
Abstract
BACKGROUND AND PURPOSE: Pediatric head and neck lesions can be difficult to characterize on clinical grounds alone. We investigated the use of dynamic MR digital subtraction angiography as a noninvasive adjunct for the assessment of the vascularity of these abnormalities.
METHODS: Twelve patients (age range, 2 days to 16 years) with known or suspected vascular abnormalities were studied. Routine MR imaging, time-of-flight MR angiography, and MR digital subtraction angiography were performed in all patients. The dynamic sequence was acquired in two planes at one frame per second by using a thick section (6–10 cm) selective radio-frequency spoiled fast gradient-echo sequence and an IV administered bolus of contrast material. The images were subtracted from a preliminary mask sequence and viewed as a video-inverted cine loop.
RESULTS: In all cases, MR digital subtraction angiography was successfully performed. The technique showed the following: 1) slow flow lesions (two choroidal angiomas, eyelid hemangioma, and scalp venous malformation); 2) high flow lesions that were not always suspected by clinical examination alone (parotid hemangioma, scalp, occipital, and eyelid arteriovenous malformations plus a palatal teratoma); 3) a hypovascular tumor for which a biopsy could be safely performed (Burkitt lymphoma); and 4) a hypervascular tumor of the palate (cystic teratoma).
CONCLUSION: Our early experience suggests that MR digital subtraction angiography can be reliably performed in children of all ages without complication. The technique provided a noninvasive assessment of the vascularity of each lesion that could not always have been predicted on the basis of clinical examination or routine MR imaging alone.
Pediatric head and neck abnormalities are relatively common and frequently are brought to medical attention because of their conspicuity and associated disfigurement. The nature of many of these lesions can be adequately assessed by clinical examination alone, but the vascularity of certain abnormalities is more difficult to evaluate and requires further investigation. MR imaging often is performed as the first imaging method to characterize the lesion and document the extent of the abnormality, sometimes as a prelude to treatment. One of the most important features that must be established is the vascularity of the lesion.
Vascular imaging can help to differentiate between high and low flow lesions in terms of structural changes, such as enlarged vessels and capillary staining, and can help to delineate hemodynamic parameters that are most simply assessed by the speed of arteriovenous shunting. Traditionally, this has been performed by transfemoral angiography, a technique that has a small but finite complication rate and can be difficult to perform in small children.
Recent advances in MR imaging have enabled the acquisition of dynamic (or time-resolved) angiographic data sets with high spatial and temporal resolution (1–3). These techniques have already been described for the assessment of brain arteriovenous malformations (4–9), dural fistulae (8–11), and cerebrovascular disease (12, 13). We herein present our preliminary work with MR digital subtraction angiography in the assessment of the vascularity of pediatric head and neck lesions.
Methods
Twelve patients were studied (five male, seven female) with an age range of 2 days to 16 years. All examinations were performed on a 1.5-T system (Infinon; Philips Medical Systems, Cleveland, OH). Routine multiplanar imaging and time-of-flight MR angiography were performed before the dynamic acquisitions were obtained. MR digital subtraction angiography was performed in the frontal and lateral projections by using half of the total allowable dose of 1.0 mol/L gadolinium chelate (Gadovist; Schering AG, Berlin) for each projection. Contrast-enhanced T1-weighted spin-echo images were obtained after dynamic angiography was performed.
Our MR digital subtraction angiography protocol has previously been described in detail (4) and is summarized herein. The sequence uses a section-selective radio-frequency spoiled fast gradient-echo sequence (7/2 [TR/TE]; flip angle, 40°; matrix, 150 × 256; field of view, 230 mm; section thickness, 6–10 cm). Images were acquired as thick 2D sections every second for a total of 1 minute. After a preliminary unenhanced acquisition, a second run was performed during the IV administration of a bolus of contrast material (at 3 mL/s) and then a 10-mL saline flush at the same rate. The dataset was rapidly processed and viewed as a subtracted video-inverted cine loop with a temporal resolution of one frame per second.
Lesions were classified as high flow lesions if any of the following was shown: 1) rapid enhancement during the arterial phase of angiography, 2) arteriovenous shunting, or 3) enlarged vessels. Lesions that became conspicuous during the venous phase or did not show increased contrast enhancement were defined as low flow lesions.
Results
MR digital subtraction angiography was performed without clinical complication in all 12 patients. In each case, the images were considered to be of high quality, equal or better to the results we routinely achieve in the adult population. The salient clinical details and radiologic findings are summarized in the Table.
Clinical details and MR imaging findings
In some instances, the initial clinical diagnosis was revised on the basis of MR imaging results. Figure 1 shows images obtained in a child with a suspected low flow vascular lesion of the scalp. Standard MR imaging showed an extra-calvarial mass with serpiginous flow voids indicative of enlarged vessels. MR digital subtraction angiography confirmed the high flow nature of this lesion. A 14-month-old child (Fig 2) presented with a large neck mass that could not be characterized by clinical examination. Conventional MR imaging showed appearances consistent with a large parotid hemangioma. MR digital subtraction angiography revealed high flow within this lesion by virtue of early arterial phase enhancement and also arteriovenous shunting. This was thought to be consistent with a hemangioma in the highly vascular (proliferative) phase. A 1-week-old neonate (Fig 3) presented with a huge occipital mass that was initially thought to be an encephalocele. MR digital subtraction angiography revealed a highly vascular amorphous mass, the vascularity of which was confirmed by histologic analysis. MR digital subtraction angiography was also able to show the absence of significant blood flow within a suspected tumor. Figure 4 shows images obtained in a 5-year-old male patient with a nasopharyngeal mass that was initially thought to be a juvenile angiofibroma on the basis of clinical findings. MR imaging and MR digital subtraction angiography revealed a large but relatively avascular mass. Biopsy was safely performed, and the lesion was shown to be a Burkitt lymphoma.

Images from the case of a 3-year-old female patient with a suspected vascular abnormality of the scalp.
A, Unenhanced sagittal T1-weighted MR image shows an extra-calvarial soft tissue mass.
B, Marked uniform enhancement can be seen after the administration of contrast material. Serpiginous flow void represents an enlarged feeding vessel.
C, Selected MR digital subtraction angiograms show prominent filling of contrast material in the arterial phase and prominent enhancement of the lesion. This was considered to represent a high-flow lesion.

Images from the case of a 14-month-old female patient with left-sided neck swelling.
A, Unenhanced axial T1-weighted MR image shows an encapsulated mass in the left parotid gland.
B, After the administration of contrast material, marked contrast enhancement is seen. Note the vascular flow voids within the lesion.
C, Selected MR digital subtraction angiograms show early arterial filling of the hypervascular lesion and arteriovenous shunting into an early draining vein. This is consistent with a parotid hemangioma in the proliferative phase.

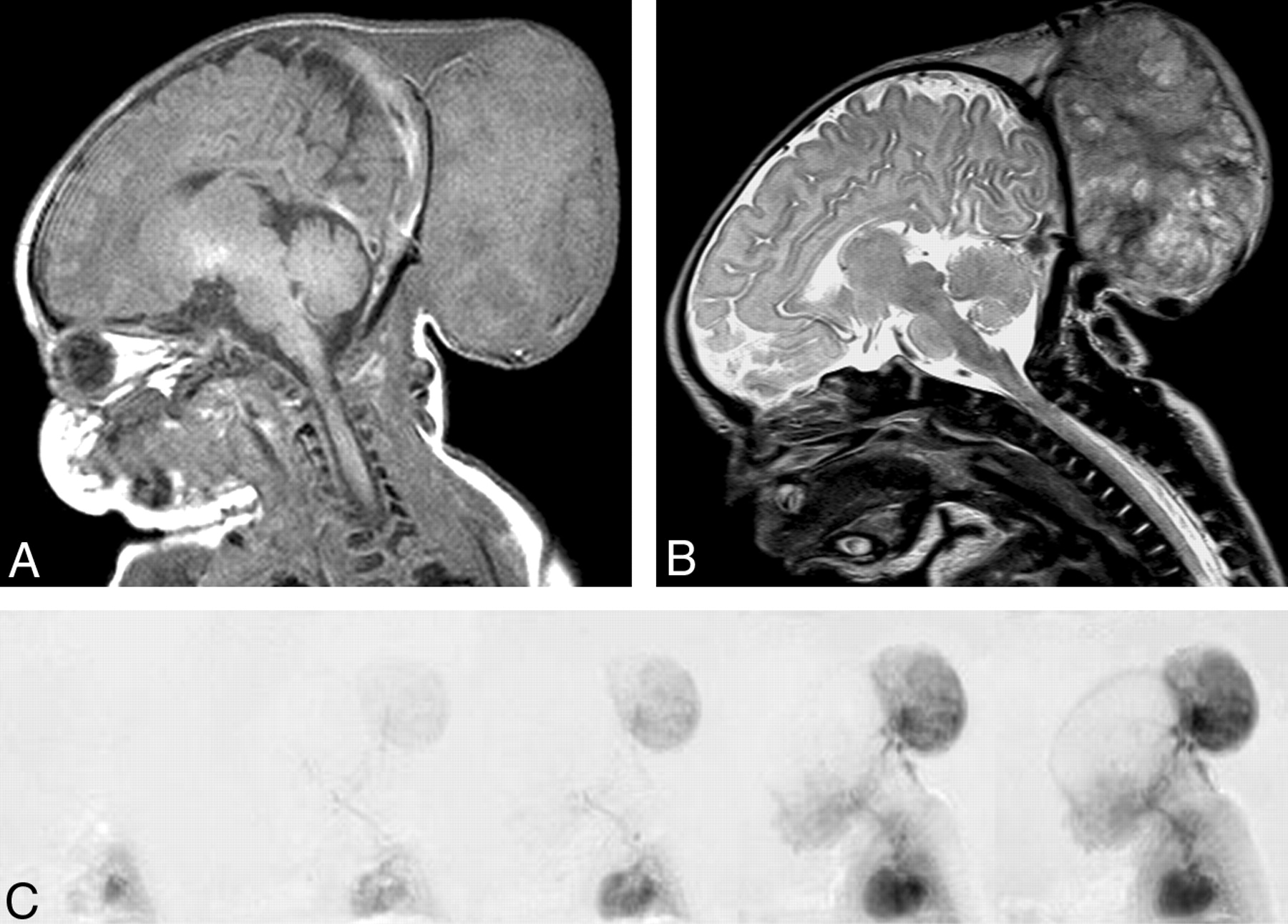
Images from the case of a 5-day-old female patient with a large occipital mass thought to be an encephalocele.
A, Sagittal T1-weighted MR image shows a large occipital mass with intermediate signal intensity.
B, More heterogeneous appearance can be seen on the T2-weighted image. No intracranial communication is shown.
C, Selected MR digital subtraction angiograms show rapid opacification of the lesion during the early arterial phase. Flow in this lesion was so high that the intracranial vessels are poorly shown. Pathologic examination revealed an undifferentiated highly vascular tumor.

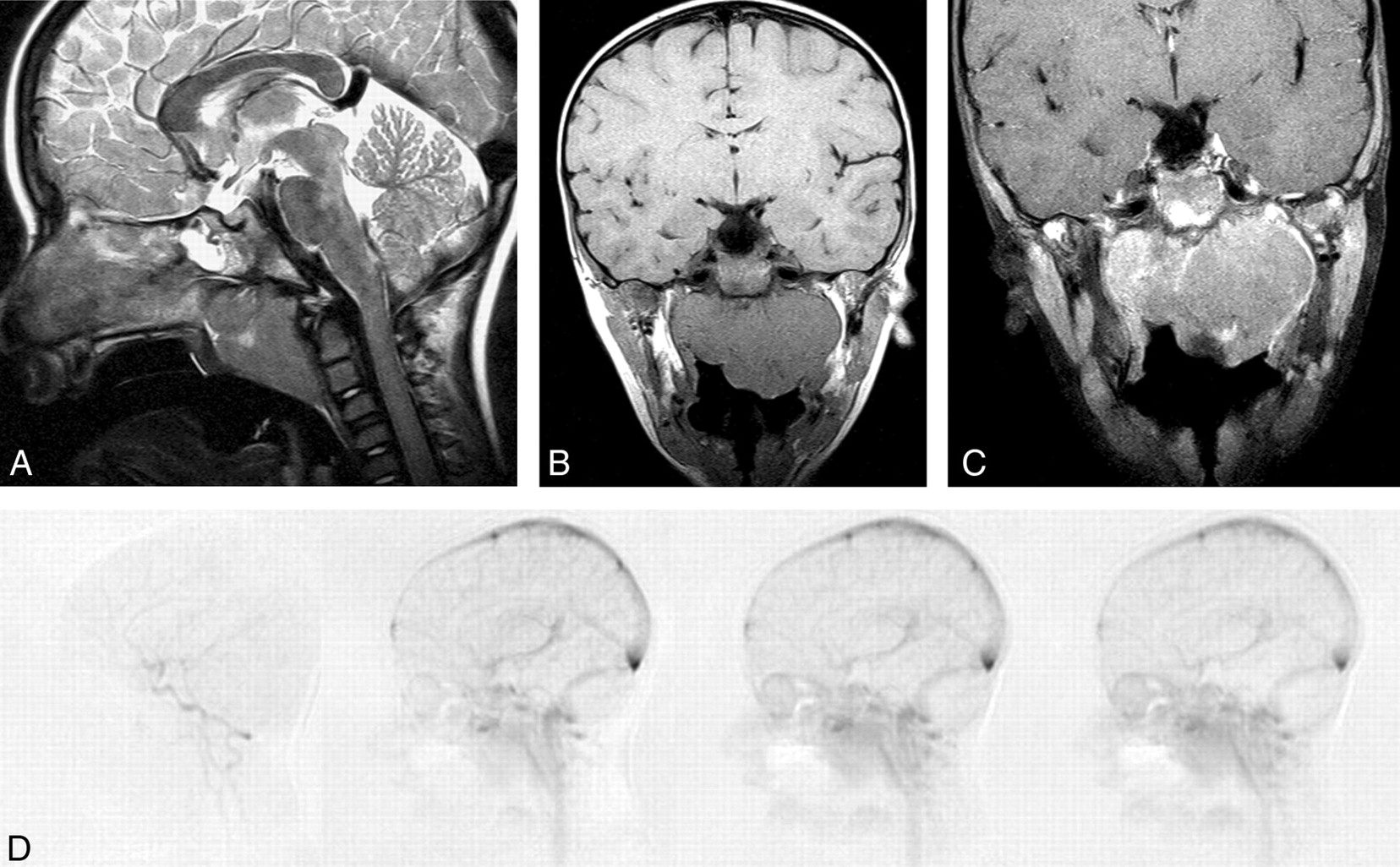
Images from the case of a 5-year-old male patient with a nasopharyngeal mass.
A, Lobulated nasopharyngeal mass is seen on the sagittal T2-weighted MR image.
B, T1-weighted coronal MR image also shows the lobulated nasopharyngeal mass.
C, Coronal contrast-enhanced fat-saturated T1-weighted MR image shows minor eccentric contrast enhancement.
D, No significant contrast material flow was seen within the lesion on MR digital subtraction angiograms. This lesion was diagnosed as Burkitt lymphoma on the basis of biopsy findings.
In other cases, MR digital subtraction angiography provided complementary evidence of a low flow lesion. These included a suspected scalp venous malformation, a lid hemangioma, and choroidal angiomas in two patients with Sturge-Weber syndrome. One example of a shunting arteriovenous malformation did not show enlarged flow voids on the spin-echo sequences.
Discussion
Characterizing the vascularity of certain pediatric head and neck lesions may be difficult on the basis of clinical examination alone. It is, however, important to differentiate such abnormalities, because the differentiation will often influence the further management of these lesions (14, 15). High flow arteriovenous malformations are often treated by a combination of intra-arterial embolization and surgery (16). Percutaneous sclerotherapy is the preferred method of treatment for venous malformations (17). Hemangiomas usually do not warrant intervention, because many will spontaneously involute.
Most head and neck tumors and vascular malformations show increased enhancement on standard MR images after administration of contrast material. Although certain appearances of high and low flow lesions, such as visible flow voids (18), have been depicted on standard MR images, these are static images that do not allow assessment of the hemodynamics of the lesion. Furthermore, flow voids may be absent or inconspicuous in certain lesions (19). The unique value of MR digital subtraction angiography is its ability to show the passage of a bolus of contrast material through the abnormality in a manner identical to that of conventional angiography.
High flow lesions show rapid contrast enhancement during the early arterial phase and may show enlarged vessels and pathologic arteriovenous shunting with early venous filling. Low flow lesions, such as venous malformations and certain hemangiomas, may show less dramatic contrast enhancement on routine MR images; however, most importantly, the lesion does not show early opacification on MR digital subtraction angiograms. Such lesions show either no vascularity on MR digital subtraction angiograms or appear during the venous phase (20).
Ziyeh et al (20) recently reported their experience with time-resolved MR projection angiography in the assessment of head and neck vascular malformations. Using view-sharing and temporal interpolation, the authors were able to achieve a temporal resolution approaching four frames per second. Five patients with venous malformations showed no pathologic vasculature on dynamic images, whereas contrast enhancement was observed on T1-weighted spin-echo MR images. Two high flow arteriovenous malformations were readily identified and were classified as such by determining the time delay between the arrival of the contrast material bolus in the extracranial carotid circulation and the vascular malformation. Rapid arrival of contrast material was associated with intense enhancement on the dynamic sequences. Furthermore, our own early experience suggests that MR digital subtraction angiography may also allow assessment of the vascularity of neoplastic lesions without the risks and expense associated with conventional angiography.
At present, MR digital subtraction angiography is inferior to conventional angiography in terms of spatial and temporal resolution and therefore has some limitation in the assessment of those arteriovenous malformations associated with rapid arteriovenous shunting. Although rapid sub-second MR imaging can be performed with frame rates similar to those of conventional angiography (21), such techniques remain experimental at this time and require further work to produce satisfactory spatial resolution. Furthermore, by using an IV injection of contrast material, there is simultaneous opacification of the internal carotid, external carotid, and vertebral circulations. This feature can create diagnostic difficulties with vessel superimposition and dural shunts. Current MR digital subtraction angiography techniques for use in the head and neck region also are limited to a small number of 2D projections that cannot be manipulated in the third plane and therefore cannot generate 3D models or be shown in an infinite number of oblique projections. A specific limitation of this study is lack of correlation with conventional angiography. Because the high flow arteriovenous malformations and parotid hemangioma were not considered for surgical intervention at this time, we could not justify subjecting these patients to further investigation.
Conclusion
Despite the limitations of this study and the technique it used, we think MR digital subtraction angiography has a potentially important role in the assessment of both neoplastic and non-neoplastic pediatric head and neck lesions.
Footnotes
Presented at the 41st Annual Meeting of the American Society of Neuroradiology, April 26–May 2, 2003; Washington, DC.
References
- Received July 16, 2003.
- Accepted after revision December 22, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.