
Abstract
Summary: MR imaging in a 73-year-old man presenting with hemispheric stroke revealed a subcortical diffusion-weighted imaging lesion associated with a high-grade stenosis of the proximal internal carotid artery, which suggested hemodynamic infarction. Collateral supply was absent. After failure of conservative therapy, successful unprotected carotid artery stent placement (CAS) was performed followed by a complete neurologic recovery. Emergency CAS should be considered in acute stroke patients with severe hemodynamic impairment if conservative treatment options are not successful.
Elective carotid artery stent placement (CAS) may be an alternative to surgery in secondary stroke prevention. Ongoing trials (1) such as SPACE (stent-protected angioplasty of carotid artery versus endarterectomy) are evaluating the clinical benefit of CAS in comparison with carotid endarterectomy (CEA). Emergency CAS in acute stroke entails increased risks due to hyperperfusion injury, bleeding into infarcted areas, and secondary embolism.
In the rare case of severe carotid artery stenosis in combination with poor collateral supply, ischemic symptoms may be caused by persistent hemodynamic impairment rather than by thromboembolism. Acute MR imaging including diffusion-weighted (DW) imaging and perfusion-weighted imaging (PWI) sequences, as well as time-of-flight (TOF) and contrast-enhanced MR angiography (CE-MRA), delivers information about stroke pathogenesis and helps detect these patients. We present a case of acute hemodynamic stroke where emergency CAS was the appropriate treatment option.
Case Description
A 73-year-old man presented with acute left hemiplegia, dysarthria, gaze palsy to the right, and anosognosia. The National Institutes of Health Stroke Scale (NIHSS) on admission was 15.
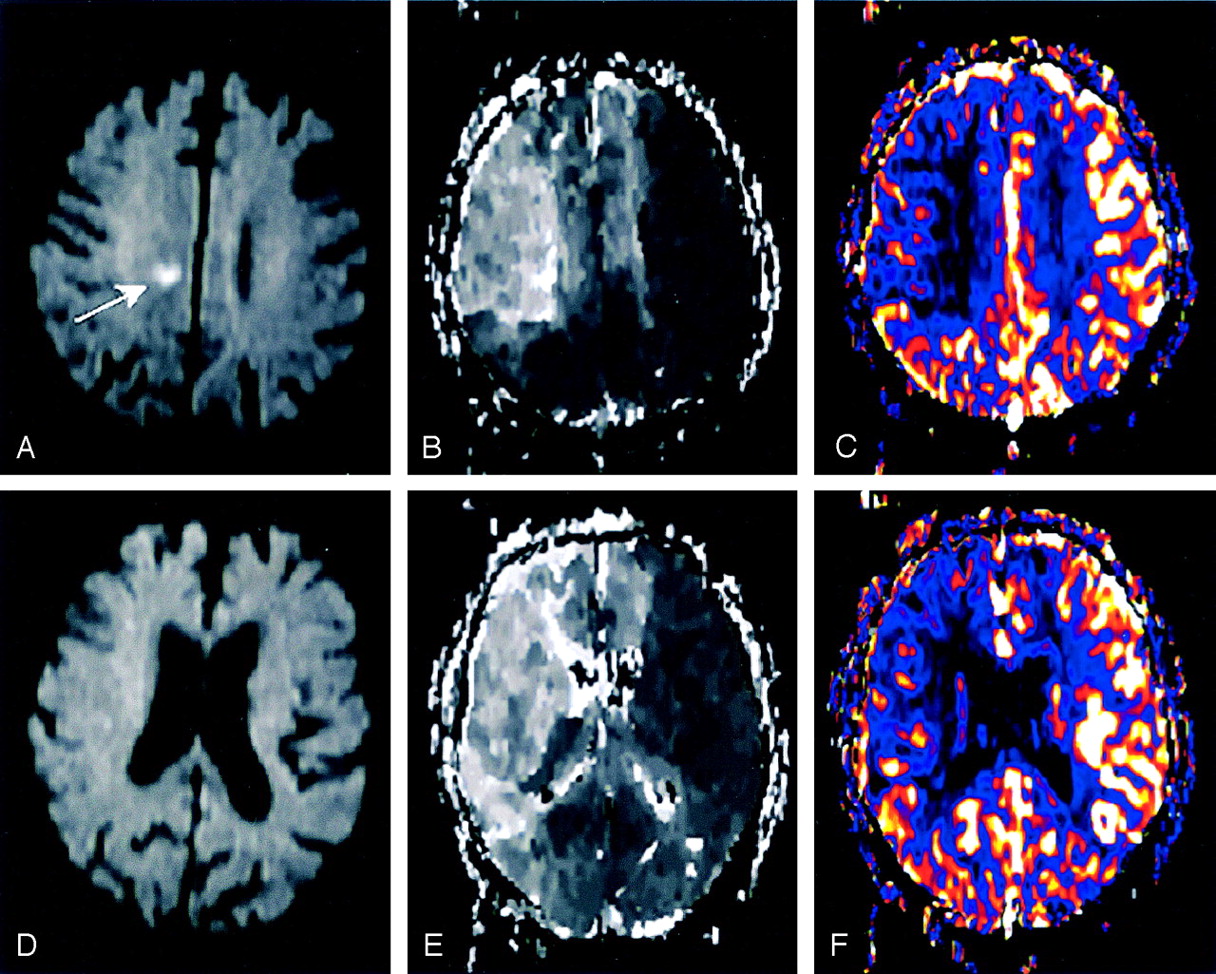
MR diagnostics 2 hours after the onset of stroke were performed on a 1.5-T system (Siemens Magnetom Sonata, Erlangen, Germany) including fluid-attenuated inversion recovery (FLAIR), T2*-weighted imaging, DW imaging, PWI (time-to-peak [TTP] and cerebral blood flow [CBF]), TOF, and CE-MRA. Total acquisition time for MR imaging was 25 minutes. The DW imaging revealed a small lesion in the subcortical white matter of the right hemisphere without any cortical lesions (Fig 1A). Intracranial TOF only faintly visualized the right distal internal carotid artery (ICA) and the right middle cerebral artery (MCA), which suggested a proximal ICA occlusion. Supplementary CE-MRA confirmed a high-grade stenosis (>90%) of the proximal right ICA (Fig 2A) and a moderate stenosis (50%) of the left ICA. Intracranially, the A1 segment of the left anterior cerebral artery (ACA) and the right posterior communicating artery were absent. These findings suggested a dominant perfusion of both ACA territories by the stenotic right ICA. A subsequent PWI (TTP and CBF) demonstrated a substantial delay and decrease of perfusion in almost the entire right MCA territory, as well as in both ACA territories (Fig 1B, -C, -E, -F). In summary, MR imaging findings revealed hemodynamic stroke origin without peripheral embolic occlusions. Therefore, intravenous thrombolysis was not performed.

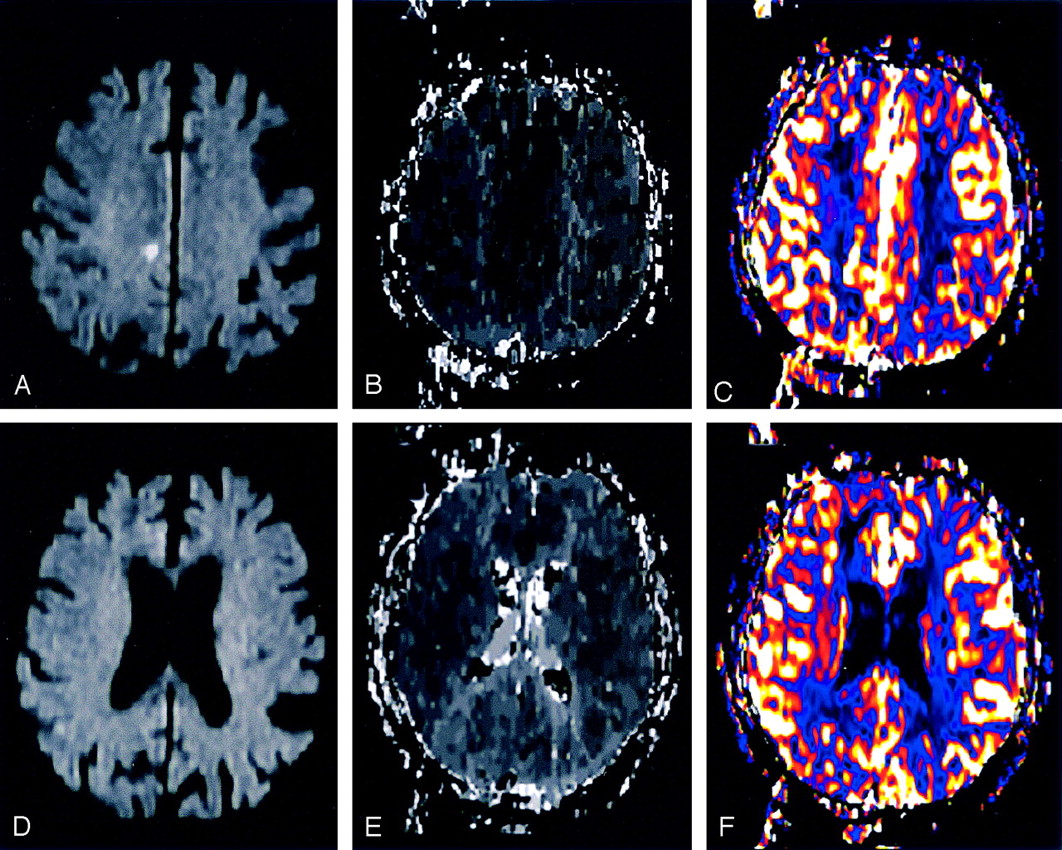
MR imaging 2 hours after the onset of stroke.
A and D, Acute MR imaging with two representative sections of DW imaging revealing a small lesion in the subcortical white matter (A, arrow), suggesting hemodynamic infarction.
B and E, Acute MR imaging with the same sections of TTP, demonstrating a perfusion delay in almost the entire right MCA territory and in both ACA territories.
C and F, Acute MR imaging with the same sections of CBF showing a decrease of cerebral blood flow in almost the entire right MCA territory and in both ACA territories, matching the TTP results.

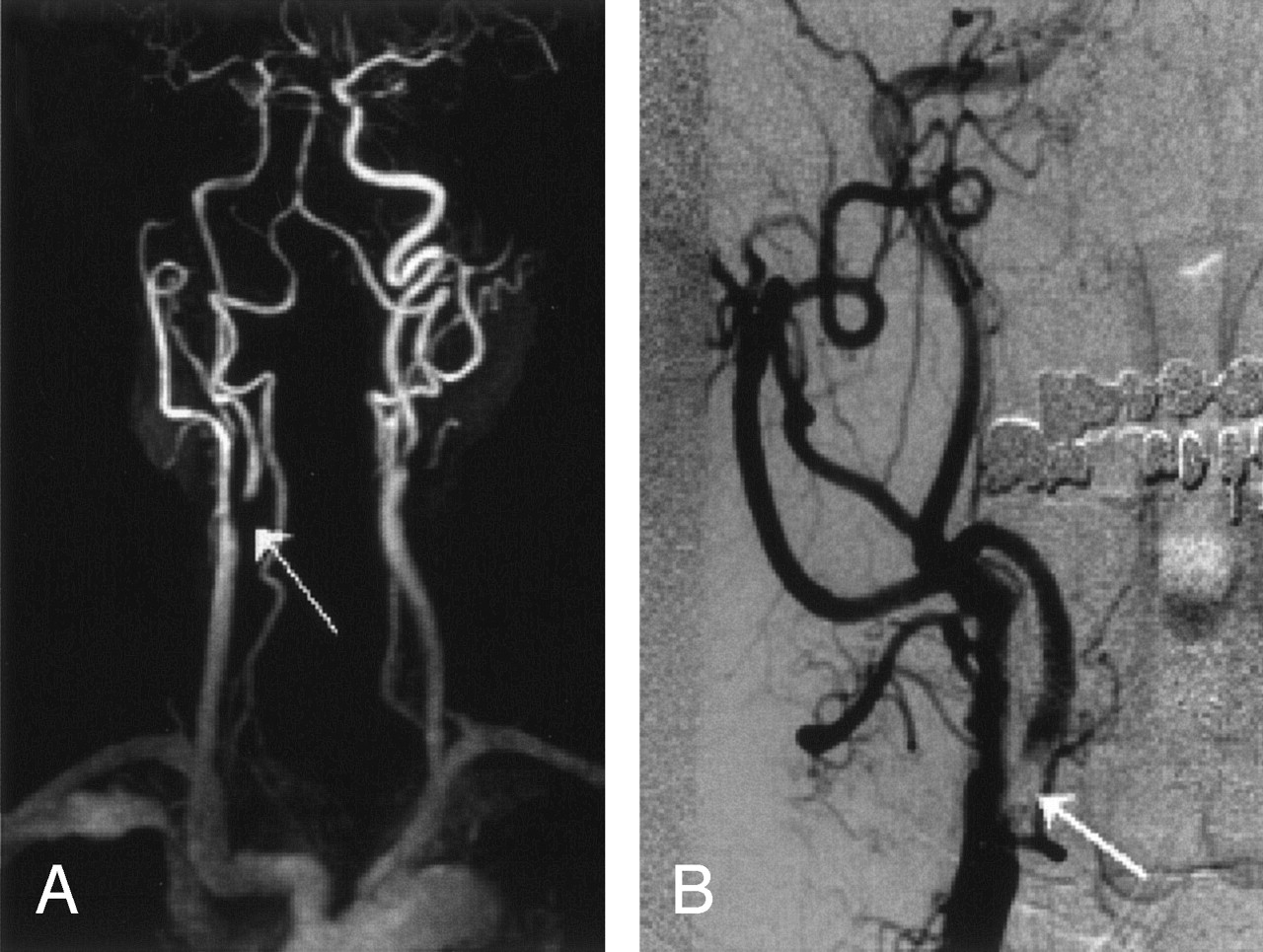
Before CAS placement.
A, Initial CE-MRA displaying a high-grade stenosis of the proximal right ICA (arrow), a moderate stenosis of the left ICA, and lack of an A1-segment of the left ACA.
B, Diagnostic angiography of the right ICA (anteroposterior) after selective injection in the right CCA, revealing the >95% stenosis of the proximal right ICA (arrow).
In a 1-hour attempt to increase systemic blood pressure by hypervolemic and hypertensive therapy, clinical symptoms did not improve. The persistent neurologic deficit and risk of ICA occlusion with a severe infarction of the right hemisphere and potentially even the left ACA territory led to the decision for CAS. Informed consent was obtained from the patient.
Diagnostic angiography revealed a >95% stenosis of the proximal right ICA (Fig 2B). The A1 segment of the left ACA and right posterior communicating artery were lacking. Because of progressing neurologic symptoms, endotracheal intubation was required in the course of the diagnostic angiography. To prevent thromboembolism, intravenous Abciximab was administered (bolus of 0.25 mg/kg, followed by 0.125 μg/kg/min continuously over a period of 12 hours). Neither acetyl salicylic acid (ASA) nor Clopidogrel was given before CAS.
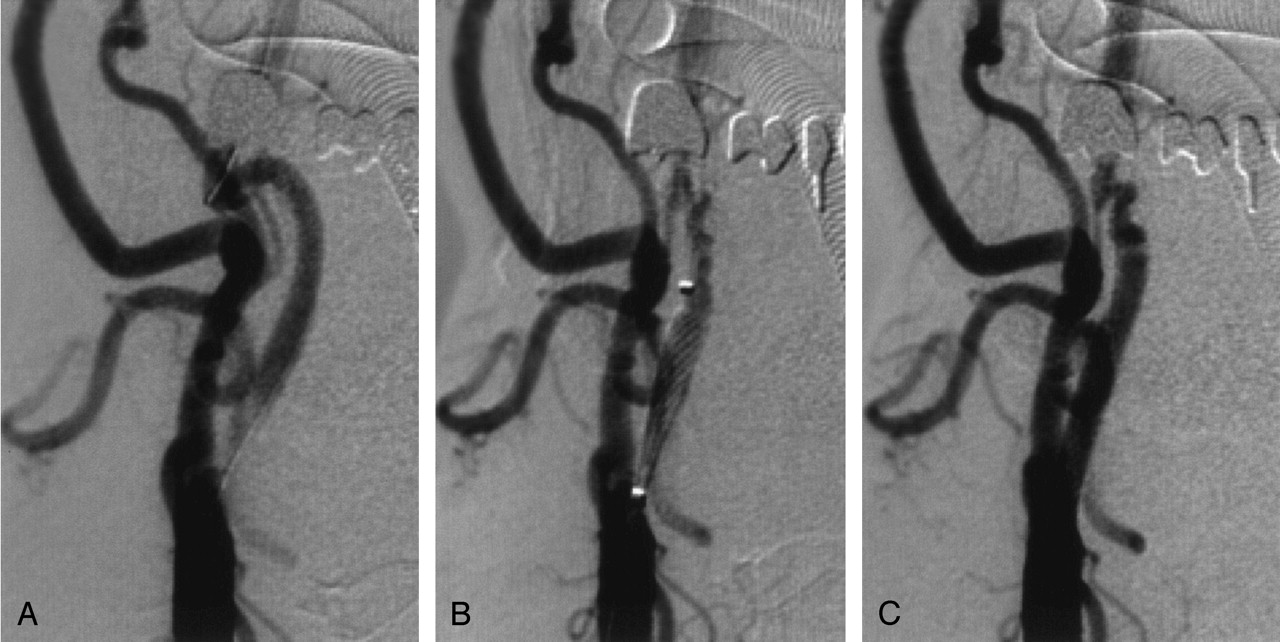
CAS was performed according to the protocol used in our neuroradiology department ( 2). Protection devices were not used. After placing a guidewire (Balance Heavyweight, Guidant, Santa Clara) through the stenosis (Fig 3A), a primary stent placement without predilatation was performed (Fig 3B) by using a 7 × 21 mm stent (Carotid Wallstent Monorail, Boston Scientific, Galway, Ireland). Postdilatation was carried out with a 5.5 × 20 mm balloon catheter (Maverick XL, Boston Scientific, Maple Grove, MN) inflated to a pressure of 12 bar. CAS was completed 5 hours after the onset of stroke. The control angiogram demonstrated a complete recanalization of the proximal right ICA (Fig 3C) with normalized filling of the right MCA and both ACA territories.

Three angiographic depictions during CAS (after selective CCA injection; anteroposterior views).
A, Guidewire placed through the stenosis.
B, Stent deployment along the stenosis.
C, Complete recanalization of the proximal right ICA after treatment.
The patient was transferred to the neurologic intensive care unit for extubation and further treatment. The following day (18 hours after extubation) a complete clinical neurologic recovery was observed. Follow-up MR imaging 24 hours after CAS revealed no new ischemic lesions (Fig 4A–D) or intracranial bleeding. The TOF angiography showed a restored flow void of the right ICA, the right MCA, and both ACAs. Correspondingly, the PWI (TTP and CBF) showed a timely reperfusion of the right MCA and both ACA territories (Fig 4B, -C, -E, -F). The NIHSS at discharge (12 days after admission) was 0.

MR imaging at follow-up.
A and D, MR imaging 24 hours after treatment with corresponding sections of DW imaging without any new cortical or subcortical ischemic lesions.
B and E, MR imaging 24 hours after treatment with the same sections of TTP demonstrating a timely reperfusion of the right MCA and both ACA territories.
C and F, MR imaging 24 hours after treatment with the same sections of CBF showing a normalized cerebral blood flow, matching the TTP results.
Discussion
Persistent hemodynamic deficit is a rare cause of acute hemispheric stroke (3,,4). Acute stroke MR imaging—including DW imaging, PWI, TOF, and CE-MRA—may differentiate rare cases of pure hemodynamic stroke from embolic stroke. A typical constellation regarding the hemodynamic stroke subtype is a severe proximal stenosis associated with abnormalities in the circle of Willis (5). With a patient selection based on CT data according to the National Institute of Neurological Disorders and Stroke protocol (6) the presented patient (stable deficit, exclusion of hemorrhage) would have been a candidate for intravenous thrombolysis. Although we cannot prove our hypothesis, it seems very unlikely that this patient might have had a benefit from intravenous thrombolysis. On the basis of the MR imaging diagnosis of pure hemodynamic stroke was confirmed and because of the persistent neurologic deficit despite of aggressive attempts to increase the blood pressure, we decided to perform emergency CAS.
In this acute phase, fresh thrombotic material may cover the surface of the stenosis, increasing the risk of CAS induced embolic complication. Therefore, a complete and immediate blockade of platelet aggregation is required. This can be achieved with an intravenous administered glycoprotein IIb/IIIa-receptor antagonist, such as Abciximab (7,8) in the presented case.
The use of protection devices in CAS is another matter of debate (9,10). We preferred primary unprotected stent placement with periprocedural application of Abciximab to a protection system requiring a predilatation in this tight stenosis. Emergency CEA may be an alternative treatment (11,12), but it implies a considerable time delay. The endovascular approach, in contrast to CEA, ensures the visualization of the intracranial vessels during the procedure.
Conclusion
Modern MR imaging acute stroke diagnostics may select rare cases of pure hemodynamic stroke in differentiation from embolic stroke. In case of hemodynamic stroke, after failure of conservative treatment, CAS in the acute phase may be the treatment of choice.
References
- Received May 18, 2004.
- Accepted after revision June 26, 2004.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}