
Article Figures & Data
Figures
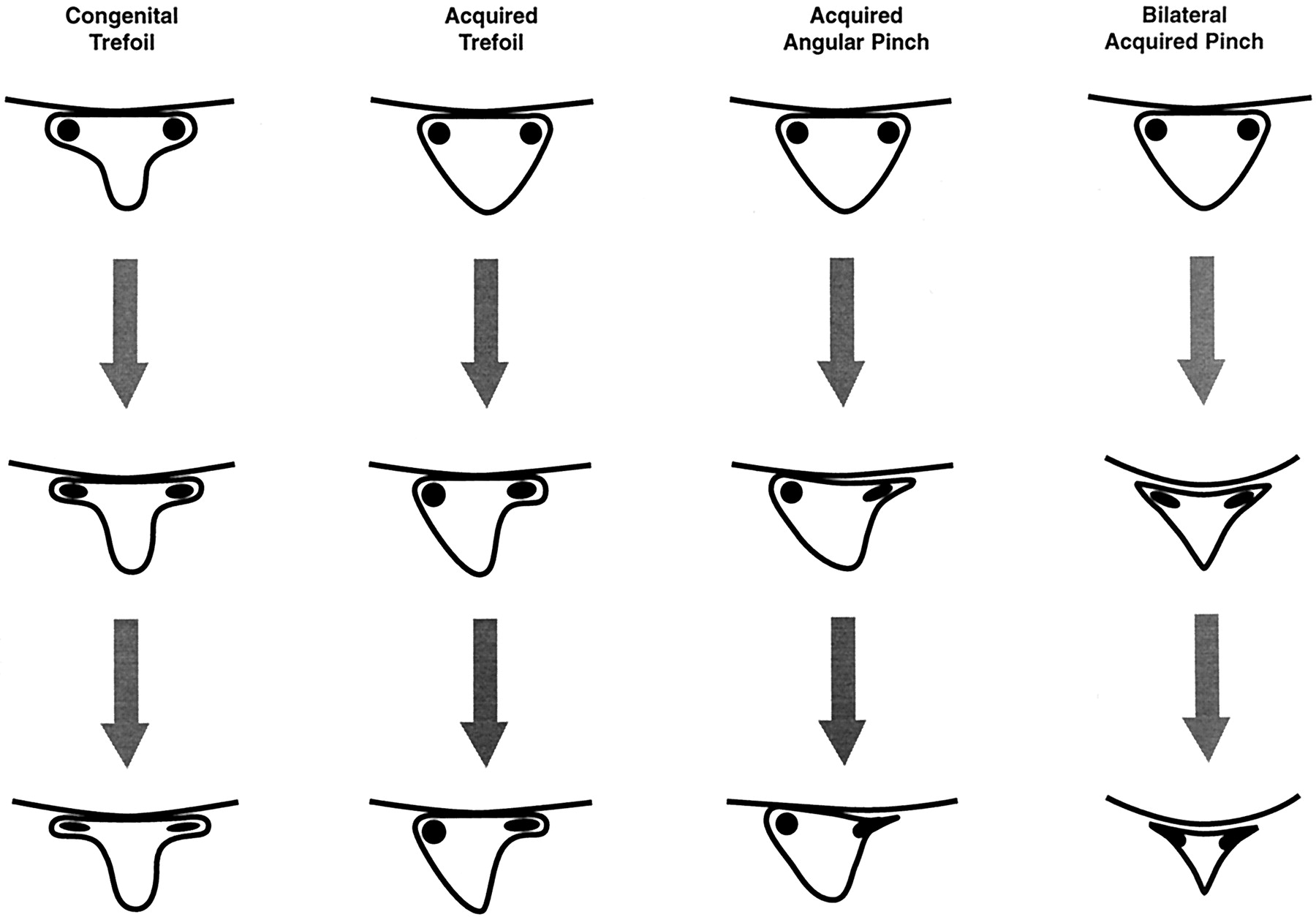
- Fig 1.
Illustrations show development of lateral recess stenosis.
Column 1, congenital trefoil canal. The lateral recess region becomes progressively narrowed because of either facet or endplate-disk margin degenerative changes. Column 2, acquired trefoil canal. Early facet degenerative changes and hypertrophy in a triangular canal develops a trefoil shape with the root positioned in a lateral recess niche. Progressive disk margin, endplate, or further facet degenerative changes leads to compression of the trapped root. Column 3, acquired angular pinch of the lateral recess. Simultaneous near equal facet, endplate, and disk margin degenerative changes lead to acute angle formation in the corner of the canal and lateral recess region. The root becomes progressively compressed in the lateral recess and may be medially deflected. Column 4, bilateral acquired angular pinch of the lateral recess. Bilateral facet, disk margin, and endplate degenerative changes can narrow the central spinal canal and the lateral recess region. This can produce both central spinal stenosis with cauda equina compression and individual nerve root compression within the abnormal lateral recess.
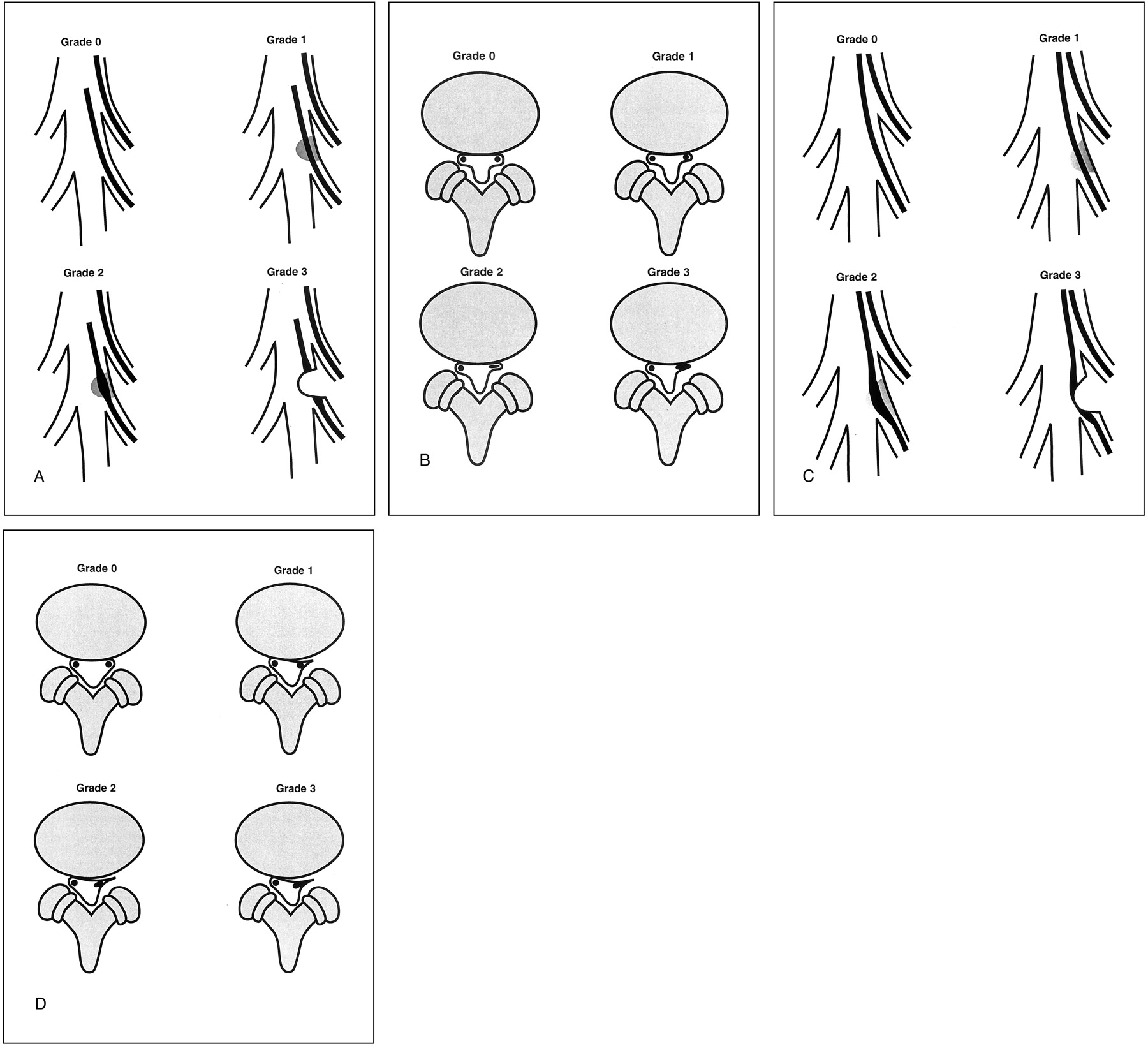
- Fig 2.
Illustrations shows grading system for lateral recess stenosis as revealed by myelography and MR imaging.
A, Grading system for trefoil lateral recess stenosis as revealed by myelography. Grade 0, appearance is normal. Grade 1, some narrowing of the lateral recess, with slight diminution of contrast material in the recess but no nerve root compression. Grade 2, further reduction in the size of the lateral recess, with some objectively identified nerve root flattening and reduced contrast material in the recess. Grade 3, complete obliteration of the lateral recess with a typical thumbprint-like appearance and complete obliteration of contrast material. The nerve root is compressed with visual widening and flattening.
B, Grading system for trefoil lateral recess stenosis as revealed by MR imaging. Grade 0, appearance is normal. Grade 1, narrowing of the lateral recess but no objective identification of root flattening or compression. Grade 2, further narrowing of the lateral recess with root flattening identified and some preservation of the space lateral to the root in the lateral recess. Grade 3, severe root compression with severe narrowing of the lateral recess and complete obliteration of any CSF space surrounding or lateral to the nerve root.
C, Grading system for acquired angular pinch lateral recess stenosis as revealed by myelography. Grade 0, appearance is normal. Grade 1, some narrowing of the lateral recess, with reduction of contrast material; some distortion of the anterior and posterolateral margin of the thecal sac due to facet or disk degenerative changes is usually seen. Grade 2, further narrowing of the corner of the canal, with reduction of contrast material in the lateral recess, some medial deflection of the nerve root, and some nerve root flattening due to compression; contrast material is still visualized lateral to the nerve root in the corner of the lateral recess. Grade 3, severe angular lateral recess compression with complete obliteration of contrast material lateral to the nerve root, root flattening and widening due to compression, and some medial root deflection.
D, Grading system for acquired angular pinch lateral recess stenosis as revealed by MR imaging. Grade 0, appearance is normal. Grade 1, early narrowing of the lateral recess due to anterior degenerative changes from disk bulge or endplate spur and posterolateral degenerative changes due to facet or ligament hypertrophy; nerve root is medially displaced, but no objective evidence of root flattening or compression is noted. Grade 2, further narrowing of the corner of the canal due to endplate, disk, and facet degenerative changes with early root compression identified; root is slightly widened or flattened and may be medially displaced and contrast material is still identified lateral to the nerve root. Grade 3, severe lateral recess impingement with definite root compression, no contrast material identified lateral to the root in the corner of the canal, and some medial root deflection.
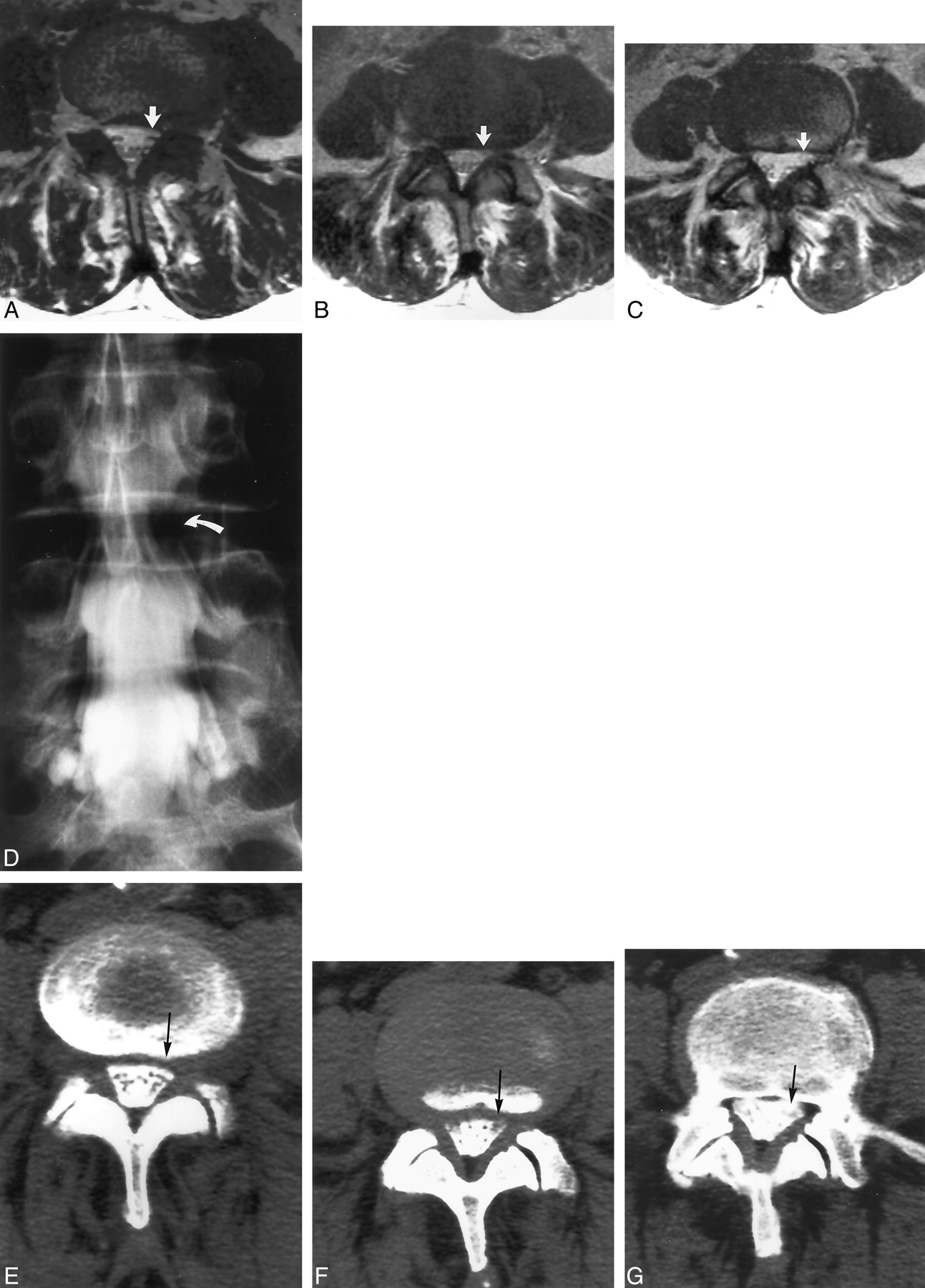
- Fig 3.
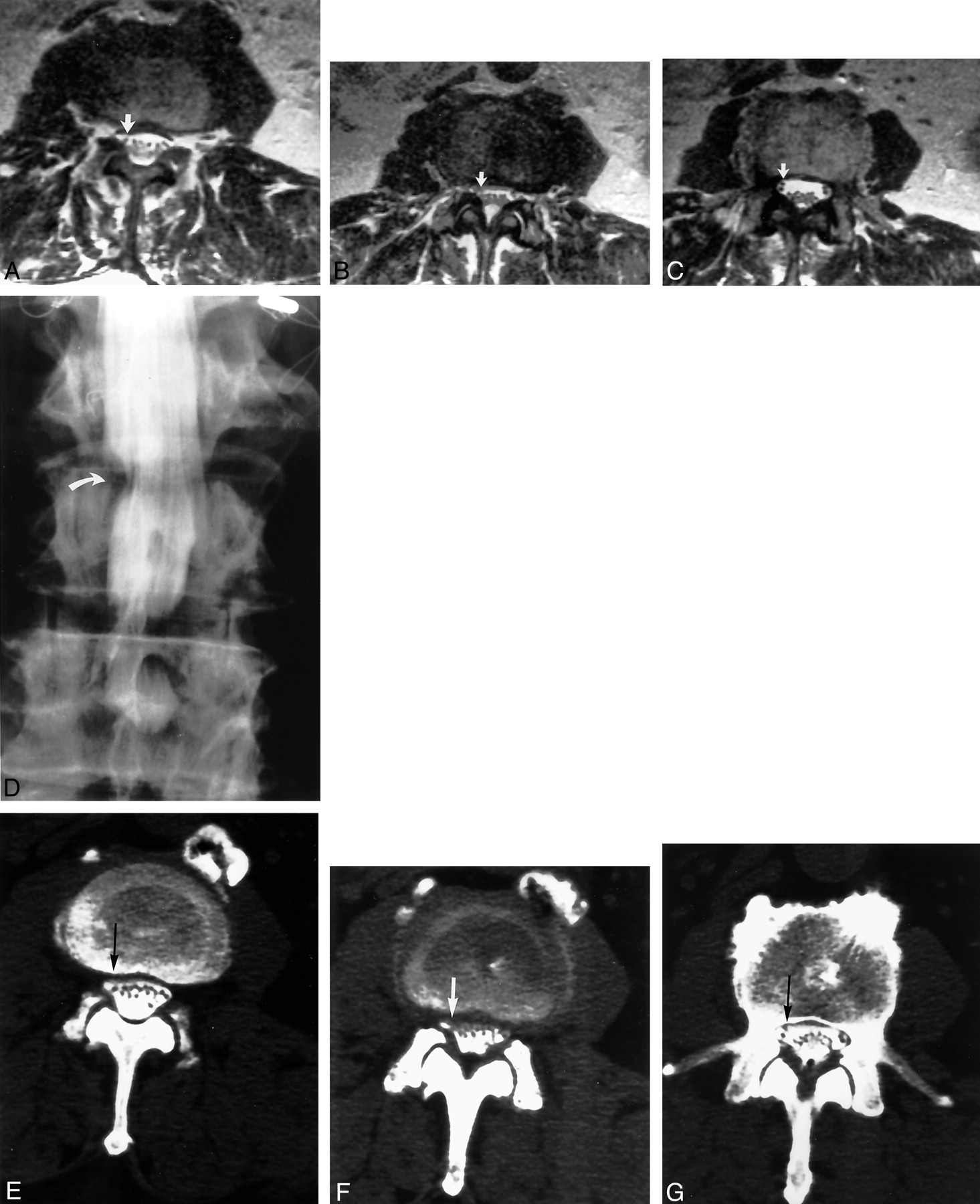
Images of a 66-year-old man with left leg pain and weakness.
A−C, Contiguous axial view T2-weighted MR images obtained at the L4–L5 level. Canal distortion is present on the right at the disk margin. Narrowing of the left lateral recess was judged to be root compression by one observer but only canal distortion by the other observer because of visualization of the roots free within the canal in the left lateral recess region (arrows).
D, Conventional myelogram shows left lateral recess root compression at L4–L5 (curved arrow). Root compression was confirmed at surgery. The patient achieved complete recovery from leg pain after decompression.
E−G, Contiguous axial view post-myelogram CT images obtained at the L4–L5 level show slight canal distortion on the right but a normal appearing left lateral recess (arrows), similar to the findings of the MR imaging study. Both observers labeled this left lateral recess as noncompressive (grade 1).
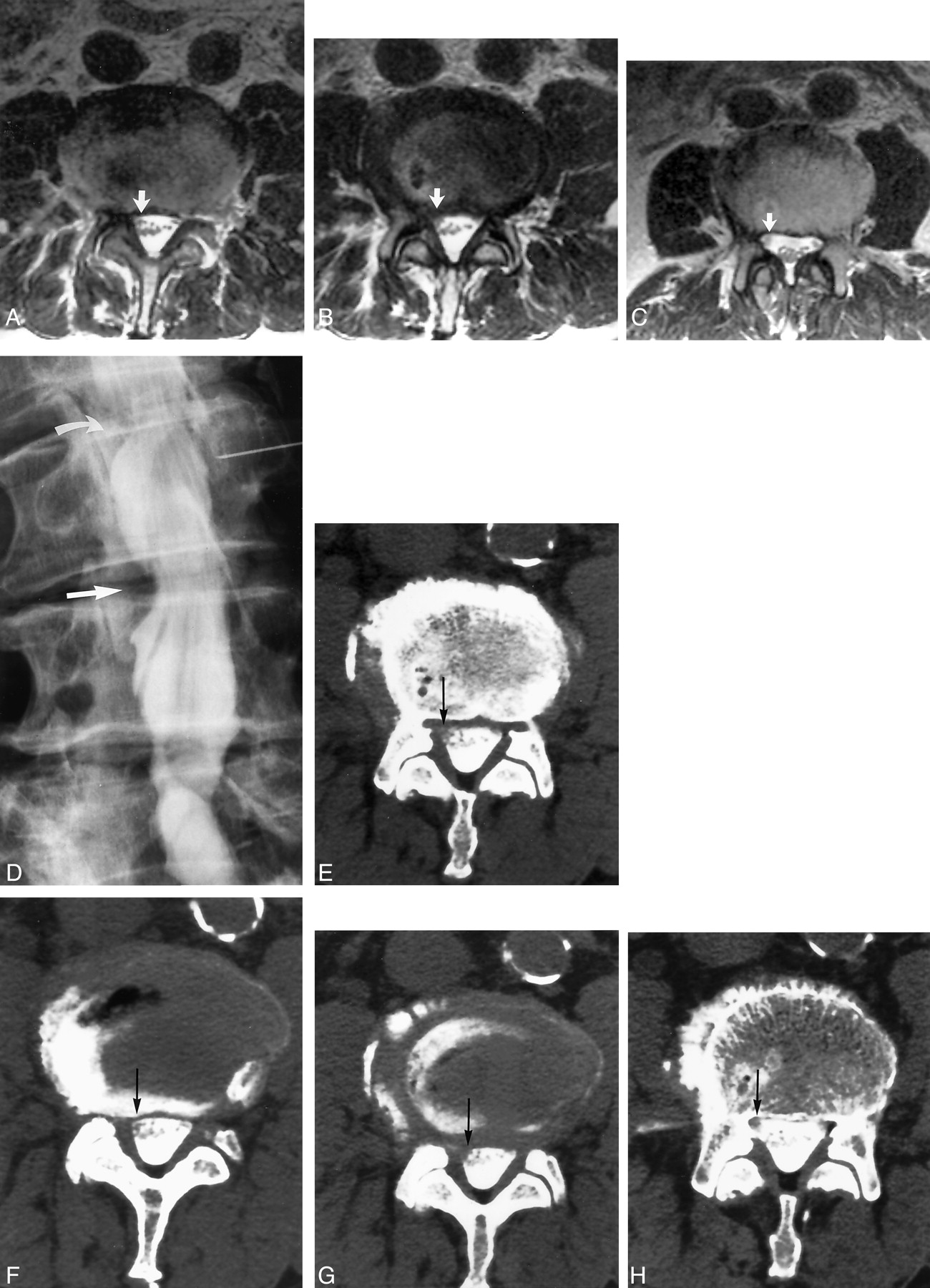
- Fig 4.
Images of an 82-year-old man with right lower extremity weakness and pain, primarily in the upper leg and thigh. Electromyography suggested right L2, L3, and L4 abnormality.
A−C, Contiguous axial view T2-weighted MR images obtained at the L3–L4 level. Root compression was identified by one observer at L3–L4 on the right (arrows) but was labeled noncompressive (grade 1) by the second observer. Root compression was also correctly identified on the right by both observers at L2–L3 (grades 2 and 3).
D, Conventional myelogram shows right-sided root compression at L2–L3 (curved arrow) and L3–L4 (straight arrow), identified and assessed as grades 2 and 3 by both observers. The patient underwent right-sided keyhole decompression at L2–L3 and L3–L4. Severe root compression was surgically identified at both levels, and the patient achieved resolution of leg pain after surgical decompression.
E−H, Contiguous axial view post-myelogram CT images obtained at the L3–L4 level show slight angular distortion on the right lateral recess (arrows). The nerve roots within the canal are slightly more prominent at this level and may be somewhat edematous. Both observers labeled this lateral recess root compressive (grade 2).
- Fig 5.
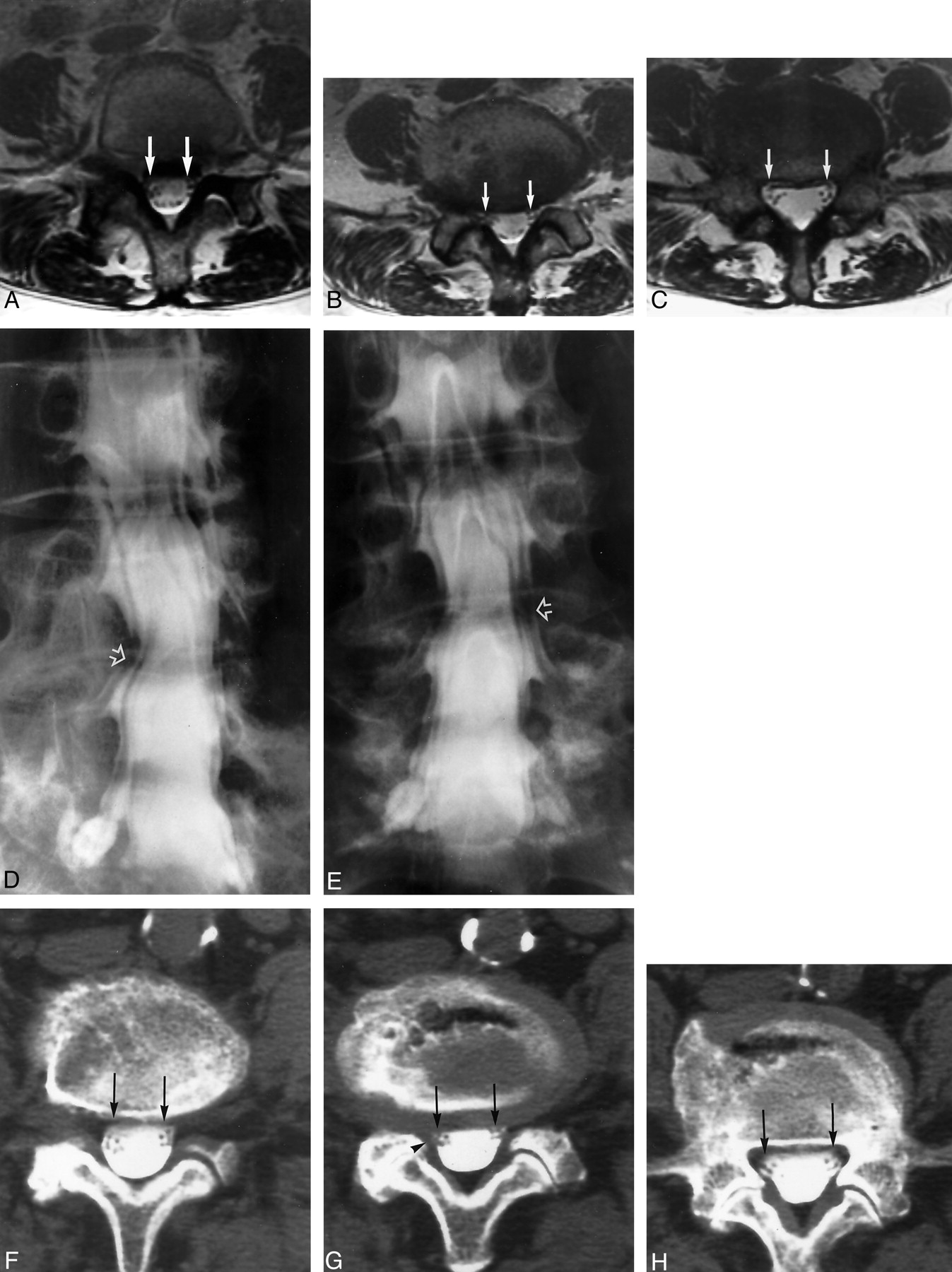
Images of a 70-year-old man with bilateral leg pain and weakness, with reduced sensation in both upper and lower legs.
A−C, Contiguous axial view T2-weighted MR images show a trefoil-shaped canal at L2–L3 that was judged to be root compression (grade 2) on the right by one observer because of the small recess size but was judged to be noncompressive (grade 0) by the other observer (arrows).
D, Conventional myelogram shows right-sided root compression at L2–L3 (curved arrow), assessed as grades 2 and 3 by both observers. Compression at L3–L4 was also identified by both observers by using MR imaging and conventional myelography. Surgical findings revealed evidence of root compression on the right at L2–L3 as well as at L3–L4. The patient was free of leg pain at the time of postoperative discharge.
E−G, Contiguous axial post-myelogram CT images obtained at the L2–L3 level show narrowing of the right lateral recess (arrows) with a normal appearance of the left lateral recess. One observer graded the right lateral recess as abnormal (grade 2), and the second observer graded this recess as narrow but not compressive (grade 1). Observer grading in this instance was reversed between MR imaging and CT myelography. One observer graded the MR imaging findings as root compressive but graded the CT myelography findings as not compressive. The other observer graded the MR imaging findings as compressive but graded the CT myelography findings as narrow but not root compressive.
- Fig 6.
Images of a 71-year-old female with left leg pain.
A−C, Contiguous axial view T2-weighted MR images obtained at the L4–L5 level were judged as normal bilaterally and assessed as grades 0 and 1 by both observers (arrows).
D and E, Conventional oblique and anteroposterior myelogram images were judged grade 2 bilaterally by both observers at L4–L5 (open arrows). Decompressive laminectomy at L4–L5 reported bilateral root compression in the lateral recess at L4–L5. The patient experienced significant improvement in leg pain at the time of discharge.
F−H, Contiguous axial post-myelogram CT images obtained at the L4–L5 level show some canal asymmetry in the lateral recesses (arrows), with slight distortion of the canal in the lateral recess on the right (G, arrowhead). One observer labeled this distortion as root compressive, whereas the other labeled this level as normal in the lateral recesses bilaterally.
- Fig 7.
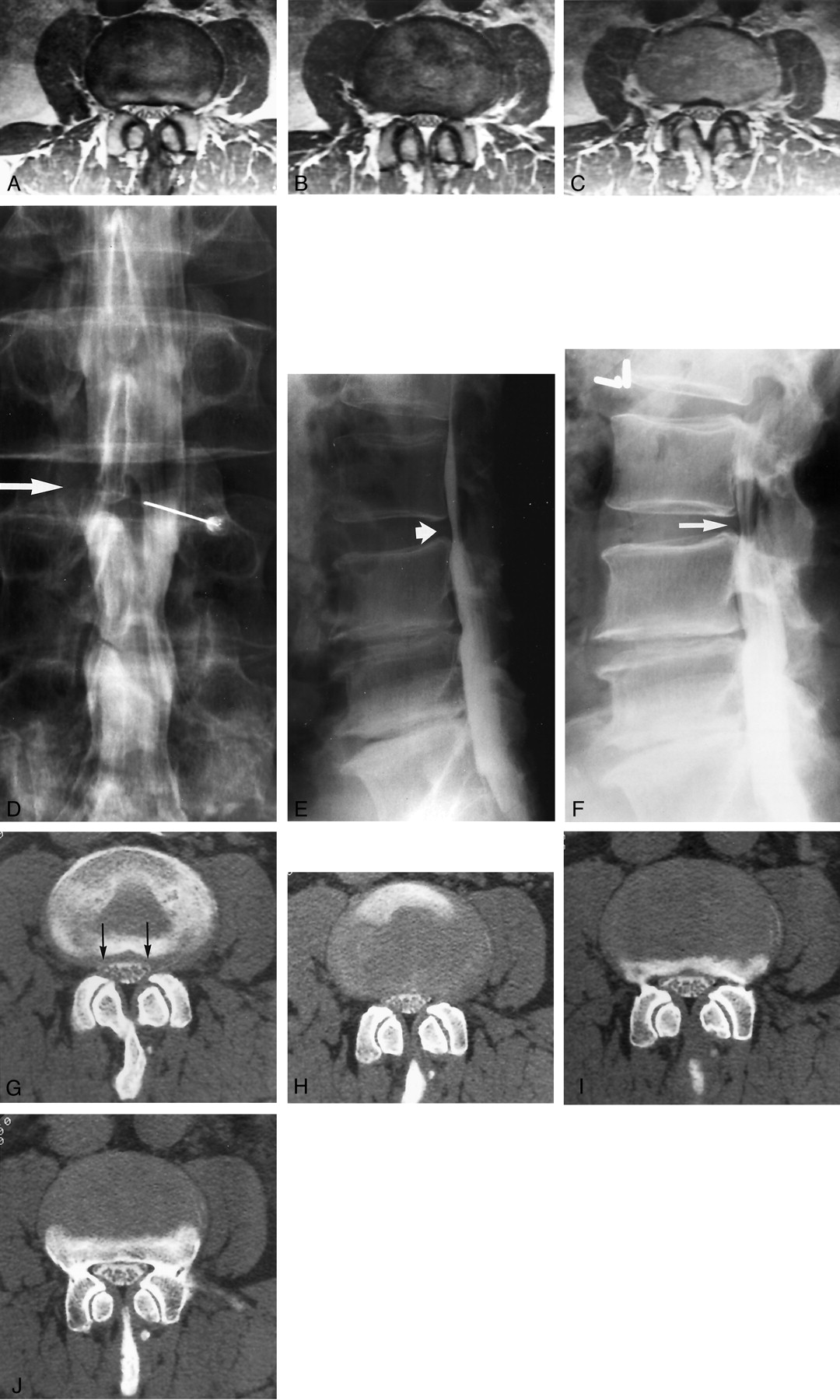
Images of a 56-year-old man with right leg pain and anterior thigh pain. Neurogenic claudication was not present. The patient had a history of surgery at L3–L4 and L4–L5.
A−C, Contiguous axial view proton density–weighted MR images show a small canal at L2–L3 but no overt evidence of root compression. Both observers labeled this as grades 0 and 1 bilaterally.
D, Anteroposterior view conventional myelogram obtained with the patient in the prone position shows a relatively normal canal at L2–L3 (arrow).
E, Lateral view conventional myelogram obtained with the patient in the prone position shows a normal canal at L2–L3 (short arrow).
F, Lateral view conventional myelogram obtained at the L2–L3 level with the patient in the standing extended position shows reduction in canal size with some posterior defect likely related to buckling of the ligamentum flavum while in extension, leading to some degree of spinal stenosis (arrow). Surgical findings documented lateral recess root compression bilaterally at L2–L3. Postoperatively, the patient achieved moderate recovery of strength and sensation, with improvement in right leg pain by the time of discharge.
G−J, Contiguous axial post-myelogram CT images obtained at the L2–L3 level show a small canal and slight lateral recess distortion bilaterally (G, arrows). One observer graded this level as small lateral recesses but no root compression (grade 1), and the other observer graded this as root compressive (grade 2).







Tables
Grade Myelography CT Myelography or MR Imaging 0 Normal Normal 1 Reduced contrast material within the lateral recess, indentation on the dural sac, nerve root is normal and unaffected Reduced size of the corner of the lateral canal or recess; trefoil shape to the lateral recess, either congenital or acquired; early acute angular narrowing of the corner of the canal and thecal sac; nerve root is visualized and not widened, flattened, or altered 2 Reduced contrast material within the lateral recess (not obliterated); indentation on the dural sac; nerve root is flattened, widened, or laterally pinched and medially displaced due to canal corner changes Reduced size of the corner of the lateral canal or lateral recess, trefoil shape and narrowing of the lateral recess, angular pinch-like shape and narrowing of the lateral canal and thecal sac, nerve root judged compressed in the small trefoil recess or angled pinch but recess judged not totally obliterated, nerve root may be deviated medially 3 Complete obliteration of contrast material from the lateral recess or corner of the canal; thumbprint-like obliteration of contrast material in the lateral recess; severe lateral pinch of the corner of the canal with obliteration of contrast material at the lateral margin; nerve root is trapped in the thumbprint compression, widened-flattened on the thumbprint, displaced medially and widened and flattened laterally due to lateral canal corner changes Severe facet hypertrophy and disc/end plate changes, no CSF or space identified in the lateral recess or corner of the canal, severe angular pinch of the lateral corner of the canal, root may or may not be clearly visible, root may be seen coursing through the compressed lateral recess, root may be seen as medially displaced Myelography CT Myelography MR Imaging Root Compression Grades 2 and 3 No Root Compression Grades 0 and 1 Root Compression Grades 2 and 3 No Root Compression Grades 0 and 1 Root Compression Grades 2 and 3 No Root Compression Grades 0 and 1 Reader 1 54 4 36 22 41 17 Reader 2 55 3 36 22 42 16





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}