
Abstract
BACKGROUND AND PURPOSE: There is active research involving the radiographic appearance of the skull base following reconstruction. The purpose of this study was to describe the radiographic appearance of the vascularized pedicle nasoseptal flap after endoscopic skull base surgery across time.
MATERIALS AND METHODS: We performed chart and imaging review of all patients with intraoperative nasoseptal flap placement during endoscopic skull base surgery at a tertiary academic skull base surgery program between July 2018 and March 2021. All patients underwent immediate and delayed (>3 months) postoperative MR imaging. Primary outcome variables included flap and pedicle enhancement, flap thickness, and flap adherence to the skull base.
RESULTS: Sixty-eight patients were included. Flap (P = .003) enhancement significantly increased with time. Mean nasoseptal flap thickness on immediate and delayed postoperative scans was 3.8 and 3.9 mm, respectively (P = .181). The nasoseptal flap adhered entirely to the skull base in 37 (54.4%) and 67 (98.5%) patients on immediate and delayed imaging, respectively (P < .001).
CONCLUSIONS: Our findings demonstrate heterogeneity of the nasoseptal flap appearance after skull base reconstruction. While it is important for surgeons and radiologists to evaluate variations in flap appearance, the absence of enhancement and lack of adherence to the skull base on immediate postoperative imaging do not appear to predict reconstructive success and healing, with many flaps “self-adjusting” with time.
ABBREVIATIONS:
- EEA
- endoscopic endonasal approaches
- ESBS
- endonasal skull base surgery
- NSF
- nasoseptal flap
Advancements in surgical techniques and instrumentation have revolutionized endoscopic endonasal skull base surgery (ESBS) from the resection of transsellar masses to a wide spectrum of lesions along the ventral skull base.1⇓⇓⇓-5 With endoscopic endonasal approaches (EEAs), intraoperative CSF leaks or large bony defects with dural exposure or both are often encountered.6 The mainstay of skull base reconstruction with EEA has become the nasoseptal flap (NSF).7,8 The NSF is a vascularized pedicled flap that consists of mucoperiosteum and/or mucoperichondrium supplied by the posterior septal branch of the sphenopalatine artery.9 First described in 2006 by Hadad et al,8 the NSF has gained popularity for skull base reconstruction due to its rich blood supply and wide coverage. With its use, the incidence of a postoperative CSF leak after ESBS has significantly decreased.10
The NSF, unlike other vascularized flaps, cannot undergo traditional monitoring with Doppler or other manual or visual methods. Because frequent endoscopic evaluation is not feasible postoperatively, MR imaging is commonly used to assess the viability of the NSF after surgery.11 Previously, radiologists have looked for flap enhancement as a sign of flap viability. However, a recent study suggested the unreliability of flap enhancement as a proxy for flap viability or as a predictor of postoperative CSF leaks.12 Reported findings, while limited, have suggested a nonenhancing mucosal gap and displacement of the NSF as possible reasons for postoperative CSF leaks.13
Postoperative imaging can also be used to assess flap positioning and changes in appearance with time. Preliminary studies of the radiographic findings of NSFs have reported various changes in thickness and enhancement on follow-up MR imaging, with 1 study by Learned et al12⇓⇓-15 reporting stabilization of the imaging features within 2–6 months after surgery. However, there is a general paucity of literature examining the radiographic appearance of the NSF so far. This study therefore aimed to systematically describe the immediate and delayed MR imaging characteristics of the vascularized pedicle NSF and to demonstrate its evolution with time to help clinicians better understand the natural progression of the radiographic appearance of the NSF.
MATERIALS AND METHODS
After the University of California, Irvine, institutional review board approval, we conducted a retrospective review of all patients undergoing endoscopic skull base surgery with intraoperative NSF placement for reconstruction of skull base defects between July 2018 and March 2021. Patients with both sellar and nonsellar pathology were included as long as the NSF was used (eg, transcribriform, transplanum, and transclival approaches were included). Imaging criteria for all postoperative scans were defined by consensus by a rhinologist/skull base surgeon (E.C.K.) and a neuroradiologist (E.K.). Two separate physicians (E.K. and E.C.K.) independently reviewed each case to ensure interobserver agreement, with disagreements resolved after further discussion.
All patients underwent preoperative MR imaging within 48 hours of the operation, immediate postoperative MR imaging within 48 hours of the operation, and delayed postoperative MR imaging at least 3 months after the operation. Features evaluated included enhancement of the pedicle and flap (ie, no, weak, or bright enhancement) as evaluated on T1 postgadolinium sequences, flap thickness (in millimeters), flap adherence to the skull base (defined as absence or presence of gaps between the flap and skull base along the length of the flap), and diaphragma sellae descent for both immediate and delayed postoperative MRIs. Flap enhancement was quantified as follows: For each MR imaging, a 200 × 100 pixel window consisting of the flap and pedicle was extracted. Flap enhancement was calculated as the average pixel intensity (range, 0–255 pixels) of the extracted images. The 33rd and 66th percentile intensities were computed from the resulting list of enhancement values, which were used as thresholds to stratify flap and pedicle enhancement into 3 categories: no, weak, or bright enhancement. Representative figures demonstrating no, weak, and strong enhancement based on our objective criteria are shown in Fig 1.

Representative figures of no enhancement (A), weak enhancement (B), and bright enhancement (C).
We collected data on overall patient demographics, tumor location, cavernous sinus involvement, suprasellar involvement, American Society of Anesthesiologists (ASA) status, prior transnasal surgery, prior radiation to the lesion, tumor pathology, surgical approach (ie, standard versus extended), intraoperative leak (ie, no leak, low-flow leak, high-flow leak), the presence of a postoperative CSF leak, and lumbar drain use for both groups (Online Supplemental Data).
All statistical analyses were performed using PASW 18.0 (https://www.malavida.com/en/soft/pasw/). Paired t tests were performed for continuous variables to assess differences in outcomes between immediate and delayed postoperative MR images. McNemar and marginal homogeneity tests were used for 2 and 3 or more categoric variables, respectively, to assess changes between immediate and delayed postoperative images. P values ≤ .05 were considered statistically significant.
RESULTS
All 68 patients had observable skull base defects with coverage by the flap, with the C-shaped NSF concave into the operative defects on postoperative coronal and/or sagittal views in all patients. Patient demographics and clinical characteristics are listed in the Online Supplemental Data. There were no postoperative CSF leaks in this cohort. In the 39 patients with a change in NSF enhancement, 27 (69%) flaps increased in enhancement and 12 (31%) flaps decreased in enhancement with time. Fifty-seven percent of flaps changed in enhancement pattern by 4 months after the operation. There were 27 (40%) NSFs that increased and 41 (60%) that decreased in thickness with time. A list of tumor pathologies is presented in Table 1. Changes in flap and pedicle enhancement, mean flap thickness, and NSF adherence to skull base descent between immediate and delayed MR imaging are reported in Table 2. Examples of changes in NSF enhancement, skull base adherence, and thickness are demonstrated in Figs 2–4, respectively.
Tumor pathology of all 68 patients
Changes in outcome variables between immediate and delayed postoperative MR imaging

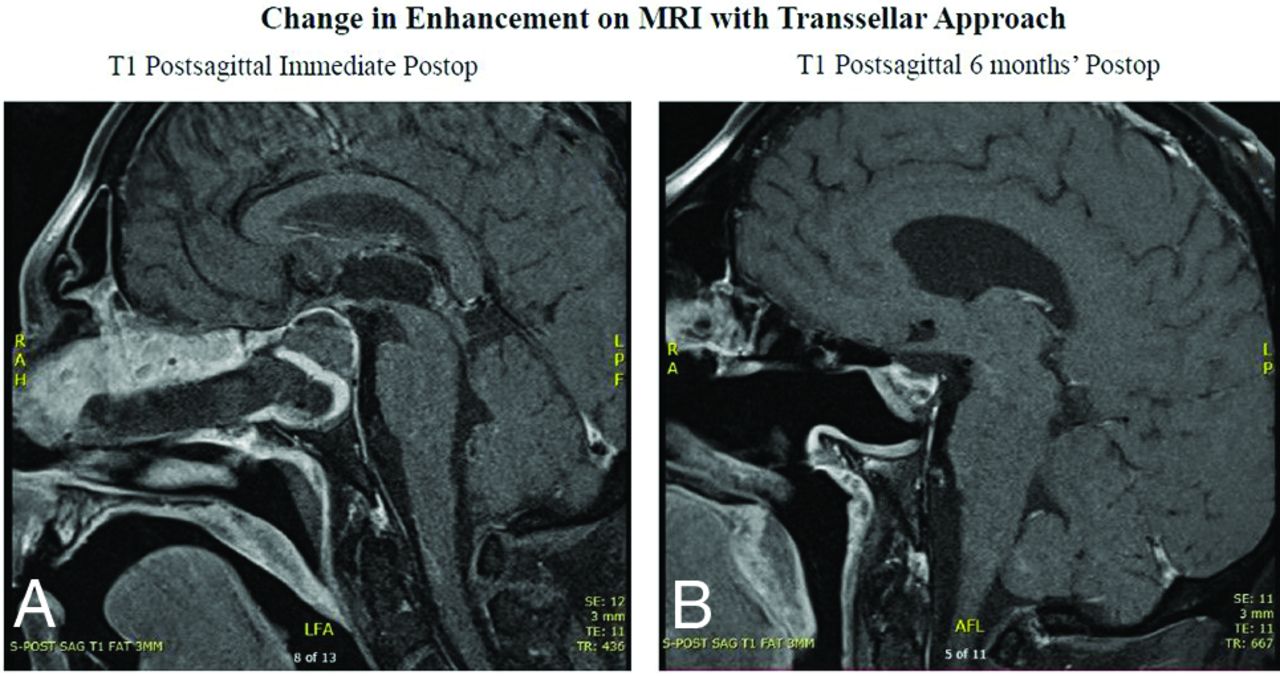
A, Immediate postoperative imaging following resection of an endoscopic transsellar pituitary adenoma with an intraoperative CSF leak demonstrates full coverage of sellar defect with the NSF in the shape of a C. There is elevation of the diaphragma sellae and compression of the pituitary gland. The flap pedicle and body are both brightly enhancing, with complete adherence to the skull base. B, Delayed imaging demonstrates continued enhancement of the flap with complete adherence to the skull base, as well as re-expansion of the pituitary gland and collapse of the diaphragma sellae.

A, Immediate postoperative imaging following resection of an endoscopic transsellar pituitary adenoma with an intraoperative CSF leak shows full coverage of sellar defect, demonstrating that the enhancing nasoseptal flap appears to be nonadherent to the skull base. B, Delayed imaging confirms that the flap is now uniformly opposed to the skull base.

A, Immediate postoperative imaging following an endoscopic unilateral transcribriform approach to an olfactory groove meningioma demonstrates that the flap extends into the defect with bright enhancement. B, Delayed imaging demonstrates mild thinning of the flap with mildly decreased enhancement. Preop indicates preoperative.
DISCUSSION
EEA is a relatively new surgical technique used to resect lesions along the skull base, allowing a wider FOV, improved illumination, and the ability to directly access tumors while avoiding vital structures.16⇓-18 However, EEA can often create large surgical defects and is associated with the risk of CSF leaks with possible increased morbidity and hospital length of stay.12 Various attempts have been made to address this dilemma, including the use of fat grafts and extranasal vascularized flaps; however, the risk of a CSF leak with these techniques remained unacceptably high and often added to postoperative morbidity. The NSF is now considered the criterion standard when reconstructing skull base defects after ESBS because it has demonstrated superiority in decreasing postoperative CSF leaks in EEA procedures whenever feasible.7,10,15,19,20 The mainstay for radiographic evaluation of the NSF has been MR imaging. While imaging can be used to assess tumor resection and surveillance with time, it can also provide valuable information on NSF enhancement, thickness, positioning, and adherence to the skull base.
In this study, we report heterogeneity in flap appearance on immediate imaging and across time. We found that nearly 60% of NSFs changed in enhancement, with a trend toward increased NSF enhancement on delayed MR imaging (27/39; 69%). Additionally, our study did not find significant changes in flap thickness (P = .181). Flap adherence to the skull base significantly increased (P = .181), with 98.5% of all NSFs adherent to the skull base on delayed MR imaging. These results provide a better understanding for clinicians on the natural progression of the radiographic appearance of the NSF postoperatively and should assist them in identifying abnormal radiographic findings in future cases.
Variations in flap enhancement on MR imaging have been conventionally used as a predictor of flap failure and the risk of a CSF leak, especially in larger skull base defects when NSFs are used. It has been hypothesized that there is an increased risk of CSF leak in poorly enhancing NSFs due to compromised vasculature. This is thought to be due to injury to or compression of the vascular supply.15 Our study as well as others have since challenged the notion that enhancement patterns can predict flap failure.12 As mentioned in previous studies, more likely reasons for a CSF leak include NSF migration or displacement, which would appear as a nonenhancing mucosal gap on imaging.12,13 Although this study did not find enhancement predictive of NSF necrosis, a recent study by Chabot et al21 reported a lack of enhancement on MR imaging as a predictor of NSF necrosis. Therefore, if suspicion for flap failure is high (eg, signs of meningitis, clear rhinorrhea), MR imaging may be warranted to better evaluate the NSF.
Most interesting, we also found no relationship between the direct adherence of the NSF to the skull base and subsequent development of postoperative CSF leaks. As reported in this study, only 54% of NSFs were directly adherent to the skull base on immediate postoperative imaging, with an increase to 98.5% on delayed MR imaging. To our knowledge, this feature has not been previously reported and should reassure clinicians that the NSF will improve its direct adherence to the skull base with time. One explanation for this finding is that NSF adherence likely improves as granulation tissue forms and the flap scars down onto the underlying bone. Additionally, the senior author routinely performs multilayer reconstruction using subdural and/or epidural underlay materials, which can also create an artificial space between the flap undersurface and skull base. These materials may break down and may also account for improved flap adherence with time.
Additionally, we found no significant changes in NSF thickness between immediate and delayed postoperative imaging. This finding contrasts with a prior study by Learned et al,14 which reported a 20%–30% reduction in flap thickness with time. Any increased thickness on delayed postoperative imaging may be due to flap neovascularization that increases flap thickness. However, this feature did not significantly change the thickness across time in our study.
In the current study, we also compared enhancement changes between immediate and delayed postoperative imaging. We found 19 flaps that did not enhance at all on immediate postoperative imaging but ultimately increased in enhancement on delayed imaging, suggesting neovascularization across time as the flap healed over the skull base. Although the NSF may not have been brightly enhancing originally, this characteristic does not appear to affect its long-term integration and healing. We showed 94% flap enhancement (ie, weak or bright) on delayed postoperative imaging. This enhancement pattern on delayed postoperative imaging appears to be similar to that seen with free mucosal graft reconstruction because a prior study by Kim et al22 reported 100% flap enhancement at 3 months after ESBS. This study did not assess free mucosal graft enhancement with time and thus cannot determine whether cases reconstructed with a free mucosal graft have similar enhancement changes from the immediate postoperative imaging to delayed imaging.
Given that CSF leaks were not observed in any patient, it is unlikely that weak-to-no enhancement of the NSF predicts flap failure. Additionally, 9 flaps that originally displayed strong enhancement decreased enhancement with time, suggesting that a decrease in enhancement is also unlikely to predict flap failure. These data, in accordance with prior literature, suggest that using MR imaging to evaluate NSF enhancement serves as a poor proxy for determining flap viability. In these scenarios, a meticulous closure technique, proper flap placement, optimizing wound-healing status, and enforcement of postoperative precautions likely play a larger role in reconstructive success. There is merit, however, in using MR imaging to determine the risk of CSF leak as it relates to flap position and placement as per the studies by Adappa et al12 and Learned et al.13
An alternative theory for an increase in flap enhancement with time may be due to reactive changes such as granulation tissue or mucosalization of the flap itself.15 Granulation tissue typically develops within 3–7 days after the operation and would not be evident at the time of the immediate postoperative MR imaging, which was acquired within the first 48 hours.23 It is, therefore, reasonable to think that granulation tissue would be present on delayed postoperative imaging and may affect flap thickness and enhancement. Although we demonstrate a significant increase in NSF enhancement with time, we did not see a corresponding increase in the thickness of the enhanced tissue. Given these findings, enhancement changes over time are most likely due to changes to the vascularity of the flap rather than secondary to tissue changes of the surrounding tissue. Hypotheses for the increased vascularity of the flap with time are 2-fold. First, the flap is initially compressed and placed on tension as it is rotated back to cover the skull base defect. As the flap matures, there is likely reduced tortuosity on the flap that improves blood flow to the flap. Second, neovascularization near the flap edges that occurs during flap healing likely plays a significant role in the increase in enhancement to the flap.
Limitations
Limitations to the study included its retrospective nature and the limited sample size and the variable interval of the second postoperative imaging. While this study included only 44 patients, this is the largest cohort to date investigating the radiographic appearance of the NSF, to our knowledge. Although several materials were used during the multilayer reconstruction in each case (eg, collagen matrix as underlay, dural sealant, and dissolvable nasal dressings superficial to the flap), this study focused its analysis on the findings of the NSF itself, which is a distinct, readily identifiable, and critical layer for reconstruction. Additionally, we were unable to statistically analyze risk factors for CSF leaks, given that we did not observe any postoperative CSF leaks in our study. Future large-scale, prospective studies are required to better understand radiographic predictors of NSF failure and postoperative CSF leaks.
CONCLUSIONS
Understanding the appearance of the NSF and its changes in postoperative appearance with time is essential for surgeons and radiologists. Our findings demonstrate that the NSF tends to increase in enhancement, with most flaps changing enhancement patterns by 4 months postoperatively. These findings should assist surgeons and radiologists in better appreciating the evolution of the NSF.
Footnotes
A. Abiri and T. Nguyen contributed equally to this work.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received May 8, 2022.
- Accepted after revision December 6, 2022.
- © 2023 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.