
Abstract
Summary: The falcine sinus is a normal anatomic structure located in the falx cerebri that closes after birth and is rarely observed in the adult population. We describe a unique case of persistent falcine sinus in an adult who presented with venous sinus obstruction.
Persistent falcine sinus has largely been described in the literature in the pediatric population. In children, Sener (1) found that persistent falcine sinus can be an incidental finding; however, it is more commonly seen with conditions such as malformations of the vein of Galen, arteriovenous malformations, absence of the corpus callosum, osteogenesis imperfecta, acrocephalosyndactyly, and Chiari II malformations. A visible falcine sinus has also been described in a child with dural sinus thrombosis (2). We describe a case of persistent falcine sinus in an adult who presented with sigmoid sinus obstruction. To the best of our knowledge, this entity has not been described before in the adult population.
Case Report
A 52-year-old African American woman with a medical history of sarcoidosis, presented to the emergency department with a 3–5-day history of left-sided neck, shoulder, and arm pain. The patient had a left subclavian venous access port in place that was placed 2 years earlier for medication infusion.
On examination, the patient had 3+ edema of the left side of her upper chest and neck. The soft tissue swelling also extended into her left arm and was tender to palpation. Initial CT of the neck showed thrombus in the left brachiocephalic vein with extension into the left internal jugular vein and into the left sigmoid sinus (not shown).
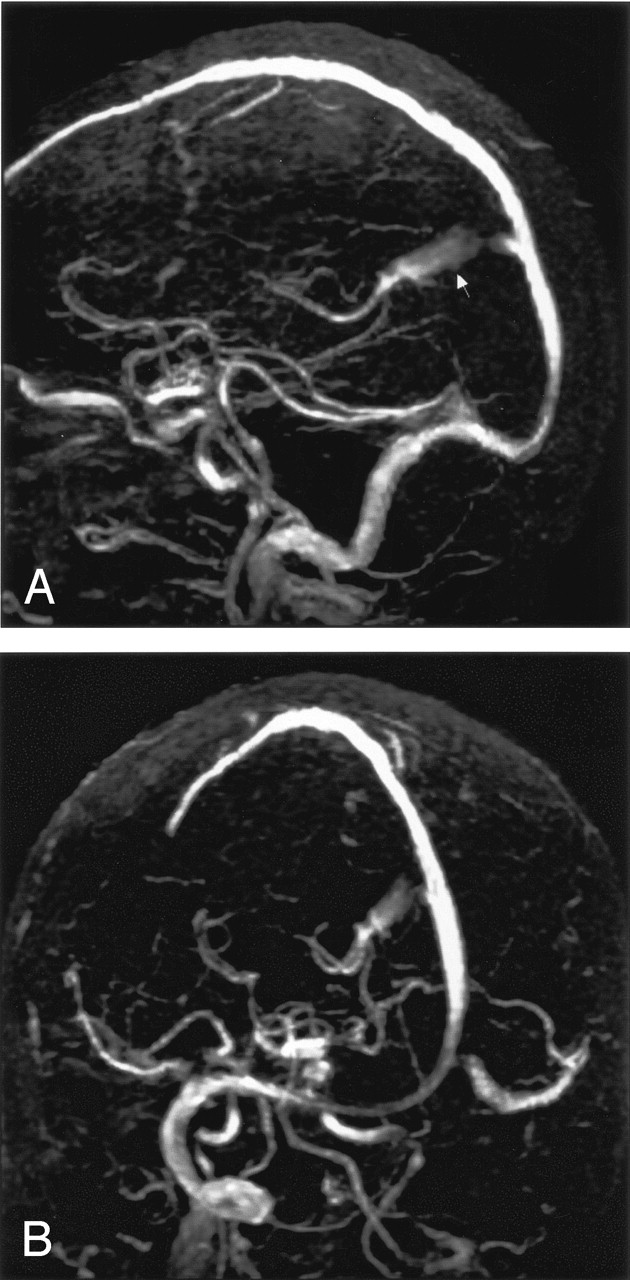
Alternative central venous access was obtained, and the patient was given urokinase therapy. MR imaging without and that with gadolinium and a non-contrast MR venography of the brain were performed. This showed acute thrombosis of the left distal transverse sinus, sigmoid sinus, and left internal jugular vein. A linear vascular structure was noted in the posterior falx extending from the vein of Galen to the superior sagittal sinus. A very small straight sinus was also visible (Fig 1). The patient was continued on anticoagulation therapy, and the remainder of her hospital course was uneventful.

A, Coronal acquisition 2D time-of-flight MR venographic sagittal projected image. B, Coronal acquisition 2D time-of-flight MR venographic oblique projected image. The persistent falcine sinus is visible (arrow), as is the atretic straight sinus. Note the lack of flow within the thrombosed left distal transverse and sigmoid sinus.
Discussion
The falcine sinus is a normal structure located in the falx cerebri, normally involuting after birth (1). The falcine sinus develops from mesenchyme in the mesencephalic flexure, the same area that gives rise to the straight sinus (3). When the straight sinus is absent or rudimentary (1, 4), the falcine sinus can be recanalized to enable venous drainage in response to the atretic straight sinus. Sener (1) suggests that a mesenchyme disorder is the primary cause for the persistent falcine sinus either in isolation or in association with the changes in the straight sinus. This is based on the premise that, if there is a defect that interferes with development of the mesenchyme that gives rise to the tentorium and tentorial plexus, an alternative drainage is found by forming a sinus with the sagittal plexus. Streeter (5) defined the sagittal plexus as a mesh of anastomotic loops from which the superior sagittal sinus and the straight sinus develop. Kesava (2) argues that that the persistent falcine sinus represents persistence of one of the caudal anastomotic loops of the sagittal plexus.
When the falcine sinus is observed in conjunction with vein of Galen malformations, the straight sinus is usually absent or thrombosed (6, 7). Drainage typically occurs into the falcine sinus that empties into the superior sagittal sinus rather than into the confluence of sinuses (8, 9). The findings of falcine sinus occurring with the vein of Galen malformation have been described on the basis of 3D color power angiographic findings obtained in utero (8). We did not observe findings suggestive of vascular malformation in our patient. There were no visible enlarged arterial structures and the vein of Galen was of normal size.
Reddy et al (10) described a small group of children with persistent falcine sinus that occurred with enlarged parietal foramina. They found an association between the enlarged parietal foramina and anomalies of cerebral venous development. They also noted an association between variations of cortical infolding, enlarged parietal foramina, and falcine sinus. Our patient did not demonstrate any of the associated findings that Reddy et al observed. Sener describes two cases of falcine sinus as an incidental finding in the pediatric population (1). In our patient, it is not clear whether the falcine sinus became recanalized due to the obstruction of the sigmoid sinus and potential increased venous pressure or had always been present as a congenital variation. The latter may seem more plausible in our patient, in light of the diminutive size of the straight sinus.
References
- Received June 10, 2004.
- Accepted after revision July 11, 2004.
- American Society of Neuroradiology





{kind=link}