
Abstract
Summary: CT angiography (CTA) of the cervical and intracranial vessels is a rapid, noninvasive, and relatively inexpensive technique for the evaluation of vascular abnormalities. Contraindications to the use of contrast media, however, can preclude use of iodinated agents for CTA. We report the use of gadolinium as contrast agent for CTA of the head and neck in three patients with contraindications to iodinated contrast agents.
CT angiography (CTA) allows reliable pretreatment planning and diminishes evaluation time for most cases of aneurysmal subarachnoid hemorrhage (1). Indeed, the accuracy of CTA for aneurysm detection has been shown to exceed that of conventional digital subtraction arteriography and, by extension, MR angiography (MRA; 2). CTA is also highly accurate for evaluation of large-vessel intracranial occlusions and is a valuable tool in the rapid triage of stroke patients to intra-arterial thrombolytic treatment (3). Furthermore, CTA of cervical vessels is useful in the evaluation of cervical arterial stenosis (4). Thus, the availability of an alternative to standard CT contrast agents would be of significant value in patients with contraindications to administration of iodinated contrast media.
Description of Technique and Report of Cases
CTA was performed on a 16-detector multisection helical scanner (LightSpeed, General Electric, Milwaukee, WI) in the head-first, supine orientation. The standard technique for iodinated CTA was employed. For detection of an aneurysm in patient 1, the study was performed by using a 25-second delay after contrast medium administration, 140 kVp, 170 mA, 0.8-second rotation time, 1.25-mm section thickness reconstructed at 0.6-mm intervals, 3.75 mm/rotation table speed, pitch 0.75:1, and soft-tissue algorithm reconstruction. Images were obtained from the C2 vertebral body through the vertex. For CTA of the cervical and intracranial vessels in patients 2 and 3, images were obtained by using a 25-second delay after contrast medium administration, 140 kVp, 250 mA, 1.0-second rotation time, 2.5-mm section thickness reconstructed at 1.25-mm intervals, 3.75 mm/rotation table speed, and pitch 0.75:1. A set of images was obtained from the C6 vertebral body level through the circle of Willis followed immediately by a second set of images from the aortic arch through the C6 level. Instead of iodinated contrast material, a power infusion of 60 mL of gadopentetate dimeglumine (Magnevist, Berlex, Wayne, NJ) was followed by a 20-mL normal saline chase, both injected at 4 mL/s through an 18-gauge cannula placed into an antecubital vein. Sixty milliliters of gadolinium (≈0.4 mmol/kg) are used at our institution for venous-enhanced peripheral MR angiography and, thus, were not considered to be investigational.
Case 1
A 63-year-old man on warfarin therapy for atrial fibrillation entered the emergency department after 30 minutes of severe right retro-orbital headache, blurred vision, and dizziness. An unenhanced CT scan of the head showed no evidence of intracranial or orbital hemorrhage. The emergency department physician requested an angiographic study of the circle of Willis to exclude an unruptured aneurysm. Because the patient had a permanent cardiac pacemaker and a history of anaphylaxis following the administration of iodinated CT contrast medium, gadolinium-enhanced CTA was performed. The patient had no adverse symptoms. Later that day, lumbar puncture showed one red blood cell per cubic millimeter of CSF, and no evidence of xanthochromia. Axial and 3D reconstructed images demonstrated no evidence of an intracranial aneurysm (Fig 1). Average attenuation within the gadolinium-enhanced intracranial internal carotid arteries was 94 H.

Gadolinium-enhanced CTA images obtained in a 63-year-old man with sudden-onset, severe headache.
A, Axial 1.25-mm gadolinium-enhanced CTA image shows the right posterior communicating artery (arrow).
B-F, Reconstructed images show the middle and anterior cerebral arteries (B), anterior communicating artery region (C), left posterior communicating artery (D), vertebrobasilar junction and basilar artery (E), and right posterior inferior cerebellar artery origin (F).
Case 2
MRA performed in a 52-year-old woman with severe complications from diabetes, including renal failure treated with renal transplant, suggested severe stenosis of both cervical internal carotid arteries, in a pattern typical of arterial dissections. Fat-saturated images through the neck were inconclusive. Iodinated contrast material was contraindicated because of moderate chronic renal insufficiency in the setting a renal transplant. A gadolinium-enhanced CTA image of the cervical vessels and circle of Willis was obtained (Fig 2). The study suggested complete occlusion of the left internal carotid artery and severe stenosis of the right internal carotid artery with tapered narrowing, which indicated the presence of carotid dissections. Average attenuation within the supraclinoid internal carotid artery was 124 H and 150 H at the carotid bifurcation.

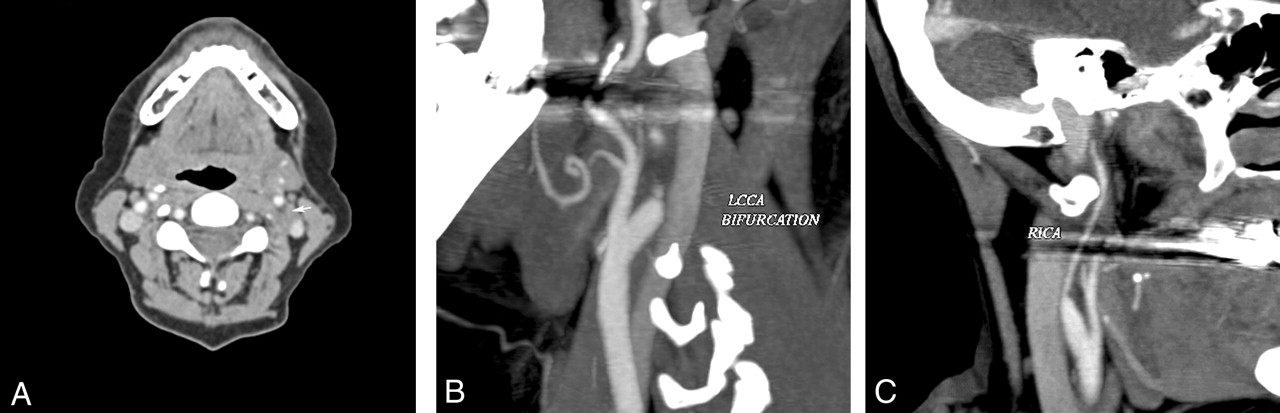
Gadolinium-enhanced CTA images of the cervical vessels obtained in a 52-year-old woman with severe carotid stenosis disclosed by MRA.
A, Axial image shows absence of contrast material in the left internal carotid artery (arrow) and stenosis of the right internal carotid artery.
B, Reconstructed image shows absence of contrast in the left internal carotid artery and smooth tapered narrowing of the proximal vessel.
C, Smooth tapered narrowing of the right internal carotid artery.
Case 3
A 71-year-old man with history of automatic implantable cardiac defibrillator placement, diabetes, and chronic renal insufficiency developed acute onset of expressive aphasia without other symptoms (NIH Stroke Scale, 1). Thrombolytic therapy was not deemed appropriate. The patient did, however, reported a history of a carotid plaque and concerns were raised about the possible need for urgent carotid endarterectomy. Iodinated contrast medium was contraindicated because of chronic renal insufficiency with prior exacerbation after use of iodinated contrast material. Gadolinium-enhanced CTA of the cervical vessels was performed and revealed only mild stenosis of the left carotid bifurcation with scattered atherosclerotic calcification and a hypoattenuated plaque (Fig 3). Immediately following the study, the patient developed mild nausea and flushing and was treated with ranitidine and diphenhydramine without further complications. His creatinine remained stable. Average attenuation within the origin of the common carotid arteries was 150 H and 130 H at the carotid bifurcation.

Gadolinium-enhanced CTA images obtained in a 71-year-old man with acute-onset, expressive aphasia and history of “carotid plaque.”
A, Reconstructed gadolinium-enhanced CTA image shows mild stenosis of the left carotid bifurcation with scattered atherosclerotic calcification and hypoattenuated plaque.
B, Reconstructed image of the left common carotid artery origin shows mild atherosclerotic calcification without any significant stenosis.
Discussion
Gadolinium-enhanced CTA has been used to image major vessels in the chest and abdomen (5), and gadolinium has an established role in conventional angiography in patients with contraindications to iodine (6). Quinn et al (7) reported visualization of gadolinium enhancement on a routine head CT scan, but to our knowledge the use of gadolinium-enhanced CTA of the intracranial and cervical vessels has not been reported.
Subjective image quality, although inferior to that of conventional CTA, was considered diagnostically adequate in each case. Contrast attenuation within the cervical and intracranial arteries was between 94 and 150 H. The K-edge of gadolinium (50 keV) is better matched to the energy profile of a filtered 140-kVp CT beam compared with that of iodine (33 keV), but the lower number of gadolinium atoms per milliliter of contrast agent produces a maximum attenuation that was one-third to one-half the typical values for iodinated contrast–enhanced CTA (5, 8). It is likely, therefore, that the value of gadolinium as a CTA contrast agent would be lessened in the setting of acute subarachnoid hemorrhage, because the attenuation of blood would be similar to that of the intravascular gadolinium.
The risks of gadolinium administration at the doses used here are not well understood, as pointed out in a pair of recent commentaries (9, 10). The potential risks revolve around nephrotoxicity and hyperosmolality; however, administration of gadolinium at similar doses has been without significant risk in most published series. Exacerbation of chronic renal failure in a subset of patients undergoing conventional angiography has been reported, and a 5% incidence of worsened renal failure after conventional angiography in patients with baseline renal insufficiency has been noted (9, 11–13). One of our patients developed mild, transient nausea and flushing immediately following injection of gadolinium. This reaction could have been related to the osmolality of gadopentetate dimeglumine (6.9 times higher than plasma osmolality) and, if so, might be avoided by using contrast agents, such as gadodiamide or gadoteridol, that are one-third less hyperosmolar. Extravasation of gadolinium can lead to local pain and serious injury, including skin necrosis. As with intravenous injection of iodinated contrast agent for CTA, infusions should be performed only in the presence of excellent venous access by using a large-bore catheter. Distal upper extremity veins should be avoided. Although many centers advocate the use of a test-bolus, or the “Smartscan” function, to time the preparation delay between the start of contrast material administration and scanning, we have found that a fixed 25-second delay is not only simpler for our CT technologists, but also provides consistently reproducible good image quality. In patients with atrial fibrillation or very low ejection fraction, we employ a 35–40-second delay.
We compared the costs for gadolinium and iodinated agents. At our institution, the cost of Magnevist (Berlex, Montville, NJ) required for CTA was six times higher, or about $150 more, than that of nonionic iodinated contrast material. There was minimal cost difference between Magnevist and iodixanol (Visipaque, Amersham Health, Princeton, NJ). In relative terms, however, the difference is likely to be small compared with the potential delay and costs incurred when CTA cannot be performed.
Gadolinium-enhanced CTA for vessels of the head and neck is technically feasible and is valuable in patients with contraindications to use of iodinated contrast material. Limitations of this approach include lower vascular contrast attenuation than is achieved with conventional CTA and requirement of high doses of gadolinium.
References
- Received November 30, 2003.
- Accepted after revision January 18, 2004.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}