
Abstract
BACKGROUND AND PURPOSE: Highly predictive markers of drug treatment outcomes of tuberous sclerosis complex–related epilepsy are a key unmet clinical need. The objective of this study was to identify meaningful clinical and radiomic predictors of outcomes of epilepsy drug treatment in patients with tuberous sclerosis complex.
MATERIALS AND METHODS: A total of 105 children with tuberous sclerosis complex–related epilepsy were enrolled in this retrospective study. The pretreatment baseline predictors that were used to predict drug treatment outcomes included patient demographic and clinical information, gene data, electroencephalogram data, and radiomic features that were extracted from pretreatment MR imaging scans. The Spearman correlation coefficient and least absolute shrinkage and selection operator were calculated to select the most relevant features for the drug treatment outcome to build a comprehensive model with radiomic and clinical features for clinical application.
RESULTS: Four MR imaging–based radiomic features and 5 key clinical features were selected to predict the drug treatment outcome. Good discriminative performances were achieved in testing cohorts (area under the curve = 0.85, accuracy = 80.0%, sensitivity = 0.75, and specificity = 0.83) for the epilepsy drug treatment outcome. The model of radiomic and clinical features resulted in favorable calibration curves in all cohorts.
CONCLUSIONS: Our results suggested that the radiomic and clinical features model may predict the epilepsy drug treatment outcome. Age of onset, infantile spasms, antiseizure medication numbers, epileptiform discharge in left parieto-occipital area of electroencephalography, and gene mutation type are the key clinical factors to predict the epilepsy drug treatment outcome. The texture and first-order statistic features are the most valuable radiomic features for predicting drug treatment outcomes.
ABBREVIATIONS:
- ASM
- antiseizure medication
- AUC
- area under the receiver operating curve
- EEG
- electroencephalography
- GLCM
- gray-level co-occurrence matrix
- GLDM
- gray-level dependence matrix
- GLRLM
- gray-level run-length matrix
- GLSZM
- gray-level size zone matrix
- LASSO
- least absolute shrinkage and selection operator
- TSC
- tuberous sclerosis complex
Tuberous sclerosis complex (TSC) is a rare autosomal dominant disorder caused by loss-of-function mutations of the TSC1 or TSC2 genes, which can affect multiple organ systems1 and is frequently associated with tumors of the brain, skin, heart, lungs and kidneys, seizures, and TSC-associated neuropsychiatric disorders, including autism spectrum disorder and cognitive disability.2 Epilepsy is the most common and clinically challenging symptom of TSC, affecting approximately 85% of patients,3,4 of which nearly two-thirds have the first seizure in the first year of life.5,6
The goal of treatment in TSC is to prevent or control seizures as soon as possible after TSC diagnosis, which will improve cognitive neurodevelopment and enhance the quality of life.3 The classic treatment for epilepsy is antiseizure medication (ASM).7 However, >50% of patients with TSC will develop drug-resistant epilepsy,8,9 and diagnosing it may take a long time.10 Therefore, there is an urgent need to investigate the predictive biomarkers for the effectiveness of ASM treatment for patients with epilepsy.
Nervous system manifestations can be observed in almost all cases of TSC, and MR imaging is a technique used routinely to diagnose TSC.11 Cortical tubers are major TSC-related brain manifestations, which show abnormal high or low signals in FLAIR sequences.12 In addition, FLAIR imaging is widely used to study the epileptogenic zone13 and epilepsy mechanism of TSC.14 Jesmanas et al9 reported that MR imaging–defined tuber types were found to be associated with early seizure onset in TSC. In addition, lesion location and type of information features in MR imaging have been shown to be associated with the outcomes of epilepsy drug treatment.10 However, the features of MR imaging were typically extracted manually, and the description of these features was usually qualitative, subjective, and nonspecific.
Radiomics is an emerging research branch in the field of medical imaging, which aims to extract mineable high-dimensional data from clinical images.15,16 Radiomics capture tissue and lesion characteristics, such as heterogeneity, texture, and shape and can be used alone or in combination with demographic, histologic, genomic, or proteomic data to solve clinical problems.17 Radiomic analyses have been successfully applied to predict the type of tumor-related epilepsy or epilepsy presentation18⇓⇓⇓-22 and treatment outcomes for cancer.23⇓⇓⇓-27 Thus, a noninvasive biomarker based on radiomic analyses that can predict the drug treatment outcome in patients with TSC would be valuable.
In this study, we used FLAIR scans to extract radiomic features including shape, first-order statistics, and textural features that are associated with the drug treatment outcome in patients with TSC. Moreover, we constructed a machine learning model to investigate how accurately we can predict the drug treatment outcome in patients with TSC using radiomic and clinical information.
MATERIALS AND METHODS
Patients
A total of 105 patients with TSC at Shenzhen Children’s Hospital between January 2013 and September 2018 were consecutively enrolled in this retrospective study, and informed consent was obtained from all patients before the study. The protocols were approved by the Ethics Committee of Shenzhen Institutes of Advanced Technology, Chinese Academy of Sciences. We included patients who met the following criteria: 1) They had undergone FLAIR MR imaging before ASM treatment, 2) electroencephalography (EEG) was recorded on admission or as an outpatient, 3) they had ASM treatment for at least 1 year, and 4) the ages at MR imaging were younger than 6 months.
Drug treatment outcome was defined according to the Gül Mert et al6 and was recorded as controlled or uncontrolled. Patients were considered as controlled if they had not had clinical seizures for at least 1 year. Uncontrolled patients had at least 1 seizure in the past year. Data were randomly split into a training data set (n = 75) and an independent test data set (n = 30). We used stratified random sampling to ensure the same class ratios for every set. There was no patient overlap between the training and test sets. The training data set was used to derive clinical and radiomic predictors of epilepsy; then, the classification performance of these predictors was internally validated on the test data set.
Data of 59 routine clinical variables were collected, including patient information, such as sex, age, typical symptoms of TSC, and examination results, as well as TSC1 and TSC2 gene test results and EEG features and so forth. This study further used the clinical and MR imaging data of all enrolled cases. The flow chart of the study is illustrated in Fig 1.

The flowchart of the current study. Patient information, including sex, age, the existence of typical symptoms of TSC, and some examination results. TSC1 and TSC2 were gene test results.
Image Acquisition
All MR imaging examinations were performed using a Magnetom Trio 3T scanner (Siemens) with an 8-channel receive-only head coil acquisition. The FLAIR parameters were as follows: TR = 9000 ms, TE = 132 ms, TI = 2600 ms, flip angle = 150°, FOV = 230 × 194 mm2, voxel size = 0.7 × 0.7 × 6.0 mm3, and matrix = 320 × 224. The MR imaging data were stored in DICOM format.
Image Processing and Segmentation
In neuroimaging studies, the ROIs are located in the brain tissue. Therefore, we removed the nonbrain tissue in MR imaging using a deep learning model.28
ROIs of the cortical tubers and migration lines were manually drawn by 2 neuroradiologists with >15 years of experience who were blinded to clinical data using open-source software (ITK-SNAP, Version 3.8.0; http://www.itksnap.org). ROIs were merged when the difference between the individual ROIs determined by the 2 neuroradiologists was <5%. When there was a >5% difference between these 2 ROIs, the ROI used was determined by a senior neuroradiologist. ROIs of the cortical tubers and migration lines were defined as areas of the MR images that exhibited abnormal hyperintense or hypointense signals. Figure 2 shows some cases of FLAIR images with and without lesions and segmentation in children with TSC. Figure 2A shows the FLAIR images of some children with TSC with lesions, and Fig 2B is the segmentation of Fig 2A. Figure 2C shows the FLAIR images of some children with TSC without lesions.

Some cases of FLAIR images with and without lesions and segmentation in children with TSC. A, The FLAIR images of some children with TSC with lesions. B, The segmentation of A. C, The FLAIR image of some children with TSC without lesions. The red color represents the segmentation of lesions.
Radiomic Feature Extraction
Due to differences in equipment parameters such as layer thickness and pixel pitch of MR images, all images were resampled to 1 × 1 × 1 mm³. A publicly available Python package, pyradiomics 3.0.1 (https://pypi.org/project/pyradiomics/), was used to extract radiomic features.29 A total of 1132 features consisting of gray-level co-occurrence matrix (GLCM), gray-level run-length matrix (GLRLM), gray-level size zone matrix (GLSZM), gray-level dependence matrix (GLDM), first-order, and shape features were extracted from ROIs on FLAIR.
First-order features described the distribution of voxel intensity within the ROI 3D matrix and the overall information about the cortical tubers. The shape features reflected the volume, surface area, and shape of the cortical tubers. GLCM, GLRLM, GLSZM, and GLDM were collectively referred to as texture features. The detailed information and formulas for the detection of the 1132 radiomic features are described in https://pyradiomics.readthedocs.io/en/latest/.
Feature Selection
The 1132 radiomic features and 59 routine clinical variables were normalized with z score normalization before feature selection. First, a bivariate analysis was conducted to screen the radiomic and clinical features. We calculated the P values of the Spearman correlation coefficient between each feature and the treatment outcome and identified the features with P values < .05. Least absolute shrinkage and selection operator (LASSO) was widely used to compress the coefficients of features and select features to prevent overfitting, so we used a LASSO algorithm to select the key radiomic and clinical features.
Development and Evaluation of an Individualized Prediction Model
On the basis of a cohort of all patients, we used 11 machine learning classifiers, such as support vector machines, random forest, logistic regression, AdaBoost (https://www.machinelearningplus.com/machine-learning/introduction-to-adaboost), gradient boosting, and decision tree to build models to predict treatment outcome with clinical information and radiomic features.
Each classifier was trained on the training set using a 10-fold cross-validation procedure and the training process needed to determine the optimal hyperparameters of the classifiers, which were determined by grid search. We selected the best classifier by comparing the performance of classifiers on the validation set. The classifier that achieved the highest area under the receiver operating curve (AUC) score was selected as a candidate solution.
Once trained, the best model was evaluated on the test set. The classification performance of the model was assessed by the receiver operating characteristic curves and AUCs in each cohort. Calibration curves were also plotted to assess the calibration of the radiomic and clinical features.30
Statistical Analysis
In this study, we use frequencies and percentages for categoric variables and median and range for continuous variables. The differences between groups were assessed by an independent samples t test, and P < .05 was defined as significant. Model training, validation, and testing were implemented with Python (Version 3.8.0).
RESULTS
Demographic and Clinical Data
The main clinical and pathologic characteristics of all 105 patients are listed in the Online Supplemental Data. Of the 105 enrolled patients, 43 (40.9%) were controlled and 62 (59.1%) were uncontrolled by drug treatment. Age of onset, infantile spasms, gene mutation type, ASM numbers, and epileptiform discharge in the left parieto-occipital area of the EEG were significantly different between the controlled and uncontrolled patients (P < .05).
Performance of the Radiomic Signature
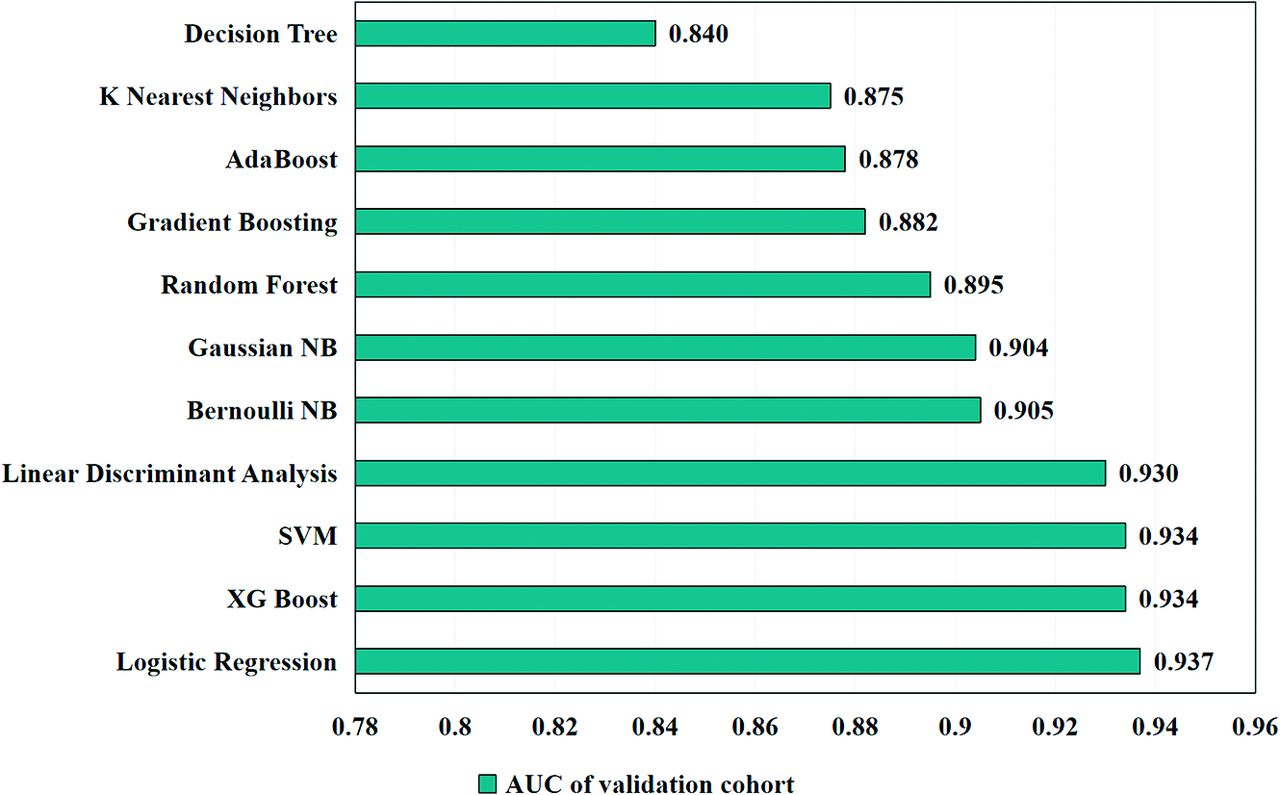
Four key radiomic features and 5 clinical features were selected using the Spearman correlation analysis and LASSO regression (Table 1), and the distribution of each radiomic feature in the controlled and uncontrolled groups is shown in Fig 3A–D. According to the AUC of the validation set that was used to select the best hyperparameters and model, the best classification model is logistic regression (Fig 4). The predictive ability of the model with radiomic and clinical features was shown by the receiver operating characteristic curve (Fig 5A), achieving the best performance of AUC = 0.96, classification accuracy = 90.7%, sensitivity = 0.97, and specificity = 0.86 in the training cohort; AUC = 0.94, classification accuracy = 88.0%, sensitivity = 0.94, and specificity = 0.84 in the validation cohort; and AUC = 0.854, classification accuracy = 80.0%, sensitivity = 0.75, and specificity = 0.83 in the test cohort, respectively. Table 2 shows the test set results on logistic regression models with input of clinical features alone and with input of radiomic and clinical features. Figure 6 shows a performance comparison of clinical features alone and radiomic and clinical features on a logistic regression model in the testing cohorts. The results of the test set with the logistic regression model are shown in Table 2. The model of radiomic and clinical features demonstrated favorable calibration in the training, validation, and testing cohorts (Fig 5B). Figure 5C–E shows the waterfall plots of radiomics and the clinical model to differentiate controlled from uncontrolled patients in the training, validation, and testing cohorts.
The radiomic and clinical features selected by LASSO regression

Boxplot of the 4 selected values of radiomic features in controlled and uncontrolled groups. The small blue and red circles represent the value of each radiomic feature in the controlled and uncontrolled groups. The middle line of the boxplot is the median of the radiomic feature, representing the average level of the radiomic feature. The upper and lower bounds of the boxplot are the upper and lower quartiles of the radiomic feature data, respectively. P values are the results of the Spearman correlation test.

The AUC scores of 11 machine learning models in the validation cohort. According to the AUC of the validation set that was used to select the best hyperparameters and model, the best classification model of radiomic and clinical features is logistic regression. NB indicates Naive Bayes; SVM, support vector machine; XG, eXtreme Gradient.

Receiver operating characteristic curve (A), calibration curve (B), and waterfall plots (C–E) of the radiomic and clinical features model in training, cross-validation, and testing cohorts.
The results of the logistic regression model in testing cohorts

The performance comparison of clinical features alone and radiomic and clinical features on a logistic regression model in testing cohorts. ACC indicates accuracy; SEN, Sensitivity; SPE, specificity.
DISCUSSION
With the increasing use of drug treatments in epilepsy, a better understanding of patient response to the treatment could help identify the optimal treatment strategy for individual patients.10 Radiomic approaches, when combined with clinical data, could improve treatment selection. In this study, a prediction model of drug treatment outcome based on radiomic data from MR imaging and clinical data was developed. The results demonstrate that the MR imaging–based radiomic and clinical models could successfully predict the outcome of epilepsy drug treatment among children with TSC.
Reliable prediction of epilepsy drug treatment outcome allows the development of a more targeted treatment, and those patients proved to be drug-resistant should be considered for surgical procedures or other treatment options to increase the curative ratio and reduce mortality.31,32 However, determining the epilepsy drug treatment outcome on the basis of its clinical and treatment presentation imposes an apparent lag. Thus, there is a need for a clinical model capable of predicting epilepsy drug treatment outcome before treatment initiation. In this study, a new model with radiomic and clinical features was developed at baseline to predict the epilepsy drug treatment outcome for patients with TSC, which will provide clinicians with a reliable and noninvasive tool to better select patients for epilepsy drug treatment.
With the rapid development of machine learning and image-processing techniques, a number of studies have developed radiomics-based predictive models for various clinical characteristics, including pathologic grade33,34 and treatment and survival outcomes.35,36 The rapid increase of the radiomic application is driven by enriched quantitative image features that clinicians can extract from medical images with high efficiency to guide clinical decision-making.37 Moreover, some researchers have successfully applied radiomic analysis to predict tumor-related epilepsy by combining various quantitative MR imaging features.18,20⇓-22 Their works mainly focused on tumor-related epilepsy. However, epilepsy caused by TSC is different. It has distinct clinical manifestations and presentations on MR imaging.10
To our knowledge, this is the first study to show that radiomics can be used to predict the outcome of epilepsy drug treatment in patients with TSC. Therefore, we tried to demonstrate the associations of these radiomics-based MR imaging features with TSC-related epilepsy drug treatment outcome, and we have achieved a relatively high discrimination accuracy and AUC in all cohorts, which suggest that the radiomic model developed in this study was effective in predicting the outcome of epilepsy drug treatment.
In our study, we selected 4 radiomic features to predict drug treatment outcomes, including log-sigma-2–0-mm-3D_gldm_SmallDependenceHighGrayLevelEmphasis (L_gldm_S), wavelet-LLH_glcm_Idmn (W_glcm_I), wavelet-LLL_firstorder_10Percentile (W_firstorder_10), and wavelet-LLL_firstorder_Mean(W_firstorder_M). L_gldm_S and W_glcm_I are texture features that reflect the homogeneity of the tubers. W_firstorder_10 and W_firstorder_M are first-order statistical features that reflect the distribution of signal intensities within the tuber region. Our results imply that the texture features and first-order statistical features are valuable for predicting drug treatment outcomes. Zhao et al38 had reported that the type II lesions (the uneven thickening of the cortex on T2-weighted and FLAIR) were statistically significant between the uncontrolled and controlled groups, similar to findings in our research. MR imaging lesion type features are related to outcomes of epilepsy drug treatment in TSC,10,12 which can indirectly support our present results because the types of lesions are generally classified clinically according to texture structure and the signal intensity of the lesions.
Additionally, our model incorporated both radiomic features and clinical characteristics that are helpful for prediction, such as the age of onset, infantile spasms, ASM numbers, epileptiform discharge in left parieto-occipital area of the EEG, and gene mutation type, making our model more comprehensive and reliable for clinical application. Our study found that about 59.1% of patients with TSC were in the uncontrolled group. It was reported that the drug resistance ratios of TSC-related epilepsy were 59.6%,38 60%,5and 62%,39 which were similar to those in our study. In addition, about 30 (48.4%) patients in the uncontrolled group had experienced infantile spasms, and 4 (9.3%) patients in the controlled group had experienced infantile spasms. Previous studies have shown similar results: TSC patients with infantile spasms are more likely to develop drug resistant epilepsy.4,40 In our study, the mean age of seizure onset was 10.34 months in the uncontrolled group and 31.17 months in the controlled group. Patients with TSC epilepsy before 1 year of age are more likely to develop resistance than those with onset after 1 year of age,40 consistent with our results. Compared with TSC1 pathogenic mutations, TSC2 mutations have a more severe clinical phenotype, and the conditions of these patients are usually more difficult to control,39,41 consistent with our findings that the proportion of TSC2 gene mutations was higher in the uncontrolled group.
Our results showed that the severity of EEG discharge in the left parieto-occipital area was correlated with the epilepsy drug treatment outcome, and the EEG discharge in the uncontrolled group was more serious. Previous reports also showed similar results. Some patients with TSC with severe EEG discharges have multifocal EEG discharges related to bilateral asymmetric spike-and-wave complexes. The onset is partial seizures or convulsive seizures, which later develop into drug-resistant epilepsy.39,40 In a study of 83 patients with TSC, ASM numbers have been reported as an important risk factor for development of refractory epilepsy in patients with TSC.6 In our study, the history of using >3 ASMs is the risk factor that will lead to occurrence of drug-resistant epilepsy.
LASSO is a widely accepted algorithm in feature selection. The 1132 radiomics features extracted in this study may cause overfitting when constructing the model. Therefore, feature dimension reduction and selection were performed to screen the key features that are most closely related to the epilepsy drug treatment outcome using bivariate analysis and the LASSO algorithm. With features associated with epilepsy drug treatment outcome, we used 11 classic machine learning models for classification and selected the best model on the basis of AUC of cross-validation. Finally, we evaluated the performance of the selected model on the independent test set consisting of unseen data.
Although this study is novel and conducted with advanced methodology, there are several limitations. First, it is a single-center cohort study, and a multicenter cohort study should be further considered to verify the findings of this study. Second, the data set is relatively small because TSC is a rare disease. However, we will collect more data from additional patients with TSC and will use advanced algorithms such as deep learning to make more precise predictions in the future. Finally, our study used only the MR imaging technique, which contains limited information. We will explore the multimodal data such as CT and PET to construct a more comprehensive radiomic model in future exploration.
CONCLUSIONS
Our study suggests that radiomics could be a noninvasive, efficient, and reliable way to predict patient outcome to drug treatment when combined with clinical data. Furthermore, we identified novel models containing informative clinical covariates and radiomic image features to predict drug treatment outcome. Our results implied that the texture features and first-order statistics features are the most valuable radiomic features for predicting drug treatment outcomes. Age of onset, infantile spasms, ASM numbers, epileptiform discharge in the left parieto-occipital area of EEG, and gene mutation type are the key clinical factors that are most likely to predict the epilepsy drug treatment outcome.
Footnotes
Zhanqi Hu, Dian Jiang, and Xia Zhao contributed equally to this study and are co-first authors.
Some of the work was partially supported by the Sanming Project of Medicine in Shenzhen (SZSM201812005), Shenzhen Key Medical Discipline Construction Fund (No.SZXK033), Shenzhen Fund for Guangdong Provincial High-Level Clinical Key Specialties (No.SZGSP012), Pearl River Talent Recruitment Program of Guangdong Province (2019QN01Y986), Shenzhen Science and Technology Program (JCYJ20210324115810030), National Natural Science Foundation of China (61871373, 81729003, and 81901736), and Shenzhen Fundamental Research Program (JCYJ2018 0228175428243).
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received July 31, 2022.
- Accepted after revision May 22, 2023.
- © 2023 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}