
Abstract
SUMMARY: Stroke-like migraine attacks after radiation therapy (SMART) syndrome is a delayed complication of cranial irradiation, with subacute onset of stroke-like symptoms including seizures, visual disturbance, speech impairment, unilateral hemianopsia, facial droop, and aphasia, often associated with migraine-type headache. The diagnostic criteria were initially proposed in 2006. However, the diagnosis of SMART syndrome is challenging because clinical symptoms and imaging features of SMART syndrome are indeterminate and overlap with tumor recurrence and other neurologic diseases, which may result in inappropriate clinical management and unnecessary invasive diagnostic procedures. Recently, various imaging features and treatment recommendations for SMART syndrome have been reported. Radiologists and clinicians should be familiar with updates on clinical and imaging features of this delayed radiation complication because recognition of this entity can facilitate proper clinical work-up and management. This review provides current updates and a comprehensive overview of the clinical and imaging features of SMART syndrome.
ABBREVIATIONS:
- ALERT
- acute late-onset encephalopathy after radiation therapy
- ATP
- adenosine triphosphate
- MELAS
- mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes
- PIPG
- peri-ictal pseudoprogression
- PRES
- posterior reversible encephalopathy syndrome
- ROS
- reactive oxygen species
- SMART
- stroke-like migraine attacks after radiation therapy
Stroke-like migraine attacks after radiation therapy (SMART) syndrome is considered a delayed complication of cranial irradiation, associated with migraine-like headaches and subacute onset of stroke-like symptoms in both adult and pediatric populations previously treated for intracranial malignancies.1⇓⇓⇓⇓⇓⇓-8 SMART syndrome is often reversible, but resolution can be delayed or have permanent sequelae in some cases.5,8 A radiation dose of >50 Gy has been suggested as a threshold, but lower doses have also been reported. In 2006, Black et al6 proposed diagnostic criteria for SMART syndrome, including the following: 1) a remote history of external beam cranial irradiation; 2) prolonged, reversible signs and symptoms referable to a unilateral cortical region beginning years after cranial irradiation, including seizure, migraine with or without an aura, and stroke-like symptoms; 3) transient, diffuse, unilateral gyriform enhancement sparing the white matter within a previous radiation field; and 4) not attributed to another disorder.6 However, since the initial diagnostic criteria were proposed, further reported cases of SMART syndrome have revealed additional clinical and imaging manifestations that fail to strictly fit within these criteria despite otherwise matching the features of SMART syndrome. As well, updates regarding clinical and imaging prognostic factors and a spectrum of SMART syndrome variants including peri-ictal pseudoprogression (PIPG) and acute late-onset encephalopathy after radiation therapy (ALERT) have been proposed.9,10 In this review, we discuss clinical and radiologic updates on SMART syndrome along with a comprehensive review covering pathophysiology, clinical and radiologic features, management, and its mimics on imaging.
Epidemiology
SMART syndrome can affect both adult and pediatric populations with a male predominance.2,3 The overall incidence remains to be revealed due to its rarity. The age of onset ranges from 3.5 to 88 years of age, with a mean age of approximately 45 years and a mean time to symptom development of 14 years after brain irradiation.7 Radiation therapy is performed via whole-brain radiation therapy or focal irradiation such as stereotactic radiosurgery, intensity-modulated radiation therapy, or 3D conformal radiation therapy; a radiation dose of ≧50 Gy is often reported in SMART syndrome.5 Patients typically recover from symptoms within 1.5–2.5 months,3 but some patients experience either incomplete recovery4,5 or recurrent episodes of SMART syndrome.5,8
Recently, it has been reported that older patients are more likely to have incomplete recovery and a longer duration of symptoms of SMART syndrome and that female patients tend to have higher rates of recurrent episodes of SMART syndrome compared with male patients.5,8
Pathophysiology
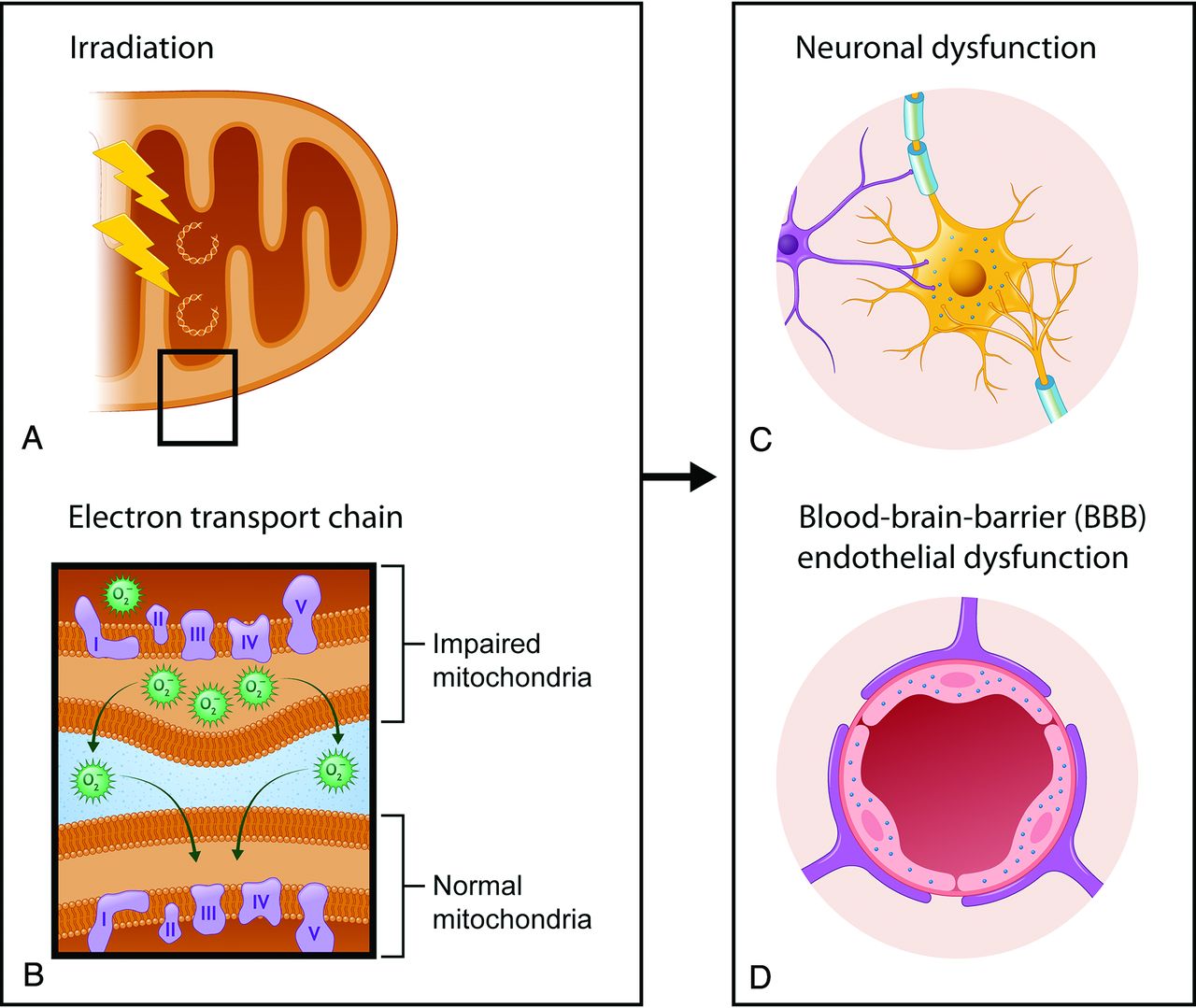
The pathophysiology of SMART syndrome has yet to be fully elucidated and is postulated to be multifactorial. Delayed brain irradiation injury involves white matter necrosis, vascular endothelial damage, demyelination, and gliosis.1 There is little histologic evidence of the above-mentioned pathophysiology of SMART syndrome.2,4 Furthermore, radiation-induced mitochondrial dysfunction has been implicated in SMART syndrome pathophysiology (Fig 1).11,12

A, Ionizing irradiation causes mitochondrial DNA damage directly or secondarily via the production of reactive oxygen species (O2) and free radicals, which result in injury to the mitochondrial DNA. B, These changes alter the function of the electron transport chain, which is composed of complex proteins (I––V) and mediates creation of adenosine triphosphate, and can result in impaired mitochondria. Also, O2 can function as a signaling molecule in intermitochondrial communication and diffuse to the nearby mitochondria, resulting in further mitochondrial dysfunction. C and D, Mitochondrial dysfunction in neurons and endothelial cells can lead to a decrease of available ATP and consequent neuronal and BBB endothelial dysfunction. Inadequate availability of ATP in both neuron and BBB endothelial cells can impair the ion homeostasis within the intracellular and extracellular compartments and lead to neuronal hyperexcitability, which can trigger subsequent cortical spreading depression.
Radiation-Induced Mitochondrial Dysfunction
Ionizing radiation therapy causes DNA damage not only in tumor cells but also in the normal brain tissues within the irradiation field directly or secondarily via the production of free radicals and reactive oxygen species (ROS) in the mitochondria.1,11 Ionizing radiation permanently impairs the mitochondria, leading to a persistent production of mitochondrial ROS.11 Mitochondrial ROS can function as signaling molecules in intermitochondrial and mitochondrial-nuclear communication and promote subsequent long-term radiation effects.11 Impairment of the mitochondria in neurons and endothelial cells can lead to altered function of the electron transport chain. Consequently, impaired mitochondria in neurons and endothelial cells leads to a decrease in available adenosine triphosphate (ATP),12 resulting in neuronal and BBB endothelial dysfunction. Inadequate availability of ATP in both neuron and BBB endothelial cells can impair the ion homeostasis within both intracellular and extracellular compartments and result in neuronal hyperexcitability.
Similarly, inadequate availability of ATP due to mitochondrial dysfunction has been also postulated in mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes (MELAS), which is related to pathogenic mitochondrial DNA gene mutations.13
Neuronal Dysfunction
Impaired neurons with radiation-induced mitochondrial dysfunction have Na, K-ATPase dysfunction due to a decrease of available ATP. Na, K-ATPase is important in maintaining extracellular ion homeostasis. When Na, K-ATPase is impaired, the K+ ion and glutamate are shifted from the intracellular space to the extracellular space. Glutamate binds to N-methyl-D-aspartate receptors and α-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid receptors, both of which are predominantly located in the dendritic spine and perisynaptic and extrasynaptic regions.14 The consequent elevation in extracellular glutamate results in a massive influx of Na+ and Ca2+ into neurons through N-methyl-D-aspartate receptors. While Na+ influx results in neuronal swelling, which is reversible, elevated intracellular Ca2+ contributes to neuronal hyperexcitability.14⇓-16
BBB Endothelial Dysfunction
BBB endothelial cells preserve ion homeostasis in the extracellular fluid, where the K+ level is strictly regulated by BBB ion transports such as Na, K-ATPase.13 Reduced functioning of BBB ion transports due to insufficient available ATP can cause an increase in K+ concentration in CSF and resulting neuronal hyperexcitability.13
Neuronal hyperexcitability is thought to trigger cortical spreading depression,17 which is a slowly propagating wave of transient regional depolarization of neurons, accompanied by suppression of all spontaneous or evoked electrical activity in that region,2,15,18 and can be observed in the acute phase of MELAS, hemiplegic migraine, and status epilepticus.
On nuclear and perfusion imaging, neuronal excitability is characterized by hypermetabolism/hyperperfusion, while subsequent spreading depression demonstrates hypometabolism/hypoperfusion. These imaging features can be used for differentiation from other etiologies such as a neoplastic process (tumor recurrence, intracranial metastasis, and leptomeningeal carcinomatosis).
Other Postulated Pathophysiology
Delayed radiation brain injury19 is postulated to induce vascular dysregulation resulting in BBB disruption and cerebral edema,20 which is similar to the proposed etiology of posterior reversible encephalopathy syndrome (PRES). Posterior circulation vessels appear to be more vulnerable to dysregulation or injury.21 However, whether there is a degree of commonality underlying the pathophysiology remains to be determined, particularly given the disparate etiologic mechanisms of vascular injury as well as the variance in distribution, because PRES usually involves the bilateral posterior circulation, while SMART syndrome usually occurs unilaterally and fails to respect vascular boundaries.
Symptoms, Clinical Work-Up, and Treatment
Symptoms.
Patients with SMART syndrome often present with migraine-type headaches (35%–72%), which have been described as being severe and unilateral and can be associated with nausea, vomiting, and light sensitivity (photophobia) with or without an aura.2,3,22 Seizure is also a common symptom of SMART syndrome (35%–83%), which can be focal or generalized and is potentially lethal, warranting rapid control by antiseizure medications.22,23 Patients with SMART syndrome can develop stroke-like neurologic deficits (33%–87%), including visuospatial deficits (complete or partial), hemisensory deficits, hemiparesis, and speech impairment.3,5,8 The incidence of subsequent infarction is reported to be 14%–18%,8,22 and the rate of recurrence of SMART syndrome is 55%–62%.5,8,22
A recent study has suggested that hemiparesis, speech impairment, and visual impairment may be likely to incompletely recover.5
Clinical Work-Up.
For the assessment of SMART syndrome, MR imaging plays a crucial role in making the diagnosis, but CSF testing and electroencephalography are also important to exclude an infectious or neoplastic process and thus are often included in the work-up.4,5 Results of the CSF analysis are usually nonspecific, without evidence of neoplastic, inflammation, or an infectious process.2,5,23 Electroencephalography, especially with a long-term video, can show electrographic activities in nonconvulsive and convulsive status epilepticus in many cases,4,5,23 allowing clinicians to prescribe antiseizure medications as appropriate.
Treatment.
Currently, there are no standard treatment guidelines for SMART syndrome due to the rarity of cases and the lack of uniformity in the approach to treatment, and treatment of symptoms is commonly performed.24
Migraines and seizures are usually controlled by antimigraine and antiseizure medications, respectively. Aspirin and verapamil are thought to help reduce the recurrence and severity of SMART syndrome episodes.2,6 Antiplatelet therapy and blood pressure drugs are conventionally used in cases in which patients with SMART syndrome are suspected of having acute infarction following an acute SMART syndrome attack. In cases in which patients with SMART syndrome have severe headache and neurologic deficits, steroids (corticosteroids) are often used mainly for reducing focal cerebral edema.3,25 However, steroid use in the acute phase has been suggested to be related to incomplete symptom recovery,5 so the risks and benefits of steroid use in SMART syndrome should be carefully considered before administration.
L-arginine, which improves endothelial function and is used in stroke-like episodes of MELAS, is reported to be a potential treatment option based on the similarity of clinical and imaging features and postulated pathophysiology.26
Imaging Features
Imaging plays a crucial role of the diagnosis of SMART syndrome, and brain MR imaging is the primary imaging technique of choice.2⇓-4 In the acute phase of SMART syndrome, the typical MR imaging features are seen as reversible, unilateral, gyriform enhancement with T2 and FLAIR hyperintense cortical swelling in a distribution not consistent with vascular territories (Fig 2).2⇓⇓-5 Findings are typically unilateral, likely reflecting the distribution of the high-dose radiation treatment field, though there are a few reports of bilateral cerebral involvement.22 Involvement of the temporal and parietal lobes is often reported, followed by the occipital and frontal lobes.4,8,22 In the delayed phase, the conventional MR imaging features as well as symptoms resolve or become mitigated. Previous reports showed that gyriform enhancement typically resolves in 14–35 days but may last up to 84 days.4 There have been many reports regarding additional imaging features of conventional neuroimaging, advanced neuroimaging, and nuclear medicine imaging. In this section, we discuss additional imaging features of SMART syndrome that are not currently included in the diagnostic criteria but are important for assessment and prognosis. We also review imaging features of variants of SMART syndrome including PIPG and ALERT.

A 51-year-old man with a history of juvenile left posterior fossa tumor treated by surgery and whole-brain irradiation 45 years ago presented with acute visual changes and seizures. He was diagnosed with SMART syndrome and treated with corticosteroids and recovered from the symptoms. A FLAIR image (A) shows cortical hyperintensity, and the postcontrast T1 image (B) shows gyriform enhancement in the right temporo-occipital region (arrows), with an incidental right temporal dural-based meningioma. There is high signal on diffusion-weighted imaging (C) without low signal on ADC (D) (facilitated diffusion) (arrows).
Conventional MR Imaging.
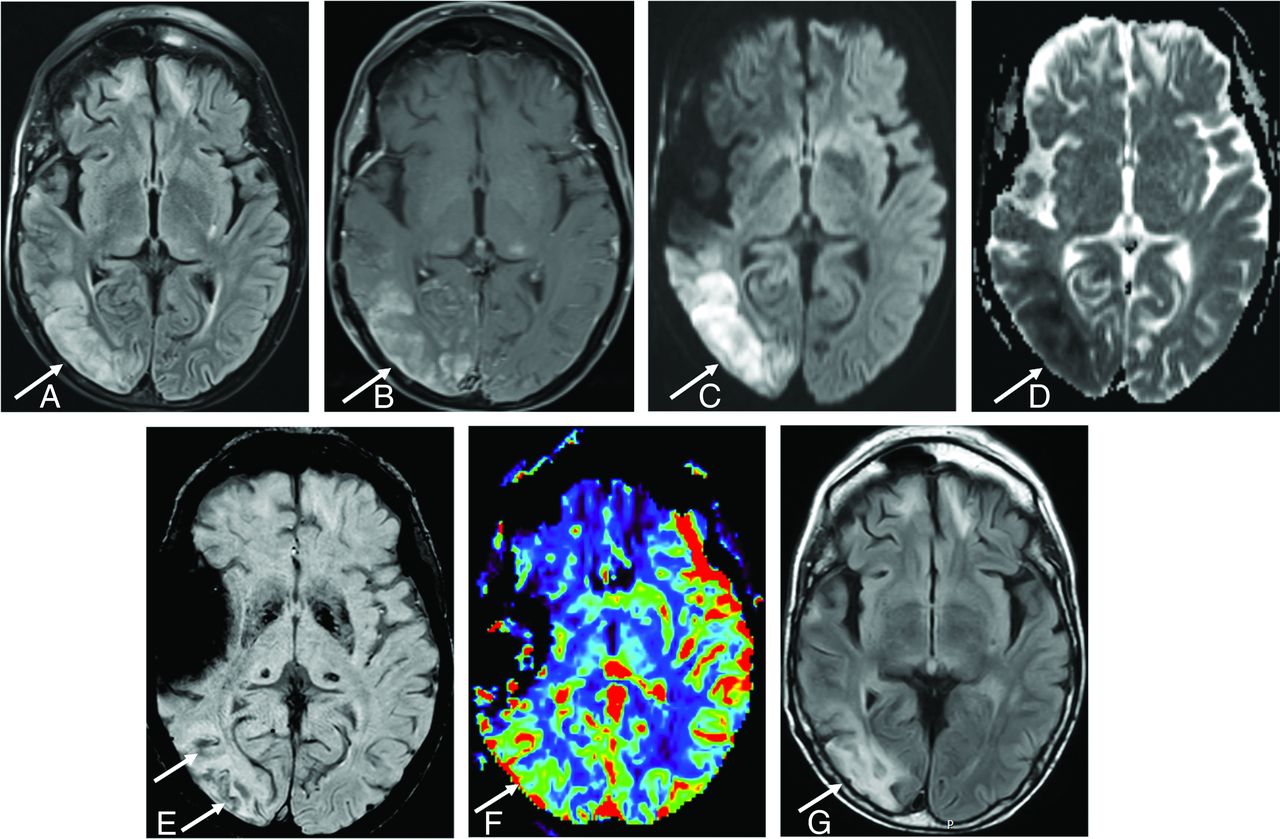
In addition to classically described MR imaging features in the diagnostic criteria, white matter involvement adjacent to the gyriform enhancement and cortical swelling are observed in some cases, likely reflecting edema in severe SMART syndrome cases (Fig 3). The white matter involvement of SMART syndrome is suspected to portend worse recovery.5

A 50-year-old man diagnosed with SMART syndrome. He had a history of pilocytic astrocytoma treated by resection and 60 Gy of radiation therapy 30 years ago and presented with left-sided hemiparesis, speech impairment, seizure, and migraine-like headache. He was diagnosed with SMART syndrome and treated by verapamil and aspirin, but residual symptoms (hemiparesis and speech impairment) remained. A, A FLAIR image shows cortical hyperintensity and involvement of subcortical white matter in the right temporo-occipital region (arrow). There is bifrontal subcortical white matter hyperintensity likely due to prior radiation injury. B, There is gyriform enhancement in the right temporo-occipital region (arrow) with restricted diffusion (C and D) (high signal on DWI and low signal on ADC) (arrow). E, SWI shows linear hypointensity along the subcortical white matter (arrow). F, Dynamic susceptibility contrast perfusion MR imaging shows an increase of CBV in the same area. G, After 3 months, FLAIR shows residual hyperintensity in the cortical and subcortical area (arrow).
DWI.
DWI detects differences in Brownian motion of water molecules, and diffusion signal abnormalities are thought to reflect alterations in the random movement of water molecules in tissues secondary to altered internal microarchitecture and can be seen in many neurologic conditions. DWI also can characterize the neuronal hypertoxicity/cortical spreading phenomenon caused by transient neuronal cell Na, K-ATPase pump impairment due to abnormal synaptic ion homeostasis, resulting in restricted diffusion.27,28 Restricted diffusion is occasionally seen in acute SMART attack regions involving the subjacent white matter. When present, restricted diffusion is suggested to be related to delayed or incomplete recovery.5,8
SWI and T2*WI.
SWI and T2*WI are sensitive to susceptibility effects of iron within hemosiderin29 and have been shown to identify microhemorrhage and radiation-induced intracranial cavernomas, which are commonly seen delayed complications of intracranial radiation therapy. SWI is more sensitive than T2*WI.30⇓-32 SWI and T2*WI show linear hypointensity in the subcortical white matter of the acute SMART attack region (Fig 3).5 There is no pathologic confirmation of this SWI white matter abnormality, but hemorrhagic transformation acutely affected by SMART syndrome is proposed.5 Also, patients with SMART syndrome with this SWI feature are suggested to experience incomplete recovery more frequently than patients without this SWI feature.5 Given that susceptibility imaging is consistently included in the routine brain protocol of many institutions, reporting of findings on SWI or T2*WI, even if negative, is important for radiologists and clinicians in terms of appropriate clinical management.
Perfusion Imaging.
CT perfusion and DSC MR imaging findings have been reported in SMART syndrome. CT perfusion evaluates iodinated contrast passing from the intravascular to extravascular space of the ROI,33 and DSC MR imaging uses the first pass of a paramagnetic contrast agent through the ROI monitored by a dynamic series of T2- or T2*-weighted images.34 Both techniques allow assessment of local perfusion from first-pass contrast bolus analysis, including CBV and CBF. In the acute phase of a SMART syndrome attack, both CBV and CBF are increased (Fig 3), reflecting increased perfusion in the acute region,35⇓-37 while in the postictal phase, CBV and CBF are suggested to decrease or become normalized.35,38 This perfusion pattern can help distinguish SMART syndrome from other etiologies such as local recurrence or carcinomatosis, which typically manifest as persistent elevated perfusion in the absence of targeted treatments, warranting sequential perfusion imaging.
MR Spectroscopy.
MR spectroscopy is a noninvasive MR imaging technique that assesses the concentration of biomolecules in an ROI. One report demonstrated a decrease in NAA and an increase in Cr and Cho peaks,39 while another article failed to find such differences.40 There appear to be insufficient data currently available to verify the role of MR spectroscopy in SMART syndrome.
Nuclear Imaging.
[18F] FDG-PET assesses regional cerebral glucose metabolism as a biomarker of neural activity and can allow localization of an epileptogenic zone in refractory epilepsy.41⇓-43 Some reports demonstrated hypermetabolism in the affected area of a SMART syndrome attack.41,42,44 Similarly, [18F] fluoroethyl- L-tyrosine amino acid (FET) PET has been used for status epilepticus45,46 and is suggested to show increased radiotracer uptake in the region of an acute SMART syndrome attack.36,45 Ictal brain perfusion SPECT using technetium Tc99m hexamethylpropyleneamine oxime was reported to show an increase of perfusion in the acute area of the SMART syndrome region,44 while the opposite pattern was reported in the interictal period,44 suggesting that endothelial dysfunction, one of the postulated pathophysiologies of SMART syndrome, is transient.
Modified Diagnostic Criteria.
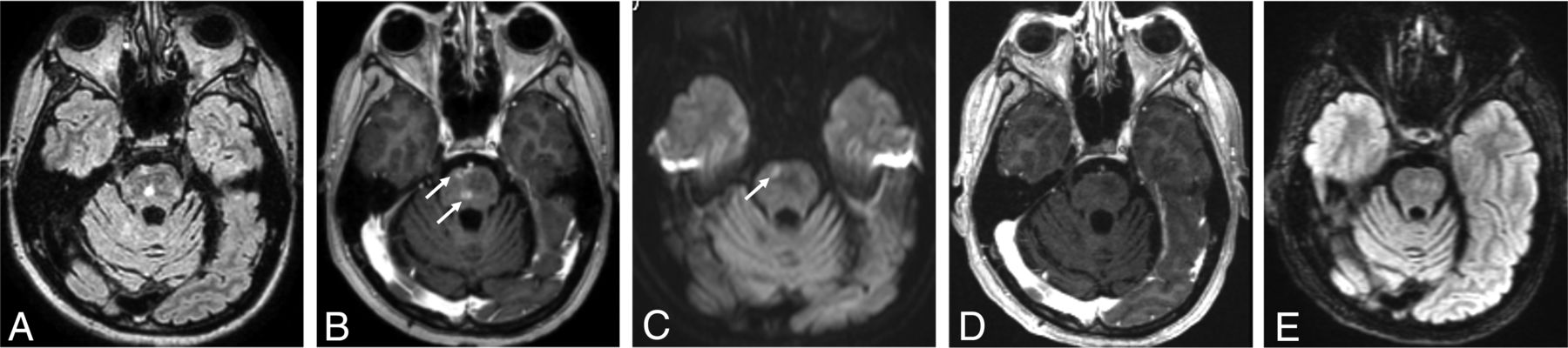
SMART syndrome is a rare late-delayed brain irradiation complication, which occurs from 1 to 37 years after radiation therapy.47 In 1995, Shuper et al48 first reported 4 pediatric cases of complicated migraine-like episodes 1–3 years after brain irradiation without detailed MR imaging features, and in 2006, Black et al6 proposed diagnostic criteria of SMART syndrome, including clinical and imaging features. However, the signs and symptoms are known to occasionally be persistent, recurrent, or followed by infarction.4,8 Furthermore, migraines are one of the common clinical features but do not always occur, despite migraines being eponymous of this entity.5 Regarding imaging features, apart from classic cortical changes, the brainstem has been suggested to be involved (Fig 4),47,49 and T2WI and FLAIR hyperintensity in the cortical and subjacent white matter may occur and last for an extended period.5 DWI, SWI, and T2*WI, which are commonly included in brain MR imaging protocols, could show alterations in acute attack regions and provide a prognostic factor for clinical recovery.5 With reference to these clinical and imaging characteristics, the diagnostic criteria proposed in 2006 could be modified as suggested in Table 1, with the above-mentioned clinical and imaging updates. The main additions to the criteria proposed in 2006 are as follows: 1) The clinical signs and symptoms may be persistent, and 2) T2WI and FLAIR hyperintensity in the cortex and subjacent white matter in the irradiated areas may occur and persist.

A 60-year-old man with brainstem SMART syndrome. He had a history of posterior fossa medulloblastoma treated with resection and 30 Gy of radiation therapy 16 years ago and presented with emotional lability and slurred speech. He completely recovered from the symptoms. A FLAIR image (A) shows hyperintensity in the central pons with peripheral patchy enhancement on the axial postcontrast T1-weighted image (arrows, B). C, DWI shows focal restricted diffusion in the corresponding area of the enhancing lesion (arrow). D and E, After 6 months, a postcontrast T1-weighted image shows resolution of enhancement with residual slight FLAIR hyperintensity.
Modified diagnostic criteria in addition to the criteria of Black et al6 for SMART syndrome
Neuroimaging of SMART Syndrome Spectrum.
Other reported delayed radiation therapy complications, which are proposed within the spectrum of SMART syndrome, include PIPG and ALERT.9,10
PIPG was postulated in 2011, with clinical features of absence of acute headache, stroke-like deficits, and MR imaging features of focal cortical or leptomeningeal enhancement overlying an ictal region without adjacent white matter involvement (Fig 5).9 Unlike SMART syndrome, PIPG is observed in all cortical regions, while SMART syndrome occurs with predominance in the temporal, parietal, and occipital lobes. A correlation between steroid introduction and clinical improvement could not be established in patients with PIPG, unlike in patients with SMART syndrome or ALERT syndrome.22

A 37-year-old man diagnosed with PIPG. He had a history of pineoblastoma treated with resection and a posterior fossa meningioma treated by resection and whole-brain irradiation 12 years before, and he presented with migraine-like headache, seizure, right-sided hemiparesis, and aphasia. He was treated with verapamil, aspirin, and valproic acid. He completely recovered from the symptoms. A FLAIR image (A) shows hyperintensity (arrow) with leptomeningeal enhancement in the left temporoparietal region on the axial (B) and sagittal (C) postcontrast T1-weighted images (arrows). Diffusion-weighted imaging (D) and ADC (E) show vasogenic edema (high signal on DWI without low signal on ADC) (arrows).
ALERT syndrome was established in 2013 and is characterized by clinical features of long-lasting impaired consciousness, seizures, and stroke-like symptoms and by MR imaging features of multifocal patchy enhancement or focal leptomeningeal enhancement associated with T2/FLAIR intensity in the corresponding area (Fig 6).10,22 Steroid efficacy was shown to be evident in patients with ALERT syndrome, with rapid symptom recovery within a few days following steroid introduction.22

A 60-year-old man with ALERT syndrome. He had a history of atypical meningioma treated with resection and radiation therapy 12 years ago and presented with impaired consciousness, left homonymous hemianopia, and left-sided weakness. He was treated with steroids, but left-sided weakness persisted. The FLAIR (A) image shows hyperintensity with patchy enhancement in the right temporoparietal region on the axial (B) and sagittal (C) postcontrast T1-weighted images (arrows).
Differential Diagnosis.
Table 2 summarizes the differential diagnosis of SMART syndrome.
Differential diagnosis of SMART syndrome
Neoplastic Process.
Given that patients with SMART syndrome typically have a history of primary or secondary CNS tumors treated with intracranial irradiation, the main differential diagnoses to consider include tumor recurrence and leptomeningeal carcinomatosis. These diseases should be ruled out because clinical management and treatment strategies are vastly different from those of SMART syndrome.
Tumor recurrence can show leptomeningeal or gyriform enhancement similar to imaging features of SMART syndrome and its spectrum on conventional MR imaging when the initial treated lesions are aggressive neoplasms or metastatic lesions,50 like leptomeningeal carcinomatosis. Therefore, confirming the original tumor and referring to the images before brain irradiation are beneficial for a differential diagnosis. In addition, transient abnormalities on perfusion and nuclear imaging between the ictal and interictal or postictal phase may help differentiate tumor recurrence from SMART syndrome and its spectrum,35,38,40,44 because imaging abnormalities of tumor recurrence and metastasis do not resolve without antioncogenic treatment. Relatively short-interval MR imaging follow-up (2–3 weeks) after therapy to reduce symptoms may also be warranted because gyriform enhancement of SMART syndrome may resolve in a short interval, while tumor recurrence and intracranial metastasis do not.4 Leptomeningeal carcinomatosis is also unlikely in the setting of resolving gyriform or leptomeningeal enhancement on follow-up MR imaging in the absence of treatment. CSF cytology, which is the criterion standard for leptomeningeal carcinomatosis with a high specificity (>95%), can be helpful for the diagnosis, though it has a low sensitivity (<50%).51
Ischemic or Vascular Process.
Subacute brain infarction can present as cortical enhancement with T2 and FLAIR hyperintensity52 and can mimic the MR imaging findings of SMART syndrome. However, subacute brain infarction typically occurs along vascular territories. Consistency with a vascular territory of subacute brain infarction can be useful to differentiate it from SMART syndrome, which often involves the temporal, parietal, and occipital lobes and does not respect vascular boundaries. If there is concern for venous ischemia, adding MR venography to a brain MR imaging protocol could be beneficial to exclude cortical vein thrombosis.53 PRES can mimic clinical features of SMART syndrome such as headache, neurologic deficits, and seizures but can typically show bilateral imaging features,54 making SMART syndrome unlikely because SMART syndrome is unilateral.
Infectious Process.
Cerebritis and meningoencephalitis can be ruled out on the basis of CSF analysis without evidence of an inflammatory or infectious process, as well as a clinical history and physical examination.
Hyperexcitable Processes.
Hemiplegic migraine or status epilepticus can also mimic clinical and imaging features of SMART syndrome.55,56 Typically, patients with hemiplegic migraine have a family history of this condition. Lack of personal or family history of hemiplegic migraine and prior intracranial irradiation make the diagnosis of SMART syndrome more likely. Status epilepticus can overlap the clinical and imaging features of SMART syndrome, making differentiation from SMART syndrome difficult.
Genetic Disease.
MELAS can show clinical features similar to those of SMART syndrome such as migraine-like headache, seizures, and stroke-like episodes. MR imaging of MELAS can also demonstrate a T2/FLAIR hyperintense cortex and subcortical white matter with leptomeningeal or cortical enhancement.13,57 The lesions of MELAS are usually multiple and asymmetric and can show an increased lactate peak with a decreased N-acetylaspartate peak on MR spectroscopy,58 while those of SMART syndrome are typically localized in a region without established MR spectroscopy findings. The diagnosis of MELAS can be confirmed by clinical tests, molecular genetic testing, muscle biopsy showing an increase of lactate and pyruvate concentrations, mitochondrial mutations, and muscle biopsy showing ragged red fibers.
CONCLUSIONS
The diagnosis, clinical assessment, and management of SMART syndrome are challenging for radiologists and clinicians due to perplexing symptoms and imaging features that can overlap with other etiologies. This review has provided an updated comprehensive overview of SMART syndrome. This rare, delayed complication of radiation therapy is still scarcely reported, and further investigation is needed to concretely establish the pathophysiology, treatment, and imaging features. Recognizing the updated clinical and imaging features of SMART syndrome can help to aid in proper clinical work-up and management.
ACKNOWLEDGMENTS
The authors thank Danielle Dobbs, graphic designer at the University of Michigan, Ann Arbor, Michigan, for creating Figure 1.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received January 31, 2023.
- Accepted after revision March 20, 2023.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.