
Article Figures & Data
Figures
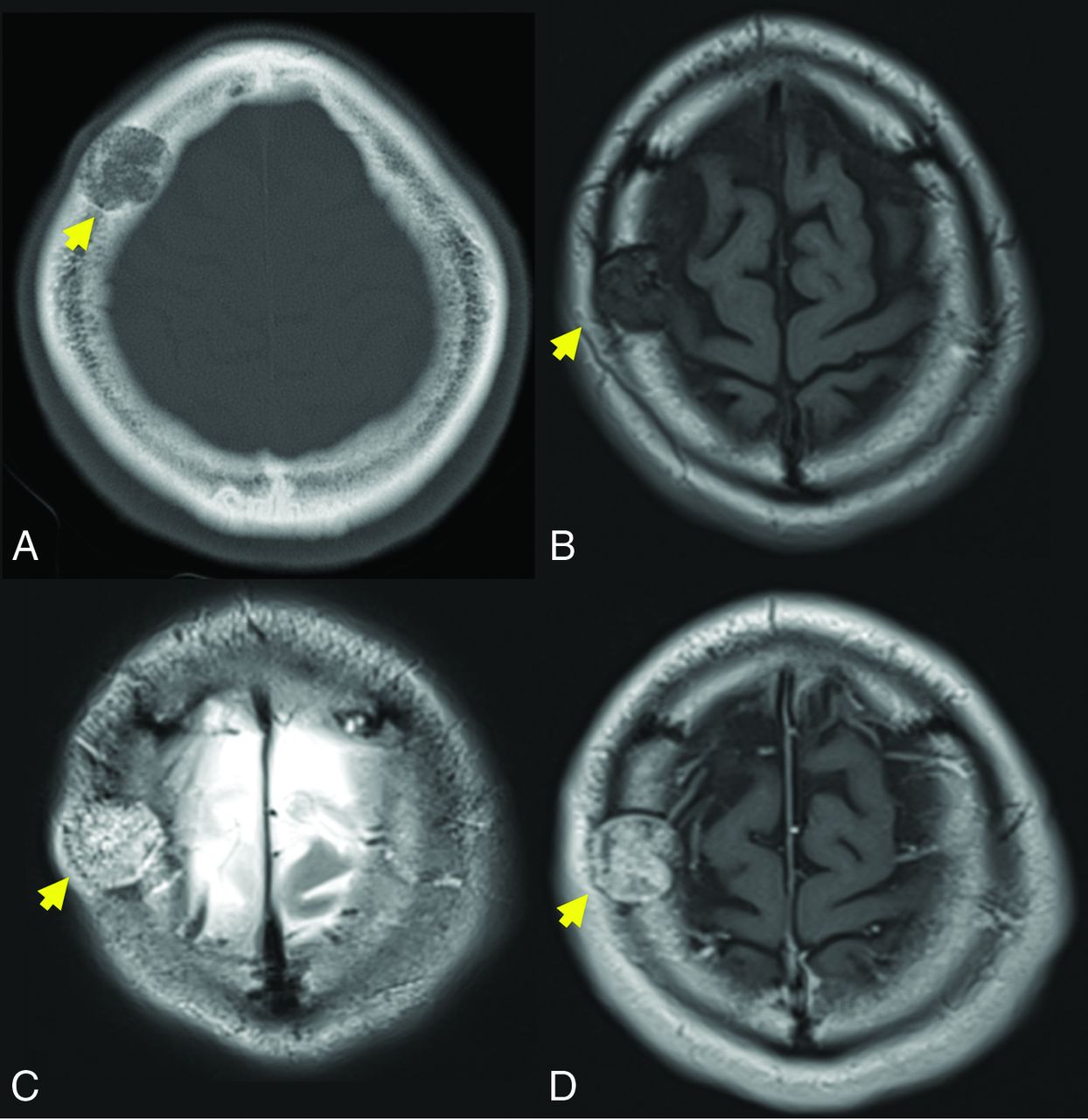
- FIG 1.
A 39-year-old man with a slowly growing calvarial mass. Axial CT (A) demonstrates a lucent right frontal bone lesion centered in the diploic space with a honeycomb pattern of internal calcification (arrow). Note a minimal overlying scalp deformity; the patient was able to palpate this slowly growing lesion. The lesion (arrow in B–D) demonstrates intermediate signal on T1WI (B), marked hyperintensity on T2WI (C), and prominent contrast enhancement, T1WI C+ (D). Note the internal foci of low signal most prominent on the T2-weighted examination (C) corresponding to the internal bone spicules evident on the CT. The diagnosis of IOVM was made on the basis of the characteristic imaging appearance. C+ indicates with contrast.
- FIG 2.
A 40-year-old man with a palpable frontal bump. Axial (A) and sagittal (B) thin-section CT images demonstrate a typical expansile lucent lesion with internal spiculated calcification (yellow arrow, A and B). Intraoperative photograph (C) shows a raised, red, porous-appearing calvarial lesion. H&E-stained photomicograph (D) shows dilated cavernous blood-filled spaces lined by flattened epithelium, characteristic of a venous malformation. There is focal hemosiderin staining, which is evidence of prior hemorrhage.
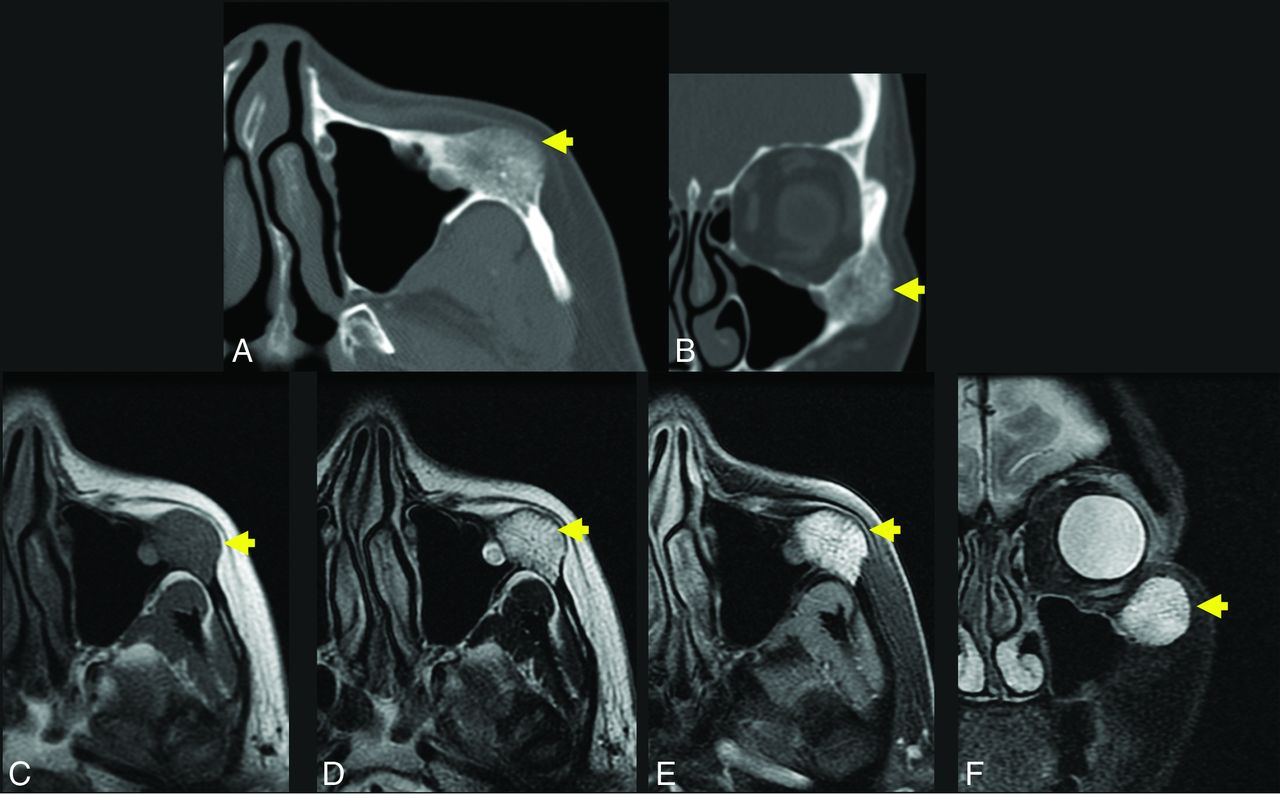
- FIG 3.
A 56-year-old woman with a palpable facial mass. The yellow arrow indicates a lesion in A–F. Axial (A) and coronal (B) thin-section CT in bone windows demonstrates an expansile, low-density lesion with internal coarsened trabeculae. The characteristic internal honeycomb pattern is typical of an IOVM. Axial T1 C– (C) and axial T1 C+ FS (D) sequences demonstrate a T1-intermediate, avidly enhancing lesion that extends beyond the cortical margin; the cortex is thinned but identifiable. Axial T2 FS (E) and coronal T2 FS (F) sequences demonstrate that the lesion is markedly T2 hyperintense. The diagnosis of IOVM was made on the basis of the characteristic imaging appearance, and the lesion remained stable on surveillance imaging for 3 years. C+ indicates with contrast; C–, without contrast.
- FIG 4.
Axial T1 (A) and axial T1 C+ FS (B) images through the maxilla demonstrate a T1-intermediate, heterogeneously enhancing expansile lesion centered in the right maxillary alveolus (yellow arrow, A and B). The lesion extends beyond the cortical margin, and there is poor identification of the normal cortex. Axial T2 (C) and axial T2 FS (D) sequences demonstrate that the lesion is T2-hyperintense with internal T2-hypointense trabeculae (yellow arrows, C and D). The diagnosis of IOVM was confirmed on pathology. C+ indicates with contrast.
- FIG 5.
Axial T1-weighted (C) and axial T1-weighted C+ (B) demonstrate an expansile lesion centered within the left greater wing of the sphenoid, with internal T1-hypointense trabeculae and avid enhancement (yellow arrows, A and B). There is mass effect on the left orbit, with resultant proptosis. Axial T2WI (C) demonstrates that the lesion is heterogeneous but predominantly T2 hyperintense (yellow arrow, C). There is vasogenic edema in the subjacent left temporal operculum, presumably based on mass effect, a response to hypervascularity, and venous congestion. Axial CT (D) is confirmatory for the diagnosis of the IOVM, given the presence of thickened internal trabeculae (yellow arrow, D) in a characteristic pattern. The patient was treated with surgical resection. The diagnosis of IOVM was confirmed on pathology, which showed dilated thin-walled blood vessels distending and replacing medullary bone. C+ indicates with contrast. Case courtesy of Phillip Chapman, MD, Professor of Radiology, Duke University School of Medicine.
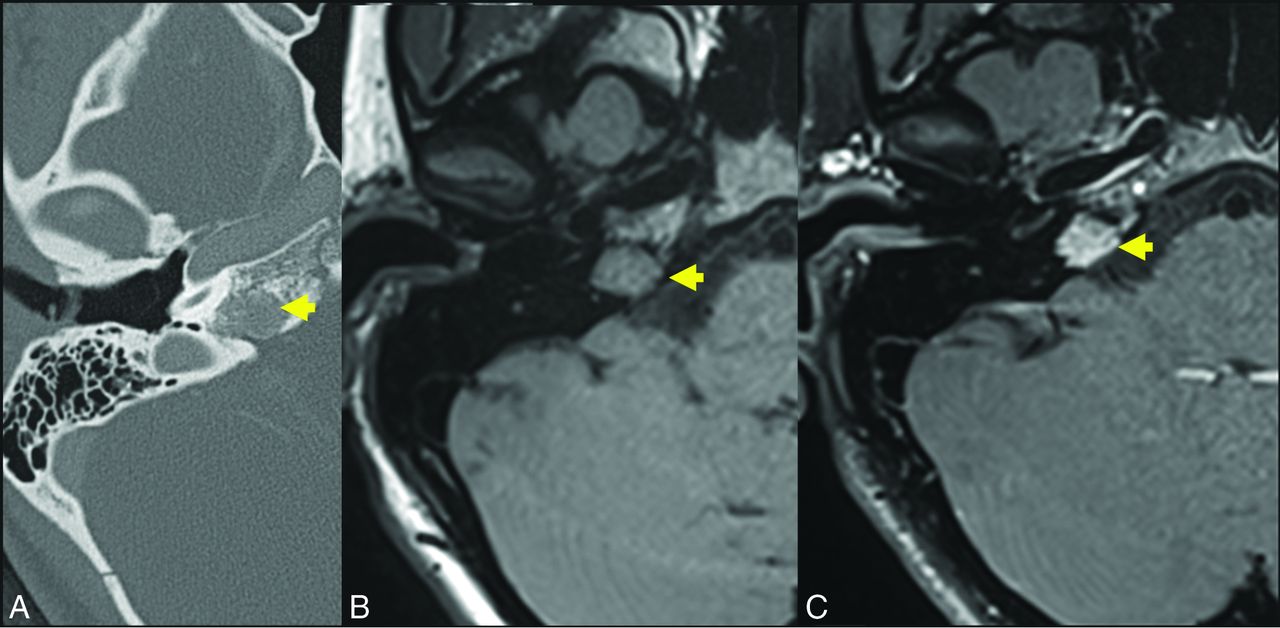
- FIG 6.
A 17-year-old girl referred for suspicion of paraganglioma identified incidentally on head CT for trauma. Axial thin-section CT (A) demonstrates a hypodense lesion centered in the right petrous apex (yellow arrow). The presence of internal trabeculae in a honeycomb pattern as well as the lesion location differentiate the correct diagnosis (IOVM of the skull base) and the suspected diagnosis of glomus jugulare paraganglioma. Axial T1 C– (B) and axial T1 C+ (C) sequences through the skull base demonstrate that the lesion is T1-intermediate (yellow arrow, B) and avidly enhancing (yellow arrow, C). A diagnosis of IOVM was made on the basis of characteristic imaging appearance. C+ indicates with contrast; C–, without contrast.
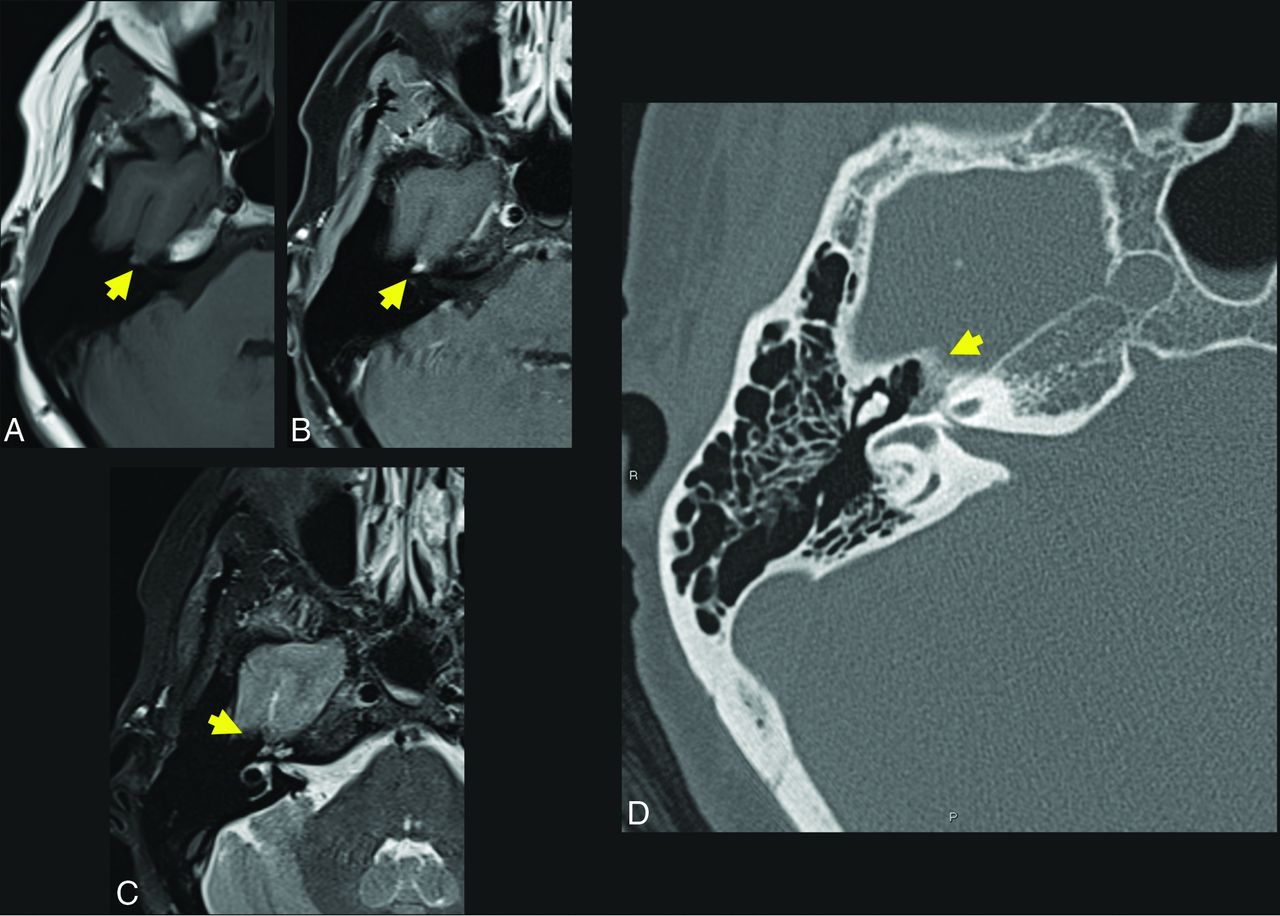
- FIG 7.
A 57-year-old woman who presented with right facial synkinesis. Noncontrast T1WI (A) and contrast-enhanced T1WI (B) demonstrate an enhancing lesion centered at the level of the right FN hiatus (yellow arrow, A and B), with corresponding increased signal on T2WI (C, yellow arrow indicates lesion). Differential considerations included both schwannoma and IOVM of the FN. Axial (D) thin-section CT of the temporal bone demonstrates an expansile, lucent lesion at the level of the anterior genu of the FN and FN hiatus (yellow arrow, D). The internal trabeculae help to confirm the diagnosis of IOVM because schwannoma would be less likely to show internal calcification. The diagnosis of IOVM was confirmed on pathology.







Tables
Category Incorrect Correct Calvaria Calvarial hemangiomaOssifying hemangiomaCavernoma of the skull Intraosseous vascular malformation (venous)Low-flow vascular malformation of the bone Facial skeleton Facial bone hemangiomaIntrabony hemangiomaCellular hemangioma Intraosseous vascular malformation (venous)Low-flow vascular malformation of the bone Skull base/facial nerve FN capillary hemangiomaFN cavernous hemangioma Intraosseous vascular malformation (venous)Low-flow vascular malformation of the bone Diagnosis CT Findings MR Imaging Findings IOVM Expansile and well-circumscribedCortex intact, but thin/scallopedStippled internal trabeculae, or,Honeycomb/spoke wheel ossification T2-very hyperintense, with internal stippled or striated signal voidT1 signal varies, thrombus may be brightT1 + gadolinium–avid enhancement Intraosseous meningioma Dense marrow sclerosis and shaggy cortical hyperostosisExtraosseous soft tissue T2 intermediateT1 + gadoliniumIntraosseous: ± enhancementExtraosseous: avid plaquelike enhancement Fibrous dysplasia Ground-glass matrix, ± cystic or more sclerotic elements T2 low-intermediate signal, though varies depending on cystic changeT1 + gadolinium: avid enhancement Metastasis, myeloma No matrixCortical lysisMultiplicity Variable, depending on primary tumor Lymphoma No matrixHyperdense soft tissue T2 intermediate, T1 + gadolinium: bland enhancementDiffusion-restriction, hypercellularity Chondrosarcoma Rings/whorls of calcified matrixClassic location, petroclival T2 marked hyperintensityEnhancement, variable but often mild Epidermoid cyst Low densityNo internal matrix T1-hypointense, T2-hyperintenseDiffusion restrictionNo internal enhancement




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.