
Abstract
BACKGROUND AND PURPOSE: Secondary prevention of ischemic stroke depends on determining the cause of the initial ischemic event, but standard investigations often fail to identify a cause or identify multiple potential causes. The purpose of this study was to characterize the impact of intracranial vessel wall MR imaging on the etiologic classification of ischemic stroke.
MATERIALS AND METHODS: This was a single-center, retrospective study of 205 consecutive patients who were referred for vessel wall MR imaging to clarify the etiology of an ischemic stroke or TIA. An expert panel classified stroke etiology before and after incorporating vessel wall MR imaging results using a modified Trial of Org 10172 in Acute Stroke Treatment system. We measured the proportion of patients with an altered etiologic classification after vessel wall MR imaging.
RESULTS: The median age was 56 years (interquartile range = 44–67 years), and 51% (106/205) of patients were men. Vessel wall MR imaging altered the etiologic classification in 55% (112/205) of patients. The proportion of patients classified as having intracranial arteriopathy not otherwise specified decreased from 31% to 4% (64/205 versus 9/205; P < .001) and the proportion classified as having intracranial atherosclerotic disease increased from 23% to 57% (48/205 versus 116/205; P < .001). Conventional work-up classification as intracranial arteriopathy not otherwise specified was an independent predictor of vessel wall MR imaging impact (OR = 8.9; 95% CI, 3.0–27.2). The time between symptom onset and vessel wall MR imaging was not a predictor of impact.
CONCLUSIONS: When vessel wall MR imaging is performed to clarify the etiology of a stroke or TIA, it frequently alters the etiologic classification. This is important because the etiologic classification is the basis for therapeutic decision-making.
ABBREVIATION:
- VW
- vessel wall
Secondary prevention of ischemic stroke depends on determining the cause of the initial stroke or TIA. However, for 25% of patients, standard investigations fail to identify a cause;1 and investigations sometimes identify multiple potential causes.
Conventional imaging of the intracranial arteries (using CTA, MRA, or conventional angiography) shows the contour of the arterial lumen, but not the arterial wall itself. This approach fails to detect nonstenotic intracranial atherosclerotic disease2⇓–4 and to differentiate disorders such as vasculitis and reversible cerebral vasoconstriction syndrome.5 It also incompletely characterizes disease activity, contributing to uncertainty about whether a particular vascular abnormality is incidental or the culprit etiology.
High-resolution vessel wall (VW) MR imaging is an adjunct to conventional vascular imaging. VW-MR imaging shows the arterial wall directly and enables the diagnosis of nonstenotic arterial disease,2⇓–4 differentiation of diseases that have a similar appearance on conventional vascular imaging,6⇓–8 and assessment of vascular disease activity.9 Studies have described the VW-MR imaging appearance of several stroke etiologies6,9,10 and measured the diagnostic accuracy of specific vessel wall findings.8,11,12 There are practice guidelines for clinical use of VW-MR imaging,9,13 and the technique has been increasingly adopted on a clinical basis.
However, there remains a broader question. When intracranial VW-MR imaging is performed to clarify the etiology of a stroke or TIA, how often and in what circumstances does this supplementary examination have an impact on the etiologic classification?
To answer this question, we studied 205 consecutive patients who had VW-MR imaging performed to clarify the etiology of a stroke or TIA. We interpreted the VW-MR imaging according to consensus guidelines and used expert-panel adjudication to characterize the impact of VW-MR imaging on the etiologic classification.
MATERIALS AND METHODS
Patients
This was a single-center, retrospective study at the University Health Network, Toronto, Ontario, Canada. We included consecutive patients referred from the hospital stroke service between 2006 and 2014 for intracranial VW-MR imaging to clarify the etiology of an ischemic stroke or TIA. We excluded patients scanned after 2014 to enable a separate analysis of long-term clinical follow-up. The institutional review board approved the study.
High-Resolution Intracranial Vessel Wall MR Imaging
VW-MR imaging on a 3T MR imaging system (Signa HDx; GE Healthcare, Milwaukee, Wisconsin) with an 8-channel receive-only head coil included time-of-flight MRA of the intracranial arteries (3D with FOV = 22 × 22 cm, acquired matrix = 512 × 512, acquired section thickness = 1 mm, section overlap = 50%, 145 slices, TR = 21 ms, TE = 2.7 ms), a T2-weighted VW-MR imaging sequence (2D fast spin-echo with FOV = 22 × 22 cm, acquired matrix = 512 × 512, section thickness = 2 mm, no interslice gap, acquired voxel = 0.4 × 0.4 × 2.0 cm, 15–25 slices, TR = 3250 ms, TE = 89 ms), and a T1-weighted VW-MR imaging sequence (single inversion recovery-prepared, 2D fast spin-echo with identical voxel dimensions, TR = 2263 ms, TI = 860 ms, TE = 13 ms) before and immediately after a 5-mL intravenous injection of gadobutrol (Gadovist; Bayer Schering Pharma, Berlin, Germany). Each VW-MR imaging sequence took 3–7 minutes, depending on the number of slices. A neuroradiologist monitored each examination to target the vessels of interest in both short- and long-axis planes, which were axial, sagittal, or coronal planes or obliques of these depending on the orientation of the vessels of interest. When conventional vascular imaging findings were normal, the VW-MR imaging target was the vessels supplying the territory of the ischemic event.
Panel Adjudication Stage 1: Conventional Work-Up
The panel included 2 neurologists with subspecialization in stroke, and 2 neuroradiologists with expertise in cerebrovascular disease. A stroke neurologist blinded to VW-MR imaging results reviewed the clinical history and physical examination notes, laboratory results, and conventional imaging reports for each patient. The neurologist categorized stroke etiology for each patient using a modification of the Trial of Org 10172 in Acute Stroke Treatment (TOAST)14 categories. We used the TOAST categories of cardioembolism, small-artery occlusion, other determined etiology, and undetermined etiology. We limited use of the TOAST category “large artery atherosclerosis” to the cervical arteries and categorized intracranial atherosclerotic disease separately. We supplemented these categories with 4 additional categories: intracranial arterial dissection, vasculitis, reversible cerebral vasoconstriction syndrome, and intracranial arteriopathy not otherwise specified. The undetermined category includes the subcategories negative evaluation, incomplete evaluation, and ≥2 causes identified. The second stroke neurologist independently categorized stroke etiology for 50 randomly selected patients in the study to assess interobserver variability.
Panel Adjudication Stage 2: Incorporating VW-MR Imaging
A neuroradiologist reviewed the VW-MR imaging for each patient and flagged any examinations that were completely nondiagnostic due to poor technical quality. The neuroradiologist categorized VW-MR imaging findings using the framework described in the Consensus Recommendations of the Vessel Wall Imaging Study Group of the American Society of Neuroradiology,9 which is summarized in Table 1. We followed the recommendations for interpretation of VW-MR imaging,9 including the need to confirm vessel wall findings in multiple planes and with multiple tissue weightings, with accurate determination of the inner and outer boundaries of the vessel wall, to confirm that vessel wall findings were indeed within the vessel wall and not thrombus within the lumen or outside the vessel. Using the same framework, the neuroradiologist also recorded whether there were VW-MR imaging findings to suggest active rather than quiescent disease. A second neuroradiologist independently categorized VW-MR imaging findings for 50 randomly selected patients in the study to assess interobserver variability.
Framework for diagnostic categorization of vessel wall MR imaging findingsa
The 2 stroke neurologists then reviewed the VW-MR imaging interpretation for each case they had previously classified, and considering the VW-MR imaging findings in the context of the entire conventional stroke work-up, they each independently either confirmed or reclassified the stroke etiology for each patient.
Statistical Analysis
Analysis software was SPSS, Version 24 (IBM, Armonk, New York). We calculated an unweighted Cohen κ statistic to measure interobserver agreement for categorization of VW-MR imaging findings, classification based on conventional work-up, and classification incorporating VW-MR imaging. We calculated the overall proportion of patients with etiologic classifications altered by intracranial VW-MR imaging and then compared the proportion of patients in each etiologic category based on conventional work-up versus conventional work-up supplemented with VW-MR imaging and used the McNemar test to identify significant differences. To identify factors from the conventional work-up (age, sex, time from symptom onset to VW-MR imaging, etiologic classification) that were associated with a change in etiologic classification after VW-MR imaging, we performed univariate logistic regression analysis with “change in diagnosis after VW-MR imaging” as the dependent variable, followed by an exploratory multivariate logistic regression.
RESULTS
Patients Characteristics and Conventional Work-Up
The study included 205 patients: 187 (91%) with stroke and 18 (9%) with TIA. Ischemic events were in the anterior circulation in 123 patients (60%), the posterior circulation in 64 patients (31%), and both in 18 patients (9%). The median age was 56 years (interquartile range = 44–67 years), and 51% of patients (106/205) were men. Table 2 describes the conventional stroke investigations. The median time from symptom-onset to VW-MR imaging was 14 days (interquartile range = 5–120 days). VW-MR imaging quality was nondiagnostic in 3/205 (1.5%) patients. All 205 patients were included in the analysis.
Conventional investigations performed to determine the etiology of TIA or stroke in 205 patients
Expert Panel Interobserver Agreement
Neuroradiologists' categorizations of VW-MR imaging findings had good15 interobserver agreement (Cohen κ = 0.75; 95% CI, 0.59–0.91). Neurologists' classifications of stroke etiology had good interobserver agreement before incorporating VW-MR imaging (Cohen κ = 0.76; 95% CI, 0.61–0.90) and very good interobserver agreement after incorporating VW-MR imaging (Cohen κ = 0.87; 95% CI, 0.74–0.99).
Impact of VW-MR Imaging on Etiologic Classificaion
The etiologic classification was altered by intracranial VW-MR imaging in 55% (112/205) of patients. The On-line Table provides details. The most common etiologic classification based on the conventional work-up was intracranial arteriopathy not otherwise specified, and 92% (59/64) of patients in this subgroup had an altered etiologic classification after VW-MR imaging.
VW-MR imaging led to a decrease in the proportion of patients classified as having “intracranial arteriopathy not otherwise specified” from 31% to 4% (64/205 versus 9/205; P < .001) and an increase in the proportion of patients classified as having “intracranial atherosclerotic disease” from 23% to 57% (48/205 versus 116/205; P < .001). VW-MR imaging led to a decrease in the proportion classified as “etiology undetermined due to 2 or more potential causes” from 4% to 1% (9/205 versus 2/205; P = .016), and a decrease in the proportion classified as having “small-vessel occlusion” from 3% to 0% (7/205 versus 1/205; P = .031). The Figure shows a representative case.

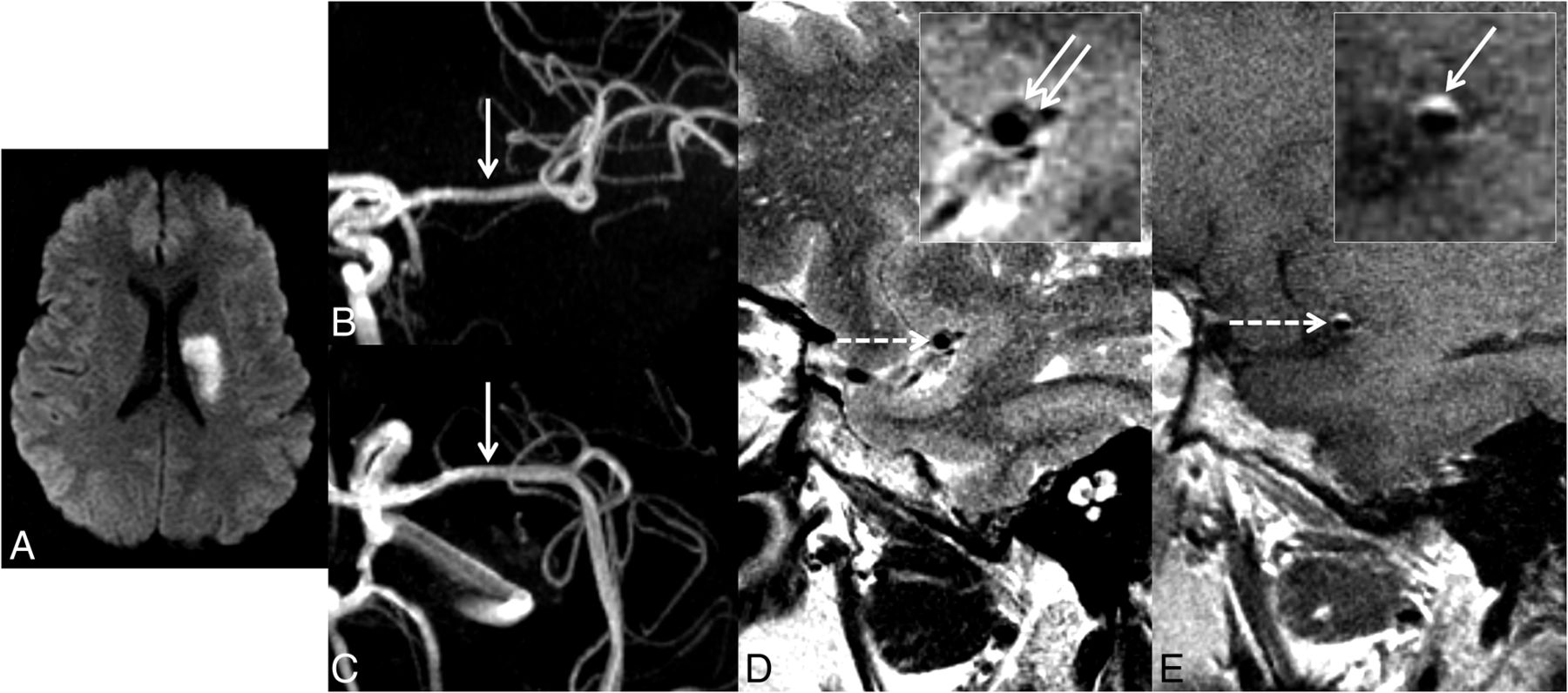
Representative case with conventional stroke work-up with negative findings and altered etiologic classification after VW-MR imaging. Diffusion-weighted MR imaging (A) shows an acute infarct in the left MCA lenticulostriate territory. MRA anterior-posterior (B) and craniocaudal (C) projections show no/minimal narrowing of the left MCA (arrows). Sagittal T2-weighted VW-MR imaging (D) shows a cross-section through the left MCA (dashed arrow), and a magnified view (inset box) shows focal, eccentric, thickening of the superior-posterior wall of the left MCA (solid arrows). Sagittal contrast-enhanced T1-weighted VW-MR imaging (E) shows the same vessel (dashed arrow) with corresponding wall enhancement (solid arrow). The VW-MR imaging appearance is consistent with atherosclerotic plaque, and the enhancement is a finding more common in recently symptomatic plaque. Adapted with permission from Schaafsma et al.23
Predictors of Impact
In the multivariate analysis, the 1 factor that independently predicted a change in etiologic classification after VW-MR imaging was the conventional work-up classification of intracranial arteriopathy not otherwise specified (odds ratio = 8.9; 95% CI, 3.0–27.2). Factors that independently predicted no change were the conventional work-up classification of intracranial atherosclerotic disease (OR = 0.2; 95% CI, 0.1–0.4) or cardioembolism (OR = 0.1; 95% CI, 0–0.6). Table 3 provides details.
Factors associated with revised etiologic classification when conventional stroke work-up is supplemented with VW-MR imaging
DISCUSSION
The objective of our study was not to measure the diagnostic accuracy of intracranial VW-MR imaging but to apply the current guidelines for interpretation of VW-MR imaging and measure the impact of the technique on the etiologic classification in patients with recent ischemic stroke or TIA. We found that VW-MR imaging substantially increased the proportion of strokes attributed to intracranial atherosclerotic disease. VW-MR imaging did not change the overall proportion of strokes attributed to vasculitis, but it altered which particular strokes were attributed to vasculitis. VW-MR imaging was most likely to have a diagnostic impact for patients who already had categorization as having intracranial arteriopathy based on the conventional work-up. The length of time between symptom onset and VW-MR imaging was not a predictor of impact.
We were not surprised to find strokes newly attributed to intracranial atherosclerotic disease after VW-MR imaging. VW-MR imaging can detect plaque that is occult on conventional vascular imaging, and previous studies have shown plaque on VW-MR imaging in patients with cryptogenic lacunar infarction.3,4 This is important because symptomatic intracranial plaque portends a high risk of recurrent stroke and can prompt specific treatment such as dual antiplatelet drug therapy and optimization of blood pressure and lipid profile.16 However, the presence of intracranial atherosclerotic plaque does not alone imply that intracranial plaque is the culprit, and we will return to this point later in this discussion.
VW-MR imaging did not alter the proportion of strokes attributed to vasculitis, but it altered which particular strokes were attributed to vasculitis. Among patients categorized as having vasculitis based on conventional work-up, only two-thirds were categorized as having vasculitis after VW-MR imaging. Most of these patients had a vessel wall lesion with typical characteristics of atherosclerotic plaque. Conversely, among patients categorized as having vasculitis after VW-MR imaging, only one-third had been categorized as having vasculitis based on conventional work-up alone. Most of these patients had been categorized as having intracranial arteriopathy not otherwise specified rather than a specific condition by conventional work-up alone.
The definitive test for central nervous system vasculitis is brain biopsy. A limitation of biopsy is undersampling due to spatially heterogeneous disease or the need to avoid eloquent regions.5 Also, vasculitis may predominate in the larger intracranial arteries rather than the smaller vessels that are usually biopsied.17 VW-MR imaging is a noninvasive means to assess arterial wall inflammation, and this can help discriminate between vasculitis and mimics such as reversible cerebral vasoconstriction syndrome and atherosclerotic disease.7,8,12,18
We had few patients categorized as having etiology undetermined due to ≥2 potential causes, but VW-MR imaging significantly decreased the proportion of patients in this category. VW-MR imaging can be useful in this context because it provides information on disease activity.
The factor that independently predicted a change in the etiologic classification after VW-MR imaging was the conventional work-up classification as intracranial arteriopathy not otherwise specified. This was not unexpected, but the high odds ratio (OR = 8.9; 95% CI, 3.0–27.2) emphasizes that a pre-existing abnormality on conventional imaging increases the likelihood of impact from VW-MR imaging. We found that the time between symptom onset and VW-MR imaging was not a predictor of impact from VW-MR imaging in our study, which had a median delay of 2 weeks, but it may be best to perform VW-MR imaging within weeks rather than months of symptom onset because findings such as atherosclerotic plaque enhancement may wane after several weeks to months.19,20
There is no single, ideal reference standard for determining stroke etiology. Therefore, we modelled our study design on clinical practice and used an expert panel to categorize stroke etiology. The stroke neurologists integrated multiple clinical, laboratory, and imaging factors to decide on the categorization. For example, 1 patient had both a patent foramen ovale and an intracranial atherosclerotic plaque, so the neurologists had to decide which one was the likely etiology. For this case, the plaque was designated as the likely etiology because contrast echocardiography had characterized the patent foramen ovale as “low-risk,” intracranial plaque was only evident in the artery supplying the territory of the stroke, and the plaque was intensely enhancing (a feature that the VW-MR imaging framework views as a feature of recently symptomatic plaque).19,20 We believe this use of an expert panel, with independent assessments and measurement of in-terobserver agreement, is a re-asonable approach to measure the diagnostic impact of VW-MR imaging. However, it is important to recognize the potential for confirmation bias: interpreting the additional information provided by VW-MR imaging as overly definitive.
This study used T1-, T2-, and contrast-enhanced T1-weighted VW-MR imaging sequences, and the interpreting neuroradiologists used the multiple tissue-weighting and multiple imaging planes to confirm the vessel wall findings as recommended.9 Some centers use only T1-weighted VW-MR imaging sequences. Our local preference has been to routinely include a T2-weighted sequence as well because it can help confirm that a finding is within the vessel wall rather than within the lumen and can contribute to the characterization of vessel wall lesions (eg, identification of hyperintensity within the fibrous cap of atherosclerotic plaque).
We evaluated patients who were referred for VW-MR imaging to clarify the cause of a stroke or TIA. We believe this is a clinically relevant patient group because it likely approximates the types of patients who will have intracranial VW-MR imaging at other centers. However, relying on the referral patterns of multiple stroke neurologists who have different thresholds for requesting intracranial VW-MR imaging does introduce a selection bias, and the proportion of patients with altered etiologic classifications after VW-MR imaging may differ at other institutions.
We used a modified TOAST14 classification system because this system is well-known and reflects the kind of etiologic classification often used in clinical practice, but there are other systems we could have used,21,22 and these may have led to different proportions of patients with a revised etiologic classification. Also, we did not attempt to stratify the level of diagnostic confidence within each particular etiologic category, but changes in the level of confidence within categories may affect therapeutic decision-making, too.
All patients had electrocardiography and many (74%) had echocardiography, but fewer (29%) had Holter rhythm monitoring for >24 hours. This scenario likely reflects the high proportion of patients who had intracranial arteriopathy not otherwise specified or a working diagnosis based on conventional work-up rather than completely cryptogenic stroke.
CONCLUSIONS
We found that when VW-MR imaging is performed to clarify the etiology of a stroke or TIA, it can have a substantial impact on etiologic classification. Because this impact is substantial, intracranial VW-MR imaging has the potential to improve therapeutic decision-making for many patients. The contrary is also true: Improper application of the interpretive framework or limitations of the framework itself have the potential to misinform therapeutic decision-making for many patients. Physicians who are performing and interpreting VW-MR imaging should familiarize themselves with technical recommendations and interpretive pitfalls for VW-MR imaging and recognize that there remain gaps in knowledge and that research is ongoing.
ACKNOWLEDGMENTS
We appreciate the dedication and skill of the Toronto Western Hospital MR imaging technologists involved in this work, especially Nicole Bennett, Holly Chun, Colleen Grace, Mary Hatchard, Olga Ioffina, Nisha James, Mahnaz Miraftabi, Asma Naheed, Jessica Pinto, Keith Ta, and Danfeng Zhao.
Footnotes
This study was supported by the Ontario Academic Health Science Centres Innovation Fund.
Disclosures: Daniel M. Mandell—RELATED: Grant: Ontario Academic Health Science Centers Innovation Fund.* *Money paid to the Institution.
References
- Received May 9, 2019.
- Accepted after revision July 24, 2019.
- © 2019 by American Journal of Neuroradiology





{kind=link}