvenous Balloon-Assisted Protection of the Venous Sinus
- Angioarchitecture of Transverse-Sigmoid Sinus Dural Arteriovenous Fistulas: Evaluation of Shunted Pouches by Multiplanar Reformatted Images of Rotational Angiography
- ONYX versus n-BCA for embolization of cranial dural arteriovenous fistulas
- Onyx 18 embolisation of dural arteriovenous fistula via arterial and venous pathways: preliminary experience and evaluation of the short-term outcomes
- Cranial dural arteriovenous fistula: transarterial Onyx embolization experience and technical nuances
- Spontaneous Angiographic Conversion of Intracranial Dural Arteriovenous Shunt: Long-Term Follow-Up in Nontreated Patients