
Abstract
BACKGROUND AND PURPOSE: Several techniques have been used to image the nasolacrimal system, providing functional (dacryoscintigraphy) or morphologic (dacryocystography, CT dacryocystography [CTD]) information. Using gadopentetate dimeglumine–diluted solution injected into the lacrimal canaliculus or instilled into the conjunctival sac, we compared the sensitivity of MR dacryocystography (MRD) with that of CTD.
METHODS: Eleven healthy volunteers and 25 patients affected by primary epiphora (21 patients) or postsurgical recurrent epiphora (four patients) underwent MRD after the topical administration of contrast media or cannulation of the lacrimal canaliculus. The MR imaging findings were compared with irrigation and CTD data. All patients underwent surgical treatment (dacryocystorhinostomy), which served as a standard of reference for confirming the MRD findings.
RESULTS: The topical administration of contrast-enhanced saline solution and the injection of contrast-enhanced saline solution after cannulation were always well tolerated. In healthy volunteers, outflow of contrast media was always revealed by MRD. Eight (32%) of 25 patients with epiphora had stenosis proximal to the lacrimal sac revealed by MRD, whereas 17 (68%) of 25 showed a dilated lacrimal sac and nasolacrimal duct stenosis, as confirmed by surgical findings. The findings of MRD after the topical administration of contrast medium and MRD after cannulation of the lacrimal canaliculus were comparable with irrigation or CTD data for all patients except one.
CONCLUSION: In patients with epiphora, MR imaging performed after the topical administration of diluted contrast material can reveal stenosis of the lacrimal apparatus and can be added to the standard orbital imaging protocol when lacrimal system involvement is suspected.
Radiologic investigation of the nasolacrimal system has, to date, been performed principally by cannulating the lacrimal canaliculi and injecting iodinate or radionuclide contrast medium. Dacryocystography reliably shows morphologic characteristics of the nasolacrimal system, revealing congenital or acquired stenosis (1), whereas dacryoscintigraphy evaluates physiological lacrimal drainage. More recently, CT dacryocystography (CTD) has been assessed (2, 3). Nevertheless, dacryocystography, dacryoscintigraphy, and CTD have several drawbacks. Dacryocystography and dacryoscintigraphy do not show the orbital soft tissues, whereas dacryocystography and CTD require cannulation of one of the lacrimal canaliculi, precluding adequate functional evaluation of the lacrimal drainage. Moreover, delivery of ionizing radiation occurs with these techniques. The absorbed dose to the lens has been calculated as 0.04 to 0.2 mSv for dacryocystography, 1.8 to 2.6 mSv for CTD, and up to 1.09 mGy/MBq for dacryoscintigraphy (4–6).
Topical instillation of iodinate and paramagnetic contrast media for use with CT and MR imaging has also been reported (7–9). MR imaging of the orbit provides superior soft-tissue contrast, which is improved by dedicated surface coils (10) and a fat-suppression technique (11). Using a diluted solution of commercially available gadopentetate dimeglumine contrast medium, we compared the results of the MR dacryocystography (MRD) technique with the CTD and surgical findings.
Methods
From November 1996 to October 1997, 11 healthy volunteers (seven men and four women) with no history of eye disease and 25 patients (four men and 21 women) affected by primary nasolacrimal outflow impairment (epiphora) (21 patients) or postsurgical recurrent epiphora (four patients) underwent MRD as a prospective study. In four of 25 patients, restenosis of the lacrimal ducts was suspected as a complication of previous dacryocystorhinostomy. The study was formally approved by our local university research board, and informed consent was obtained from volunteers and patients.
Patients with epiphora first underwent CTD. The technique consisted of cannulating the inferior lacrimal canaliculus and injecting 5 mL of iodinate contrast medium (Iopamiro 300; Bracco) and then performing axial-view, 2-mm-thick, contiguous-section CT with soft-tissue and bone windows. Coronal reformations were obtained in five cases. None of the healthy volunteers underwent CTD.
Four to 7 days later, the MRD study was performed using a 0.5-T MR imaging system (Vectra; GE) and quadrature head coil. For morphologic evaluation of the lacrimal system in healthy volunteers and patients, contiguous axial T1-weighted spin-echo imaging (500/22 [TR/TE]; number of acquisitions, one) was performed before and after the fat-suppression technique. One to 3 mL of gadodiamide dimeglumine (Magnevist per os; Shering) diluted with sterile saline solution (1:10) was then injected into the inferior lacrimal canaliculus via a lacrimal cannula. We found this concentration to be sufficient for optimal contrast when using a middle-field unit. Axial T1-weighted imaging was then repeated, before and after a fat-suppression pulse sequence was added.
One week later, the volunteer/patient returned for functional study. Evaluation of spontaneous lacrimal drainage was obtained using the same diluted contrast medium solution. The topical administration of three to five drops every 5 minutes into the conjunctival sacs was begun 15 minutes before MR imaging. An ophthalmologist was present during the administration of the topical contrast material. The diluted solution was always well tolerated, and local anesthesia was unnecessary.
Two neuroradiologists blindly evaluated the images, comparing CTD with MRD studies and evaluating the site of the stenosis and extravasation of contrast-enhanced tears. Consensus regarding CTD and MRD findings and regarding MRD after the topical administration of contrast media (MRDt) versus MRD after cannulation of the lacrimal canaliculus (MRDc) was always reached by the two neuroradiologists.
The sensitivity of MRDc versus MRDt was also investigated. Surgical confirmation (dacryocystorhinostomy) as a standard of reference was performed in all the patients affected by epiphora.
Results
Results are summarized in the Table. In the healthy volunteers, the lacrimal sac and duct were opacified bilaterally by using the topical administration of gadolinium and MR imaging (MRDt), by direct injection and MR imaging (MRDc), or by direct injection and CT (CTD).
Results of MR and CT dacryocystography in 11 healthy volunteers (22 eyes) and 25 patients with epiphora (50 eyes)
Among the patients with epiphora (Fig 1), CTD showed that 32% (eight of 25 patients) had stenosis proximal to the lacrimal sac. Surgical evaluation confirmed sclerotic change as a sequela of previous infection at the level of the lacrimal canaliculus or common lacrimal duct. CTD showed that 68% (17/25) of patients had a dilated lacrimal sac and presumed stenosis of the nasal lacrimal duct, and surgical findings confirmed nasolacrimal duct stenosis secondary to sclerotic tissue. MRDt and MRDc revealed findings that were comparable with the CTD and surgical findings (Table, Fig 2) in all except one patient who was affected by dacryocystophlegmon. In that case, MRDt did not show any contrast material entering into the lacrimal sac, whereas MRDc revealed partial inflow after forced injection. This false-positive result for presaccular stenosis revealed by MRDt was probably related to diffuse exudate filling a dilated lacrimal sac, preventing normal contrast-enhanced solution inflow (Fig 3). The use of fat saturation improved the contrast between the opacified lacrimal system and surrounding healthy tissue (Fig 4).

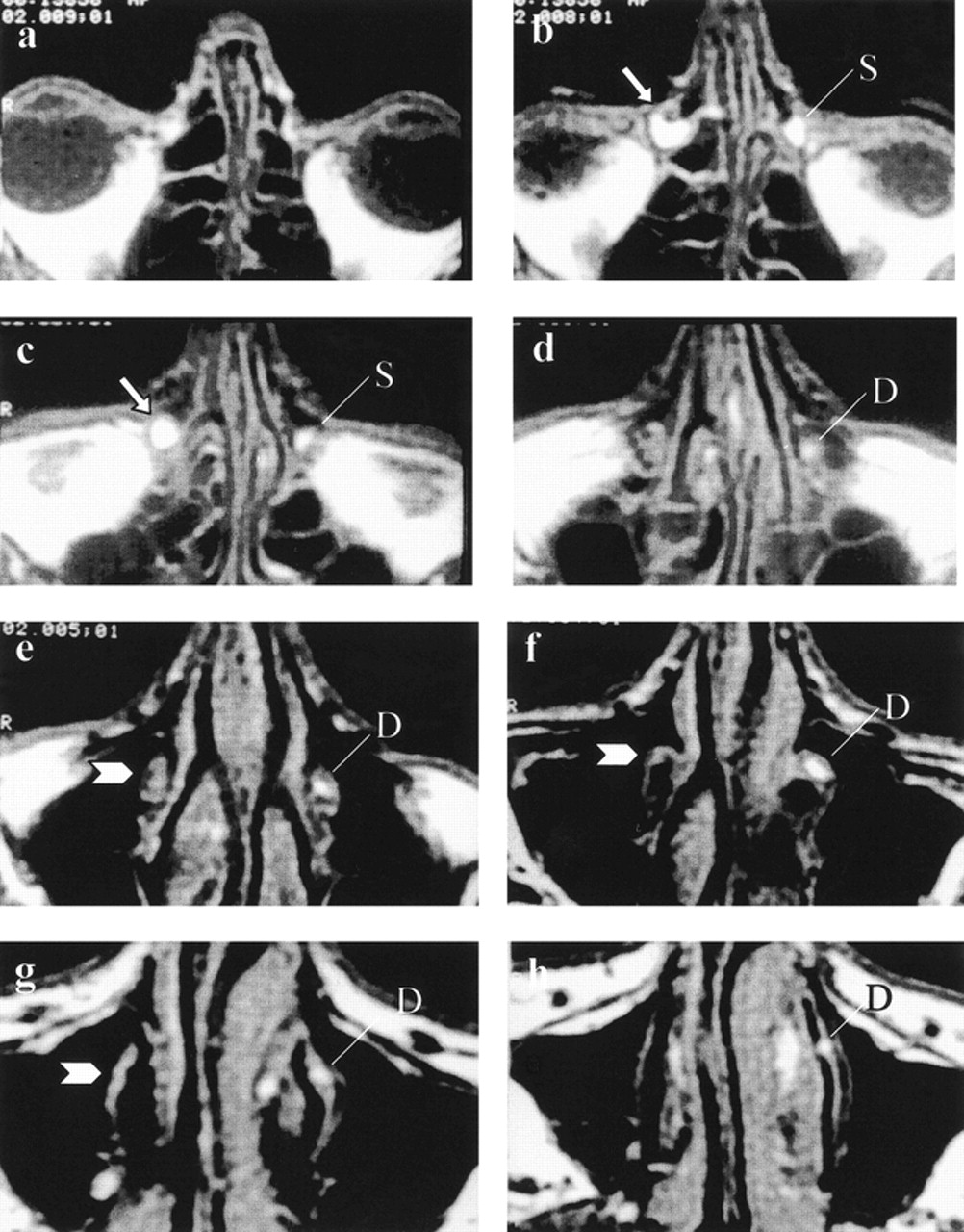
MRD images of a patient with right postlacrimal sac stenosis and healthy left lacrimal system. Axial T1-weighted (600/30/1 [TR/TE/excitations]) images obtained after the topical administration of diluted gadopentetate solution from the nasolacrimal duct to the orbital level. On the left side, healthy drainage of contrast-enhanced tear can be appreciated inside the lacrimal sac (L) and the nasolacrimal duct (N). On the right side, postsaccular stenosis causes dilation of the right lacrimal sac (arrows), and no contrast media is appreciated down into the ipsilateral nasolacrimal duct (arrowheads).
a, Nasolacrimal duct, most inferior section.
b through g, Progression of sections from inferior to superior.
h, Orbital level, superior section.

Right postlacrimal sac stenosis and healthy left lacrimal system.
a, Axial CTD scan obtained at the level of the lacrimal sac. Dilation of the right lacrimal sac (white arrow) and absence of contrast medium inside the right nasolacrimal duct (arrowhead) can be appreciated. For comparison, see the healthy drainage of the contrast medium on the left side (thin arrows).
b, Axial CTD scan obtained at the level of the nasolacrimal duct.
c, Right postlacrimal sac stenosis and healthy left lacrimal system. Axial MRDt images (600/30/1) obtained after the injection of iodinate and gadopentetate contrast media at the level of the lacrimal sac. Dilation of the lacrimal sac (white arrow) and absence of contrast media below the lacrimal sac level on the right side (arrowhead) are equally depicted on MRDt images. The healthy contrast media drainage on the left side is also appreciated (thin arrows).
d, Axial MRDt images (600/30/1) obtained after the injection of iodinate and gadopentetate contrast media at the level of the nasolacrimal duct.

Bilateral dacryocystophlegmon.
a, CTD scan obtained at the level of the lacrimal sac. Dilation of the lacrimal sac, showing dense material inside, with a hyperdense foreign body inside the left one (arrowhead) is visible.
b through d, Four-in-one image with caudocranial contiguous axial T1-weighted MRDc images (600/30/1) using lacrimal canaliculus cannulation. After the injection of a diluted gadopentetate solution, only partial inflow of the contrast medium is appreciated inside the lacrimal sacs (white arrows), with intraluminal exudate being isointense to the cortex. See the small hypointense foreign body on the right lacrimal sac (arrowhead).

Right post-lacrimal sac stenosis and healthy left lacrimal system.
a, Axial MRDt image (600/30/1) obtained before fat saturation. Although no additional information is detected on the fat saturation image, higher contrast between the gadopentetate dimeglumine solution (arrowheads) and perilacrimal soft tissue is shown.
b, Axial MRDt image (600/30/1) obtained after fat saturation.
Discussion
The lacrimal system consists of two lacrimal canaliculi converging into the lacrimal sac at the level of the Maier's sinus separately or together into a common lacrimal canal with a one-way valve (Rosenmüller valve). The nasolacrimal duct originates from the lacrimal sac, extending down to the level of the inferior turbinate, where lacrimal outflow occurs through the one-way Hasner's valve, the drainage being guaranteed by orbicular muscle contraction, spreading the tears inside (Fig 5).

Schematic drawing of the lacrimal system (modified from Sobotta/Becher Atlas, USES 1976). C, lacrimal canaliculi; S, lacrimal sac; R, Rosenmüller's valve; H, Hasner's valve
Obstruction of the nasolacrimal system causing lacrimal drainage impairment and epiphora can occur above or below the lacrimal sac level. Treatment of lacrimal system stenosis includes conventional surgery (dacryocystorhinostomy). Restenosis related to scarring, however, represents one of the most common sequelae (12, 13). Recently, transluminal dilation of the lacrimal system with inflatable balloon (14–16) or application of commercially available balloon-expandable metallic stents has been performed (17).
Over the years, several imaging techniques have been used for showing the lacrimal system. These include irrigation, probing, radionuclide imaging, and, more recently, lacrimal endoscopy (18, 19). However, these techniques do not provide information concerning soft and bony tissue around the lacrimal sac and nasolacrimal duct. Radiologic investigation of the lacrimal system, using conventional or spiral CT with either dacryocystography or CTD, reliably depicts surrounding soft tissue despite the limited contrast in orbital soft-tissue imaging. Direct injection of iodinate contrast medium inside the lacrimal canaliculus, however, prevents a functional assessment of tear drainage (20).
MR imaging is considered the technique of choice for the orbit because of superior soft-tissue contrast. Nevertheless, despite excellent depiction of orbital diseases, the technique has limitations. Rubin et al (21) showed that conventional MR imaging has low sensitivity in differentiating between lacrimal sac diverticulum (communicating with the lacrimal sac) and local neoplasm. A small water-containing mucocele can also be difficult to differentiate from lacrimal sac tumors (22).
According to Goldberg et al (9), MRDc depicted the impairment of lacrimal drainage confirmed according to the surgical findings, showing sclerotic tissue before or after the lacrimal sac level as an inflammatory reaction sequela. MRDt seems to be a reliable technique in compared with MRDc; similar findings were detected in all patients except in one who was affected by dacryocystophlegmon. In that case, exudate inside the lacrimal sac prevented spontaneous drainage of the contrast-enhanced tear; however, forced injection of diluted gadodiamide solution partially filled the sac. Surgical findings indicated that a dilated lacrimal sac with sclerotic walls filled with dense purulent material with postsaccular stenosis related to sclerotic bands.
No significant difference in sensitivity was found among CTD, dacryocystography, clinical irrigation, and MRDt and MRDc. Moreover, MRD does not require delivery of ionizing radiation to the lens. Surgical findings showing sclerotic tissue inside the lacrimal system as a presumed sequela of previous inflammatory disease always confirmed the MRD data, proving the high sensitivity of the MR technique.
Regarding the safety of gadodiamide dimeglumine contrast medium, no adverse conjunctival reaction (local pain, burning sensation, or chemosis) was noted in any of our volunteers or patients. Considering that many patients affected by traumatic, neoplastic, or inflammatory diseases causing epiphora undergo presurgical MR imaging of the orbit, MRDt could easily be added to the standard protocol, showing the anatomic lacrimal system as well as any functional or drainage impairment. Moreover, MRDt permits functional assessment of lacrimal drainage and could be used instead of other ionizing techniques, such as dacryoscintigraphy. Unfortunately, the signal loss of the bony nasolacrimal canal remains the principal drawback of MR imaging, because abhealthyities of the bony nasolacrimal duct (ie, congenital bony stenosis or atresia and intracanalar bony fragments) are not easily detected.
In conclusion, MR imaging performed after the topical administration of diluted contrast material into the conjunctiva can show stenosis of the lacrimal apparatus and can be added to the standard orbital imaging protocol when lacrimal system involvement is clinically suspected.
Footnotes
1 This work was presented at: the 84th Scientific Assembly and Annual Meeting of the Radiological Society of North America, November 29, 1998; Chicago, IL.
↵2 Address reprint requests to Dr. Luigi Manfrè, Via Duca degli Abruzzi 40, 95127 Catania, Italy.
References
- Received January 13, 1999.
- Accepted after revision January 25, 2000.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}