
Article Figures & Data
Figures
- fig 1.
Overall average score for each imaging technique. Note.—SD = source data; MPR = multiplanar reformat; IA DSA = intraarterial digital subtraction angiography; MIP = maximum intensity projection; 3D = three-dimensional isosurface reconstruction.
- fig 2.
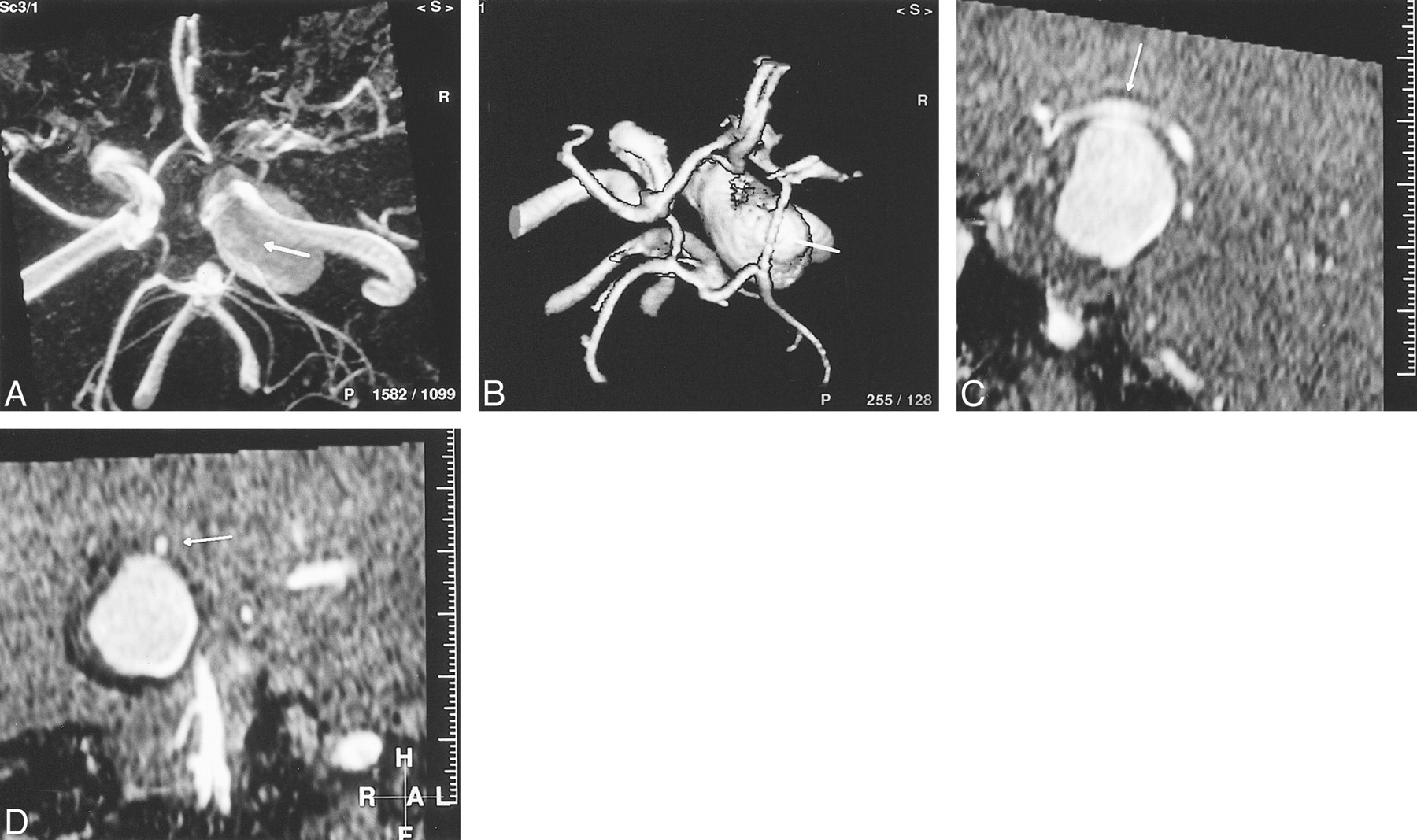
A 55-year-old woman presented with intractable pain and a complete right CN III palsy caused by pressure effect from a giant (25 mm), fusiform, intracavernous internal carotid artery aneurysm. The circle of Willis should be scrutinized as part of the assessment prior to endovascular balloon occlusion of the parent vessel.
A, TOF-MIP MRA (100/20/1) from above and slightly from the right. The right posterior communicating artery (arrow) cannot be differentiated from aneurysm by MIP-MRA findings. The ipsilateral anterior cerebral artery is also poorly demonstrated.
B, TOF-3D-isosurface MRA (100/20/1), similar projection to A. The posterior communicating artery (arrow) can now be clearly separated from aneurysm. The ipsilateral anterior communicating artery is of increased caliber compared with the MIP-MRA projection.
C, TOF-MPR MRA (100/20/1), parasagittal view. The relationship of the posterior communicating artery (arrow) to the aneurysm can be clearly seen along its whole length on this projection. The artery is in contact with aneurysm at its apex.
D, TOF-MPR MRA (100/20/1), coronal view. By scrolling along the posterior communicating artery (arrow) in the coronal plane, its relationship to the aneurysm is clearly depicted.
- fig 3.
A 48-year-old woman presented with an SAH secondary to an anterior communicating artery aneurysm rupture. Diagnostic IA-DSA showed multiple aneurysms.
A, TOF-3D-isosurface MRA (100/20/1), right periorbital view. There is some minor artifact due to patient movement. The anterior communicating artery aneurysm (short broad arrow) appears to arise from the right A1/A2 junction. A terminal left internal carotid artery aneurysm is also visible (long thin arrow).
B, TOF-MPR MRA (100/20/1), coronal slice through the anterior communicating artery complex. Scrolling through, no communication is seen between the left A1 segment (thin short arrow) and aneurysm (short broad arrow). The aneurysm is continuous with the right A2 segment (long arrow).
C, IA-DSA, left periorbital projection. The anterior communicating and left terminal internal carotid artery aneurysms are clearly seen (arrows). There are also two discrete middle cerebral artery aneurysms. The anterior communicating artery aneurysm only filled from a left-sided injection. If one were to have planned endovascular treatment on the basis of the MRA findings, the approach would have been via the right internal carotid artery.
- fig 4.
A 62-year-old woman presenting with a left CN III palsy due to posterior communicating artery aneurysm.
A, IA-DSA of left common carotid artery, lateral projection. A large left, saccular, posterior communicating artery aneurysm with a discrete narrow neck is seen well.
B, TOF-MIP MRA (100/20/1), similar projection to that of A. Streamlining artifact is seen within the internal carotid artery, and there is signal loss within the aneurysm itself.
C, TOF-3D-isosurface MRA (100/20/1), similar projection to that of A and B. The posterior communicating artery aneurysm (arrow) appears identical to its depiction by IA-DSA.
D, Axial-source TOF image (100/20/1). The true lumen of the posterior communicating artery aneurysm is depicted as high signal, but this is surrounded by concentric mixed signal rims representing intramural thrombus (arrow). The presence of thrombus is not appreciated on the IA-DSA image. The aneurysm is significantly larger than the IA-DSA and postprocessed MRA images suggest.
- fig 5.
A 45-year-old woman presented with SAH due to rupture of an anterior communicating artery aneurysm.
A, Diagnostic IA-DSA of left common cartotid artery, frontal projection. The anterior communicating artery aneurysm is seen, but its relationship with the left A2 segment is not clear. A submental vertical projection was not obtained.
B, TOF-MIP MRA (100/20/1), submental vertical projection. It can now be appreciated that there is a bifid anterior communicating artery (long arrow). The aneurysm (short arrow) arises from the junction between the left A2 and the upper limb of the anterior communicating artery. On the MIP-MRA image, the aneurysm appears tubular and of narrower calibre than is suggested by the IA-DSA image.
C, TOF-3D-isosurface MRA (100/20/1), similar projection to that of B. The lower limb of the anterior communicating artery is again clearly visible (long arrow). The morphologic characteristics of the aneurysm (short arrow) depicted by this technique are more similar to those shown by IA-DSA.
D, IA-DSA of the anterior communicating artery aneurysm post GDC embolization. Prior manipulation of the MRA has allowed the appropriate projection to be chosen. Only the distal part of the aneurysm would retain a coil, leaving a significant remnant.





Tables

- TABLE 2:
Wilcoxon matched-pairs signed-ranks test (IA-DSA vs. other techniques)
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Usefulness of high-resolution three-dimensional proton density-weighted turbo spin-echo MRI in distinguishing a junctional dilatation from an intracranial aneurysm of the posterior communicating artery: a pilot study
- Aneurysm outflow angle at MRA as discriminant for accurate diagnosis and differentiation between small sidewall cerebral aneurysms and infundibula
- Computer-Assisted Detection of Cerebral Aneurysms in MR Angiography in a Routine Image-Reading Environment: Effects on Diagnosis by Radiologists
- Diagnosing Intracranial Aneurysms With MR Angiography: Systematic Review and Meta-Analysis
- Angiographic CT with Intravenous Contrast Injection Compared with Conventional Rotational Angiography in the Diagnostic Work-Up of Cerebral Aneurysms
- Three dimensional CT angiography versus digital subtraction angiography in the detection of intracranial aneurysms in subarachnoid hemorrhage
- Atrial myxoma as a cause of stroke: case report and discussion