
Article Figures & Data
Figures
- fig 1.
MR and clinical score graphs. The MR and clinical scores are presented for animals HWM-1 (A), HWM-2 (B), MP4–1 (C), and MP4–2 (D). MR scans and histologic images are presented in figures 2–5⇓⇓⇓. The dynamic nature of the MR-revealed changes is demonstrated by the changes in MR scores. These graphs show the lack of a direct correlation between clinical disease and lesion activity in the brain, particularly in the relapsing-remitting animals (MP4–1, MP4–2). More detailed information on the clinical and MR scores is presented in Tables 3–5⇓⇓
- fig 2.
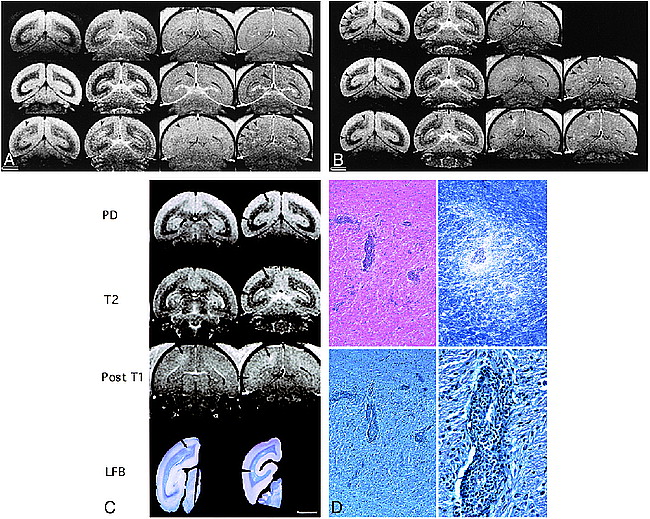
Sequential MR series and histologic representation of lesions found in MP4–1 marmoset.
A and B, Six of 15 representative sequential MR studies from weeks 0–15 after EAE induction (A, weeks 0, 2, 4; B, weeks 6, 8, 15 [from top to bottom, respectively]) show the natural history of EAE in animal MP4–1. A and B are PD, T2, postcontrast T1-weighted, and postcontrast MT T1-weighted images (left to right). B at week 6 did not have corresponding postcontrast MT T1-weighted image. This animal developed a maximal clinical score of 2 at 2–2.4 weeks, demonstrating an intermittent fixed gaze, spasticity, muscle tremors, and seizures. This animal developed transient seizures at 18 days that subsided with phenytoin therapy for a period of 30 days. At week 2, there was marked contrast enhancement of the falx cerebri and tentorium on postcontrast T1-weighted and MT images (arrowheads), which was not appreciated at baseline or on most follow-up studies. No meningeal pathologic lesions were observed after histopathologic staining. PD- (2500/20/2 [TR/TE/excitations]) and T2-weighted (2500/80/2) images showed diffuse WM lesions as early as 2.5 weeks after EAE induction (not shown) that persisted through week 4. Diffuse WM changes seen at week 4 on the PD- and T2-weighted images (arrowheads) were accompanied by more focal enhancement on the week 4 postcontrast MT image (450/13/4) (arrowheads). The same lesion areas enhancing on the 4th-week post-MT image were visible as focal lesions at week 6 on the PD-, T2-, and to a lesser extent, the postcontrast T1-weighted (450/13/4) images (arrowheads). Enhancement of the same lesion areas appears to have persisted on the 8th-week postcontrast MT image (arrowheads), and became less visible on the PD- and T2-weighted images. New lesions developed at week 15 on the PD-, T2-, and postcontrast T1-weighted and MT images (arrowheads). The contrast-enhancing lesions at weeks 4–8 appear to match some of the demyelinating lesions on the LFB-stained histologic section (fig 2C, slice 2). Enhancing lesions on the postcontrast MT image may represent the focal centers for BBB breakdown, which produced the more diffuse changes on the 4th-week PD- and T2-weighted images, and later condensed down to the focal origin of the lesions present at week 6 on the PD- and T2-weighted scans. (Scale bar equals 5 mm)
C, Two MR slices for the PD- (2500/20/2), T2- (2500/80/2), and postcontrast T1-weighted (450/13/4) sequences from the terminal 15-week MR scan are shown. Slice 2 is present in figures 2A and 2B. The LFB-stained brain mounts from the left brain are positioned below their corresponding MR slice. The brain was sectioned for histologic analysis with the superior aspect slightly posterior to the MR slice. The superior-enhancing lesion of slices 1 and 2 (arrow) on the postcontrast T1-weighted image is seen histologically only on slice 1. The histologic features of this lesion are shown in figure 2D. One demyelinated area on the LFB-stained slice 2 is also seen on the corresponding PD-, T2-, and postcontrast T1-weighted scans (arrowhead). The other areas of demyelination on the LFB-stained slice 2 appear to match previous lesion areas visible on the 4th- and 8th-week postcontrast MT, 4th-week postcontrast T1-weighted, and 6th-week PD- and T2-weighted images (fig 2A and 2B). (Scale bar equals 5 mm)
D, Histologic features of the most superior lesion in figure 2B (15th-week postcontrast T1-, MT, PD-, and T2-weighted series) and in figure 2C (postcontrast T1-weighted and LFB-stained slice 1; postcontrast T1-, PD- and T2-weighted slice 2) is shown in this figure. Top left panel is H&E-stained (magnification, 100×), top right panel LFB-stained (magnification, 100×), lower left panel is bodian silver—stained (magnification, 100×), and lower right panel is bodian silver—stained (magnification, 400×). Higher-power view of the H&E-stained sections shows that the perivascular inflammatory cell infiltrate is mostly confined to the Virchow-Robin spaces. LFB staining shows that there was minimal demyelination surrounding the inflamed vessels of the centrum semiovale. Bodian silver stains at medium and high power show that the axonal processes are intact throughout the involved regions.
- fig 3.
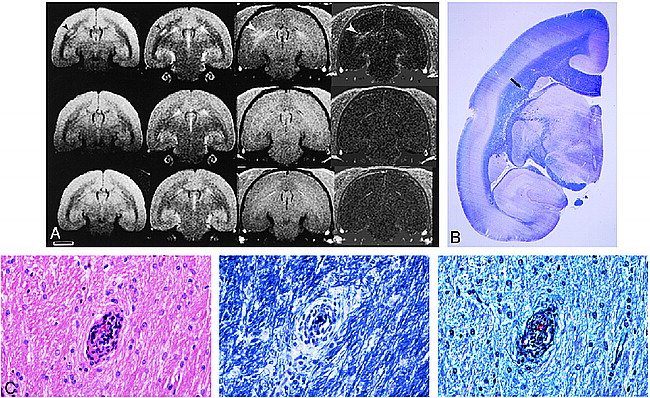
Imaging studies and histopathologic analysis of MP4–2 marmoset.
A, PD- (2500/20/2), T2- (2500/80/2), pre- and postcontrast T1-weighted images (450/13/4) (top to bottom, respectively), and the difference (post- minus precontrast T1-weighted) images are presented for marmoset MP4–2, for weeks 2.5, 4, and the 15-week terminal scan after EAE induction (left to right, respectively). The corresponding clinical scores were 2 for ataxia (week 1), 1 for weak right-hand grip (week 2), and 2 for slight ataxia (week 4). The clinical and MR scores are shown in figure 1, panel D. Little correlation existed between the MR-revealed lesions and clinical scores in this animal except for the lesion on the left side of the brain (week 2.5) and the concomitant right upper extremity weakness. A large enhancing lesion is seen in the left periventricular region, corresponding to a lesion in the same area on the T2- and PD-weighted scans at 2.5 weeks (arrowheads). The degree of enhancement can be appreciated in the difference image. By week 4 the lesion was no longer enhancing, but was visible on the PD- and T2-weighted images. By week 6 (not shown), and on the terminal scan, the lesion is no longer visible on the PD- or T2-weighted scans. The disappearance of this lesion corresponds to sparse histopathologic visibility in the anatomic region of the brain. Initially the lesion, although large in size, either did not progress to the point of demyelination or represented an area of remyelination. The only lesion present on histologic slices in the area of the large MR-revealed lesion at 2.5 weeks is minimally visible on the whole-brain mounts in figure 3B, and at higher-power magnification in figure 3C. (Scale bar equals 5 mm)
B, Luxol fast blue stained coronal section confirms that there is no demyelination. A small perivascular cuff (arrow) was the only lesion in this anatomic region located after multiple histology sections were taken through this block of brain tissue. This whole brain mount of marmoset MP4–2 corresponds to the terminal coronal scan in figure 3A and to the higher magnifications of this lesion (arrow) in figure 3C.
C, A single perivascular cuff of inflammatory cells is found at high magnification on the H&E-stained section (magnification, 400× [left]). The LFB-stained section (magnification, 400× [middle]) reveals intact myelin, and the bodian silver—stained section (magnification, 400× [right]) reveals intact axonal processes surrounding the only inflamed vessel. This lesion corresponds to the area where a large WM lesion was present at 2.5 weeks in figure 3A (arrow) and to the lesion present on the whole-brain mounts in figure 3B (arrow).
- fig 4.
MR Imaging and histologic staining of marmoset HWM-2.
A, Two MR slices are presented for the preterminal PD- (2800/22/2), T2- (2800/110/2), and post T1-weighted contrast-enhanced (400/19/3) imaging sequences. LFB-stained histologic sections are below the corresponding MR brain slice. This marmoset had a clinical grade of 3 because of a paraparesis resulting presumably from lesions affecting the spinal cord motor tracts. A demyelinated lesion on the LFB-stained slice 1 on the right side of the corpus callosum (large arrowhead) matches the centrally hypointense and peripherally hyperintense lesion on the corresponding PD-weighted image and the enhancement on the postcontrast T1-weighted scan. This lesion measured 1 mm on the MR scan and histologic features of this lesion are shown in figure 4B. A smaller demyelinating lesion present on the left side of the corpus callosum of LFB-stained slice 1 (small arrowhead) is seen as a hyperintense area on the PD-weighted image and as an enhancing lesion on the postcontrast T1-weighted image (small arrowhead). This lesion was 0.5–0.75 mm in size. The enhancing corpus callosal lesion, although already demyelinated, has a persistent inflammatory infiltrate possibly representative of a chronic active lesion. The enhancing properties on the postcontrast T1-weighted images may reflect either active cytokine release mediating a BBB breakdown or permanent BBB integrity damage. The MR and clinical scores for this animal are presented in figure 1, Panel B. (Scale bar equals 5 mm)
B, The top left panel shows an H&E-stained section (magnification, 100× [top left]) of the right corpus callosal lesion (fig 4A, slice 1 [large arrowhead]) that has a dense perivascular mononuclear inflammatory cell collection and moderate infiltration of the surrounding parenchyma. In the top right panel, the LFB-stained section (magnification, 100× [top right]) of the same field reveals demyelination throughout the involved area. In the bottom panels, the bodian silver—stained section (magnification, 100× [bottom left]; magnification, 400× [bottom right]) was used to confirm that the axonal processes were relatively spared even when there was pronounced demyelination.
- fig 5.
Imaging studies and histologic features found in marmoset HWM-1.
A, Preterminal PD- (3200/22/2) and T2-weighted (3200/110/2) MR brain images correspond to the LFB-stained whole-brain mount in the bottom row. On these slices focal lesions were present on the left side of the brain on the histopathologic and MR slices, whereas more confluent lesions were present on the right side of the brain (arrowheads). Histopathology for this animal is presented in figure 5B. The clinical and MR scores for this animal are presented in figure 1, panel A. (Scale bar equals 5 mm)
B, A histologic composite of LFB-stained lesions distributed throughout the CNS that is not confined to the LFB-stained whole-brain mount (fig 5A), is shown to demonstrate the disparity between lesion types that coexist in this model. The left panel reveals multiple perivascular inflammatory infiltrates with a well-delineated lack of LFB limited to the area of inflammation in the subcortical and deep WM. In these lesions, the inflammatory infiltrate is essentially within the Virchow-Robin space; thus, there is little, if any, true loss of myelin. The middle panel shows a more diffuse inflammatory infiltrate, again, around concentrically located vessels. In this panel the inflammatory infiltrate is minimally invasive to the parenchyma of the brain, with subsequent demyelination of the abutting axons. The right panel shows yet a more extensive inflammatory infiltrate surrounding centrally located vessels. The infiltrate extends well into the parenchyma with definite loss of myelin, giving the impression of patchy confluent lesions.





Tables
 TABLE 1:
TABLE 1:Inocula, animal designation and information, and the MR imaging schedule
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Dissociation of Experimental Allergic Encephalomyelitis Protective Effect and Allergic Side Reactions in Tolerization with Neuroantigen
- Prevention of Experimental Autoimmune Encephalomyelitis in Common Marmosets Using an Anti-IL-12p40 Monoclonal Antibody
- Effective Antigen-Specific Immunotherapy in the Marmoset Model of Multiple Sclerosis