
Abstract
BACKGROUND AND PURPOSE: Mechanical thrombectomy appears to be a promising option for distal medium-vessel occlusions, for which intravenous thrombolysis is effective but may be insufficient when used alone. This study aimed to determine the optimal technique for these distal mechanical thrombectomies using the human placenta model.
MATERIALS AND METHODS: Twenty-four procedures were performed, allowing comparison of direct aspiration (n = 12) versus the combined technique (n = 12). Two positions of the aspiration catheter were tested for each of these techniques: in direct contact with the clot and at a distance from it (5–10 mm). Two types of clots were tested: red blood cell–rich clots and fibrin-rich clots. First-pass recanalization and induced arterial collapse and traction were assessed.
RESULTS: The first-pass recanalization was less frequent for direct aspiration than for the combined technique, without reaching statistical significance (41.7% versus 75.0%, P = .098). Full collapse (P < .001) and extended arterial traction (P = .001) were significantly less frequent for direct aspiration. For direct aspiration with the aspiration catheter not in direct contact with the clot, there was not a single first-pass recanalization and there was systematic arterial collapse, resulting in a no-flow in the aspiration syringe.
CONCLUSIONS: The combined technique appears to be more harmful, and although direct aspiration has a lower rate of first-pass recanalization, it seems appropriate to try direct aspiration as a first-line procedure. However, if the aspiration catheter cannot reach the clot, it is not useful or even risky to try aspiration alone. These results need to be confirmed by clinical studies.
ABBREVIATIONS:
- ACS
- arterial collapse score
- ATS
- arterial traction score
- DA
- direct aspiration
- DMVO
- distal medium-vessel occlusion
- FPR
- first-pass recanalization
- HP
- human placenta
- MT
- mechanical thrombectomy
- PLVO
- proximal large-vessel occlusion
- RBC
- red blood cell
Randomized controlled trials on acute ischemic stroke due to proximal large-vessel occlusion (PLVO) established the superiority of mechanical thrombectomy (MT) in addition to the best medical management, including IV thrombolysis, over the best medical management alone within 6 hours from symptom onset.1 More recent trials have demonstrated that the time window for MT can be extended up to 162 or 24 hours3 from the last time the patient was known well, when the selection is based on neuroimaging evaluation showing a salvageable penumbra2 or a mismatch between clinical deficit and infarct size.3 Different techniques are currently used to perform these procedures, including stent retriever alone, the direct aspiration (DA) technique, and the combined techniques (ie, using different techniques such as stent retriever and an aspiration catheter at the same time). However, there is no consensus on the optimal technique for thrombectomy.
Although IV thrombolysis is more effective for the small clots of distal medium-vessel occlusions (DMVOs) than for the large clots of PLVOs,4,5 IV thrombolysis alone is sometimes insufficient for DMVOs, recanalizing only one-third to one-half of the occluded vessels.6,7 With the iterative advances in device technology, MT is emerging as a promising solution for these DMVOs for several reasons:8 First, the considerable benefit of MT for PLVOs suggests that MT would also be beneficial for DMVOs; second, the advent of MT for PLVOs has led to rapid advances in catheter technology, leading to more navigable and smaller devices capable of reaching more distal and narrower vessels; third, an adverse event during MT for PLVOs is thrombus fragmentation with emboli in the distal arteries (thus, for maximum benefit from MT for PLVOs, rescue endovascular treatment of these distal emboli is desirable). Evaluation of Mechanical Thrombectomy in Acute Ischemic Stroke Related to a Distal Arterial Occlusion (DISCOUNT9) (NCT05030142) is a multicenter open, randomized controlled trial that is currently recruiting. The main objective of this trial is to assess the efficacy of MT in addition to the best medical treatment compared with the best medical treatment alone in acute ischemic stroke related to a DMVO.
The more tortuous access route and greater mobility of DMVOs, combined with thinner arterial walls, potentially increase the risk of complications, especially hemorrhages. Arterial collapse and traction induced by thrombectomy devices, particularly by avulsion of the cortical arteries or perforating branches, are phenomena thought to be responsible for these hemorrhagic complications.10 It is, therefore, necessary to study which techniques are the least harmful and most effective, especially between the DA technique and the combined technique, which are commonly used for this indication.11
The human placenta (HP) is a validated vascular model for interventional neuroradiology, using either the veins or arteries of the chorionic plate.12⇓⇓-15 The HP model has many advantages, including its relatively low cost, minimal infrastructure requirements, and ease of preparation and setup, with fewer ethical concerns compared with animal models. The aim of this translational study was to determine the optimal technique for these distal MTs by assessing first-pass recanalization (FPR), induced arterial collapse, and induced arterial traction, using this HP model.
MATERIALS AND METHODS
Angiogram Procedures, HP Model, and Clots
All procedures were performed with a monoplane angiographic system (Azurion; Philips Healthcare), allowing the acquisition of posterior-anterior 2D projections and 3D rotational angiography after injection of iodinated contrast medium. Iodixanol, 320-mg iodine/mL (Visipaque 320; GE Healthcare), was diluted to 70% with saline and injected manually (8 mL for 2D projections and 20 mL for 3D rotational angiography). All acquired images were converted to internationally compatible DICOM files.
After written consent was obtained from the mothers, 2 placentas were prepared with the methods previously described by our group,15 using the antiphysiologic direction (ie, using the chorionic plate veins as intracranial arteries). Briefly, the guidewire provided with an 8F introducer sheath was placed in the umbilical vein up to the chorionic plate veins, allowing positioning the introducer sheath with its dilator on this guidewire. The same strategy was used to catheterize each of the umbilical arteries up to the chorionic plate with 5F introducer sheaths. A suture was then placed around each umbilical vessel to avoid fluid reflux along them. A pressure bag was used to deliver a heparinized saline solution via an IV line into the venous introducer, dilating the vessels and removing the intraluminal clots. Another IV line was connected to each arterial introducer, and the other ends were placed in a tray, as the end of the circuit. To avoid any confusion and to allow the use of common terms, we will consider these chorionic plate veins as arteries for the remainder of this article.
Twenty-four clot analogs were generated using the methodology described by Duffy et al16 to obtain 2 types of clots: red blood cell (RBC)-rich clots, formed after spontaneous coagulation of ovine whole blood, and fibrin-rich clots, formed by mixing citrated plasma with RBCs in a 19:1 ratio (ie, 5% RBCs), which were subsequently coagulated.
MT
According to Saver et al,8 the intermediate, “medium vessels” can be defined as cerebral arteries with lumen diameters between 0.75 and 2.0 mm. To study the induced arterial collapse and traction on DMVOs produced by the different MT techniques, we therefore performed MTs on vessels of <2.0 mm in diameter. To ensure having vessels with a diameter of <2.0 mm and taking into account the potential random errors induced by the operator and the software, we used only vessels with diameters between 1.5 and 1.7 mm.
Revascularization was conducted by the following: 1) a DA technique with an aspiration catheter (3MAX; Penumbra), and 2) the combined technique with a 3 × 15 mm stent retriever (Catch Mini; Balt Extrusion) and an aspiration catheter (Fargomax; Balt Extrusion). Aspiration was generated by a 60-mL locking syringe (VacLok; Merit Medical). For the DA technique, the aspiration catheter was pushed close to the clot without crossing it with a microwire or microcatheter. We studied 2 positions of the aspiration catheter: in direct contact with the clot and at a distance from it (5–10 mm), simulating cases in which the clot cannot be reached by the aspiration catheter due to the tortuosities of the vessels or angulation. Ten seconds after the start of the manual aspiration, the aspiration catheter was removed. With the distal inner diameter of the 3MAX aspiration catheter being 0.89 mm, the vessel-to-catheter ratio was 1.7 to 1.9. For the combined technique, a microwire (Traxcess 14; MicroVention) and microcatheter (Headway 17; MicroVention) were directed through the clots. The stent was then loaded into the microcatheter and deployed across the clot using the unsheathing technique, with approximately two-thirds of the stent distal to the clot. The aspiration catheter was then guided coaxially along the microcatheter and the stent. In addition, for the combined technique, we studied 2 positions of the aspiration catheter: in direct contact with the clot and at a distance from it (5–10 mm). The stent was allowed to deploy for 5 minutes before removal using the Solumbra technique. An example of MT using the combined technique is shown in Fig 1.

MT of a fibrin-rich clot by the combined technique with the aspiration catheter at 5–10 mm from the clot. A, 3D acquisition after injection of iodinated contrast medium by the introducer. The black dotted arrow indicates the branch where the occlusion will be located. B, Snapshot of the roadmap performed at the beginning of the procedure, showing the branch occluded by the clot (black arrow). C, Stent retriever unsheathed across the clot. The distal markers of the stent are indicated by the black arrowhead. The tip of the microcatheter is indicated by the white arrowhead. Note that the stent is not yet fully deployed because this snapshot was taken immediately after unsheathing. D, Fibrin-rich clot removed.
FPR, Arterial Collapse, and Arterial Traction
FPR was defined as achieving a complete recanalization with a single thrombectomy device pass. Failure of FPR was defined by an inability to mobilize the clot or by distal embolization (ie, fragmentation of a primary clot downstream of the primary occlusion).
Possible arterial collapse induced during MT procedures was graded according to the arterial collapse score (ACS) described by Liu et al:17 ACS 0 when arteries remained unchanged; ACS 1 for indentation (ie, focal inward movement of 1 side of the arterial wall closest to the catheter tip); ACS 2 for flutter (ie, reciprocal cycles of focal collapse and re-expansion of the complete arterial lumen circumference distal to the catheter tip); ACS 3 for focal collapse (ie, sustained collapse of a short segment of the whole arterial lumen into the catheter tip); and ACS 4 for full collapse (ie, complete collapse of a long segment of the artery extending away from the catheter tip).
Arterial traction was divided into 3 grades: arterial traction score (ATS) 0 for no arterial traction; ATS 1 for local arterial traction (ie, mobilization of the thrombectomized arterial segment only); and ATS 2 for important extended arterial traction with or without avulsion.
Statistical Analysis
Categoric variables are presented as count (percentage). Statistical comparisons were performed by the χ2 and Fisher exact tests for categoric data. A P value < .05 was considered statistically significant. The data were analyzed using the Statistical Package for the Social Sciences (Version 28.0.1.1; IBM).
RESULTS
Two techniques (DA and combined technique), 2 clot types (RBC-rich and fibrin-rich clots), and 2 aspiration catheter positions (direct contact with the clot and at a distance from it [5–10 mm]) were tested with different combinations for a total of 24 procedures. The overall FPR rate was 58.3% (n = 14). Arterial collapse of any type occurred in 87.5% of the cases, with 50.0% ACS 3 (n = 12) and 37.5% ACS 4 (n = 9). We observed no indentation (ACS 1) or flutter (ACS 2). Arterial traction of any type also occurred in 87.5%, with 54.2% ATS 1 (n = 13) and 33.3% ATS 2 (n = 8). A detailed table of the results for each procedure is provided in the Online Supplemental Data. Examples of arterial collapse and arterial traction are shown in Fig 2. No contrast media extravasation was observed during the procedures.

MTs of a fibrin-rich clot (white arrow) by DA (A–C), and of an RBC-rich clot (black arrow) by the combined technique (D–F); both aspiration catheters (black arrowheads) are at 5–10 mm from the clot. The black star indicates the stent retriever for the combined technique. A, Before the start of the aspiration. B, After the start of the aspiration, focal collapse (ACS 3) at the tip of the catheter. C, When the aspiration catheter is removed, local arterial traction (ATS 1), the artery is pulled into the aspiration catheter. This is illustrated by the dotted black arrow. It was an FPR failure. D, Before the start of the aspiration. E, After the start of the aspiration, full collapse (ACS 4) of the proximal artery and both distal branches. The collapse extends away from the catheter tip; the stent-retriever is molded by the vessel wall. F, When the stent is being retrieved, note extended arterial traction (ATS 2) of all regional branches. This is illustrated by the dashed black arrows. It was an FPR success. Both cases are available in the Online Supplemental Data and Online Supplemental Videos 1 and 2.
DA versus Combined Technique
The main results are summarized in the Table. The FPR was less frequent for DA than for the combined technique, without reaching statistical significance (41.7% versus 75.0%, P = .098). ACSs were as follows: 25.0% ACS 0, 75.0% ACS 3, and 0.0% ACS 4 for DA; and 0.0% ACS 0, 25.0% ACS 3, and 75.0% ACS 4 for the combined technique. Full collapse (ACS 4) was significantly less frequent for DA (P < .001). ATSs were as follows: 25.0% ATS 0, 75.0% ATS 1, and 0.0% ATS 2 for DA; and 0.0% ATS 0, 33.3% ATS 1, and 66.7% ATS 2 for the combined technique. Extended arterial traction (ATS 2) was significantly less frequent for DA (P = .001).
Comparison of FPR, full collapse, and extended arterial traction induced by DA and the combined technique
Aspiration Catheter Position
The FPR was more frequent when the aspiration catheter was in direct contact with the clot than when it was at 5–10 mm from the proximal end of the clot, but it did not reach statistical significance (75.0% versus 41.7%, P = .098). ACSs were as follows: 25.0% ACS 0, 33.3% ACS 3, and 41.7% ACS 4 when the aspiration catheter was in direct contact with the clot; and 0.0% ACS 0, 66.7% ACS 3, and 33.3% ACS 4 when it was at 5–10 mm from the proximal end of the clot. Full collapse (ACS 4) was not significantly more frequent for either position of the aspiration catheter. ATSs were as follows: 25.0% ATS 0, 41.7% ATS 1, and 33.3% ATS 2 when the aspiration catheter was in direct contact with the clot; and 0.0% ATS 0, 66.7% ATS 1, and 33.3% ATS 2 when it was at 5–10 mm from the proximal end of the clot. Extended arterial traction (ATS 2) was not significantly more frequent for either position of the aspiration catheter.
For DA, when the aspiration catheter was in direct contact with the clot and the clot completely obstructed the tip of the catheter after the start of the aspiration (n = 3), there was neither collapse nor arterial traction, and in these cases, FPR was always successful (Fig 3). Conversely, when the aspiration catheter was not in direct contact with the proximal aspect of the clot, there was not a single FPR and there was a systematic arterial collapse, resulting in no-flow in the aspiration syringe and a systematic arterial traction. For the combined technique, when the aspiration catheter was at 5–10 mm from the proximal aspect of the clot, FPR occurred in 5 of 6 cases (83.3%), and when the catheter was in direct contact with the clot, FPR occurred in 4 of 6 cases (66.7%).

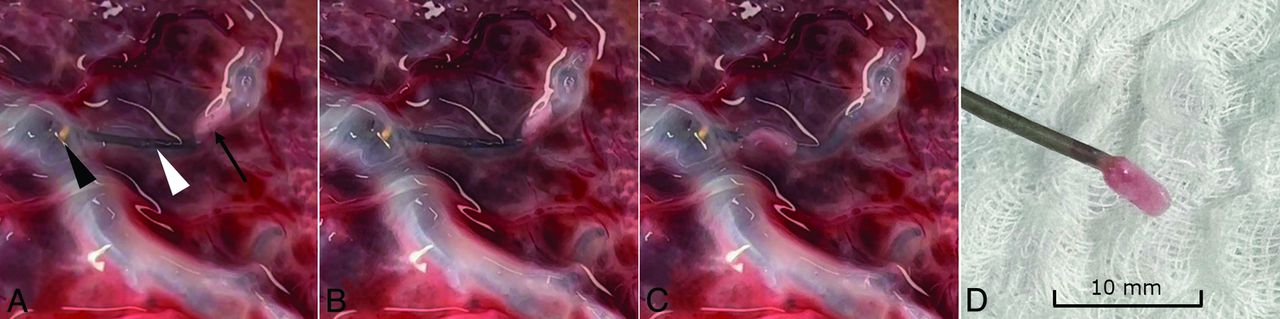
MT of a fibrin-rich clot by DA with the aspiration catheter in contact with the clot. A, The small aspiration catheter (white arrowhead) is placed in contact with the clot (black arrow) using a distal access catheter (the black arrowhead indicates the tip of this catheter). B, After the start of the aspiration, the clot is drawn toward the tip of the aspiration catheter, without any arterial collapse. C, When the aspiration catheter is removed, there is still no collapse and no arterial traction is observed. D, Removed fibrin-rich clot at the tip of the aspiration catheter. The case is available in Online Supplemental Data and Online Supplemental Video 3.
Types of Clots
The FPR was more frequent for fibrin-rich clots than for RBC-rich clots, without reaching statistical significance (75.0% versus 41.7%; P = .098). Of the failed FPRs, fragmentation occurred in 2 cases, with an RBC-rich clot in both cases.
DISCUSSION
The risk of complications, particularly hemorrhagic ones, is increased for MTs of DMVOs. Arterial collapse and traction induced by thrombectomy devices are phenomena considered potentially responsible for these hemorrhagic complications.10 However, because DMVOs can be debilitating in some locations, it seems that some distal MTs might be useful for well-selected patients. It is, therefore, necessary to study which techniques are effective and which are the least harmful, especially between DA and the combined technique, which are commonly used for this indication.11 The HP model is particularly well-suited for these investigations regarding MTs of DMVOs.15
The FPR rate was 58.3% in this study, which is consistent with the modified first-pass effect (ie, TICI 2b-3 after a single pass) rates found in the literature (52.4%).18 In our study, DA was associated with a lower FPR rate than the combined technique, without reaching statistical significance (P = .098). This finding is similar to what is found in the literature. Abbasi et al18 published a meta-analysis regarding PLVOs in 2021, which showed that the modified first-pass effect rates were 48% (1653/3191) for DA and 58% (193/333) for the combined technique. As in our study, these rates were not significantly different (P = .22).
In our study dedicated to distal thrombectomies, we observed no indentation (ACS 1) or flutter (ACS 2). Focal or full arterial collapse (ACS 3 or 4) occurred in 87.5% of cases. This result is consistent with the findings of Liu et al,17 who initially defined 4 stages of arterial collapse for PLVOs but observed ACS 3 or 4 in 98% of cases in the M2 branches. DA was associated with significantly less full arterial collapse (P < .001) and extended arterial traction (P = .001) than the combined technique. Arterial collapse, especially if full, and arterial traction, especially if extended, are possibly responsible for the high rates of SAH seen during MTs of DMVOs.10 Thus, because the combined technique appears to be more harmful and even though DA has a probable lower rate of FPR, it seems relevant to try DA as the first-line procedure in thrombectomies of DMVOs.
There was not a single FPR for DA when the aspiration catheter was not in direct contact with the proximal aspect of the clot. The usual way to recognize clot engagement in the aspiration catheter is to activate aspiration and wait until there is no flow in the canister or the aspiration syringe. We have found that arterial collapse also results in a no-flow situation, which can be misinterpreted as clot engagement. Moreover, the aspiration catheter being withdrawn while the arterial wall is being aspirated can cause arterial traction, which can lead to intracranial hemorrhage, without any chance of recanalization. This issue suggests that if the clot cannot be reached with the aspiration catheter, there is little point in trying aspiration alone. For the combined technique, the FPR rates were good regardless of the position of the aspiration catheter (83.3% and 66.7%). Therefore, contrary to DA, it appears relevant to use aspiration in addition to the stent retriever, even if the aspiration catheter cannot reach the clot.
We found that the FPR was more frequent for fibrin-rich clots than for RBC-rich clots, a finding not consistent with findings in the literature.19⇓-21 We hypothesized that this finding was due to less interaction between the arterial wall and the clot in this HP model compared with real-world conditions, whereas this interaction in real-world conditions might be more important with fibrin-rich clots compared with RBC-rich clots. This lack of interaction is one of the inherent limitations. In addition, for our experiments, the clots were removed within minutes after placement, whereas in real patients, clot removal is usually performed after several hours. This delay most likely allows greater interaction between the clot and the arterial wall.
While initial stent retrievers had radial diameters of 6 and 4 mm, smaller devices have recently been developed to be more suitable for distal thrombectomies, including 3-mm-diameter devices (eg, the Catch Mini; pREset LITE, phenox; Trevo NXT ProVue, Stryker Neurovascular; and, more recently, Solitaire X, Medtronic) and a 2.5-mm diameter device (eg, the Tigertriever 13; Rapid Medical).8 For the combined technique in this study, we used the Catch Mini stent retriever, which has the important advantage of being usable with the 0.017- and 0.013-inch microcatheters.22
One limitation of this study is that the results might have been different with any of the other commercially available stent retrievers. Unfortunately, to the best of our knowledge, there are no studies comparing these devices in terms of safety and effectiveness.
There are a few other limitations we would like to acknowledge. First, in this model, there is no collateral circulation as in the human brain, and extrapolation to human cerebral arteries must be done with caution because arterial collapse might be overestimated. Second, the semitransparent nature of the chorionic plaque is a definite advantage of this model because it allows macroscopic observation of clots and device behavior, but it also allows improved positioning of the aspiration catheter and stent retriever compared with real-world conditions, which may have increased the FPR rate. Third, the ACS (developed by Liu et al17) and ATS scales were developed on the basis of testing in ex vivo models and may not be translatable to patients. Techniques to monitor the mechanical response of arteries in living patients are needed.
CONCLUSIONS
The combined technique appears to be more harmful, and although DA has a lower rate of FPR, it seems appropriate to try DA as a first-line procedure. However, if the clot cannot be reached by the aspiration catheter, it is not useful and is even risky to try aspiration alone. Conversely, for the combined technique, it seems relevant to use aspiration, even if the aspiration catheter cannot reach the clot. These results need to be confirmed by clinical studies.
Acknowledgments
We would like to thank Mr Denis Biaussat and Balt Extrusion for their valuable assistance, particularly in obtaining the Catch Mini stent retrievers and Fargomax catheters. We would also like to thank Mrs Fabienne Santini and Penumbra for their valuable assistance, particularly in obtaining the 3MAX aspiration catheters. We would also like to thank Mr Mahmood Mirza, Mrs Sarah Johnson, and Cerenovus for their valuable assistance, particularly in obtaining the clot analogues.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received December 5, 2022.
- Accepted after revision February 23, 2023.
- © 2023 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.