
Abstract
Summary: We present the case of a flight passenger who experienced acute and severe headache during landing. MR imaging was performed because the patient had a history of vascular malformation and revealed an incidental venous angioma. A mass lesion in the frontal sinus, consistent with submucosal hematoma secondary to barotrauma, was thought to be the cause of the headache. To our knowledge, this is the first case of sinus barotrauma described in the radiologic literature and the first to describe the associated MR imaging findings.
Sinonasal barotrauma is caused by a rapid change of ambient pressure. In the presence of compromise to the normal sinus outflow, a pressure gradient occurs, which is the basic cause of the traumatic event. Divers and aviators are the two main populations that are affected by barotrauma. Radiologic correlations are scarce and include only plain film records. We present a case of frontal sinus submucosal hematoma secondary to barotrauma and report the associated MR imaging findings.
Case Report
A 43-year-old man experienced abrupt and severe right-sided frontal headache that occurred with the descent of a commercial jet airplane and became excruciating at the time of landing. The pain gradually improved, disappearing after a few hours. The patient’s medical history was remarkable for a right-sided vascular malformation of the brain that was discovered 13 years before the episode reported herein, after a different type of headache, which had not recurred. Previous MR images and medical records were not available. There was no history of recent upper respiratory tract infection or previous sinonasal disease. Physical examination, including nasal endoscopy, revealed a deviated nasal septum and hypertrophy of the inferior conchae. The nasal mucosa was edematous and inflamed. The remaining results of the examination were normal. Because of the history of vascular malformation, MR imaging was performed 1 week after the incident. It revealed only a large typical developmental venous anomaly, originating from the subependymal veins of the superior aspect of the right lateral ventricle, with no other brain abnormalities (not shown). Additionally, a polypoid mass was present in the right frontal sinus (Fig 1). The mass was hyperintense on both T1- and T2-weighted images and did not enhance with the administration of contrast agent.

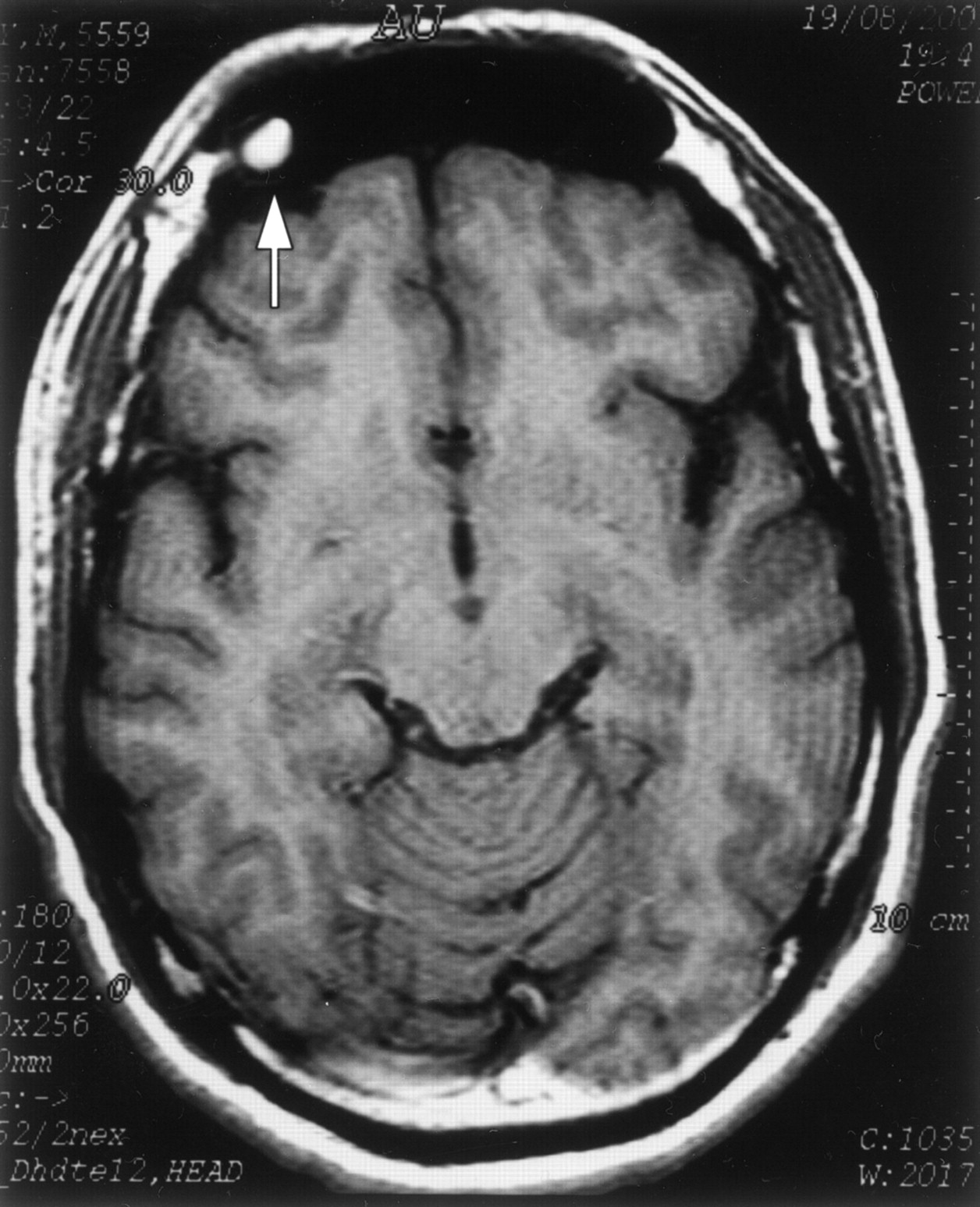
Images from the case of a 43-year-old man who experienced an abrupt and severe right-sided frontal headache that occurred with the descent of a commercial jet airplane and became excruciating at the time of landing. Imaging showed that a polypoid mass was present in the right frontal sinus.
A, Axial view spin-echo T1-weighted MR image obtained through the frontal sinuses. A rounded mass in the right frontal sinus (arrow), which was hyperintense on both sequences, was consistent with submucosal hemorrhage.
B, Fast spin-echo T2-weighted MR image.
Considering the history and the MR imaging appearance, it was thought that the mass lesion was a submucosal hematoma secondary to barotrauma and that the developmental venous anomaly was incidental. MR imaging performed 2 months later revealed only a small remnant of the lesion (Fig 2). Clinical follow-up performed 6 months later showed that the patient was asymptomatic.

Axial view T1-weighted MR image obtained at a follow-up study 2 months later. Only a small remnant is seen (arrow). Note that because of differences in angulation of the axial plane, the brain morphology is different from that shown in Figure 1 but the morphology of the frontal sinus is similar.
Discussion
Sinonasal barotrauma is the result of a rapid change in ambient pressure that is associated with sinus outflow compromise, such as inflammatory mucosal thickening, polyps, and/or structural deviations (1–5). This occurs most commonly in flight passengers and scuba divers.
Rapid increase in ambient pressure, as in airplane or diving descent, is the most common mechanism. The pressure in the obstructed sinus remains relatively low, resulting in a vacuum effect, sometimes referred to in the literature as “the squeeze.” This vacuum effect may be stressful to the sinus mucosal lining and may cause mucosal edema, serosanguineous exudate, and submucosal hematoma. This may cause pain, sometimes abrupt and severe, and possible epistaxis. Referred pain and numbness may occur as a result of pressure on branches of the trigeminal nerve in the maxillary sinus (5).
Radiologic reports of sinus barotrauma are scarce and include only plain film records (1–3, 5). Comparable with the findings described above, these include mucosal thickening, fluid levels, polypoid masses, and complete sinus opacification.
Rapid decrease in ambient pressure is a much less common cause of sinus barotrauma with different mechanism and results. When the ambient pressure decreases, the pressure inside the affected sinus remains relatively high, sometimes referred to as the “reversed squeeze.” When a defect in the sinus wall exists (1, 4, 5), the positive pressure may result in pneumocephalus, periorbital or orbital emphysema, and, rarely, meningitis. Mucosal edema and some bleeding may occur (1) but are less prominent than in the squeeze situation.
Weissman et al (1) suggested a clinical grading of sinus barotrauma according to severity. With grade 1, transient discomfort is present over the affected sinus and clears promptly. The results of plain radiography are normal, and only slight mucosal edema may be present. With grade 2, pain is present and lasts <24 hr. Plain radiography may reveal mucosal thickening. These two relatively mild grades may occur either in the squeeze or reversed squeeze situations. Grade 3, which is the most severe grade, results in abrupt and severe pain lasting occasionally >24 hr and is always the result of the squeeze. Plain films may show a fluid level and/or a polypoid mass representing submucosal hemorrhage and free bloody exudate.
Our diagnosis of sinus barotrauma was based on the association of acute pain with rapid change in atmospheric pressure, the clinical improvement and then resolution of the lesion shown by MR imaging, and the frontal sinus lesion signal intensity being consistent with subacute hematoma during the extracellular methemoglobin phase, which is appropriate for the assumed age of the lesion. The differential diagnoses of an unenhanced mass lesion in the paranasal sinuses that is hyperintense both on T1- and T2-weighted images include a mucocele and the rare sinus cholesterol granuloma. Lack of sinus expansion or erosion, the clinical setup, and the prompt spontaneous resolution indicated the mass in our case was submucosal bleeding secondary to barotrauma.
The diagnosis of sinus barotrauma is usually made clinically, and imaging is not necessary. In cases of repeated barotrauma, a correctable cause of ostial obstruction should be looked for (4). Successful surgical endoscopic enlargement of the natural ostium was reported in aviators with recurrent sinus barotrauma (6). In our case, the MR imaging was performed because of the history of vascular malformation of unknown type, feared to be related to the headache but proved to be only incidental.
Aviators or divers with nasal congestion of any cause (eg, upper respiratory tract infection, sinus infection, allergy) should be appropriately treated with antibiotics and/or decongestants. However, these patients are warned that they may still have difficulty in clearing the sinuses and that this difficulty could result in significant morbidity or disabling injury (4). To the best of our knowledge, this is the first report of sinus barotrauma in the radiologic literature and the first to describe MR imaging findings in such a case.
- Received May 9, 2002.
- Accepted after revision July 16, 2002.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}