
Article Figures & Data
Figures
- FIG 1.
Derivation of the 3 major study groups, the subgroups of HIBI, and the subtypes of watershed patterns of injury in patients who had partial, prolonged HIBI.
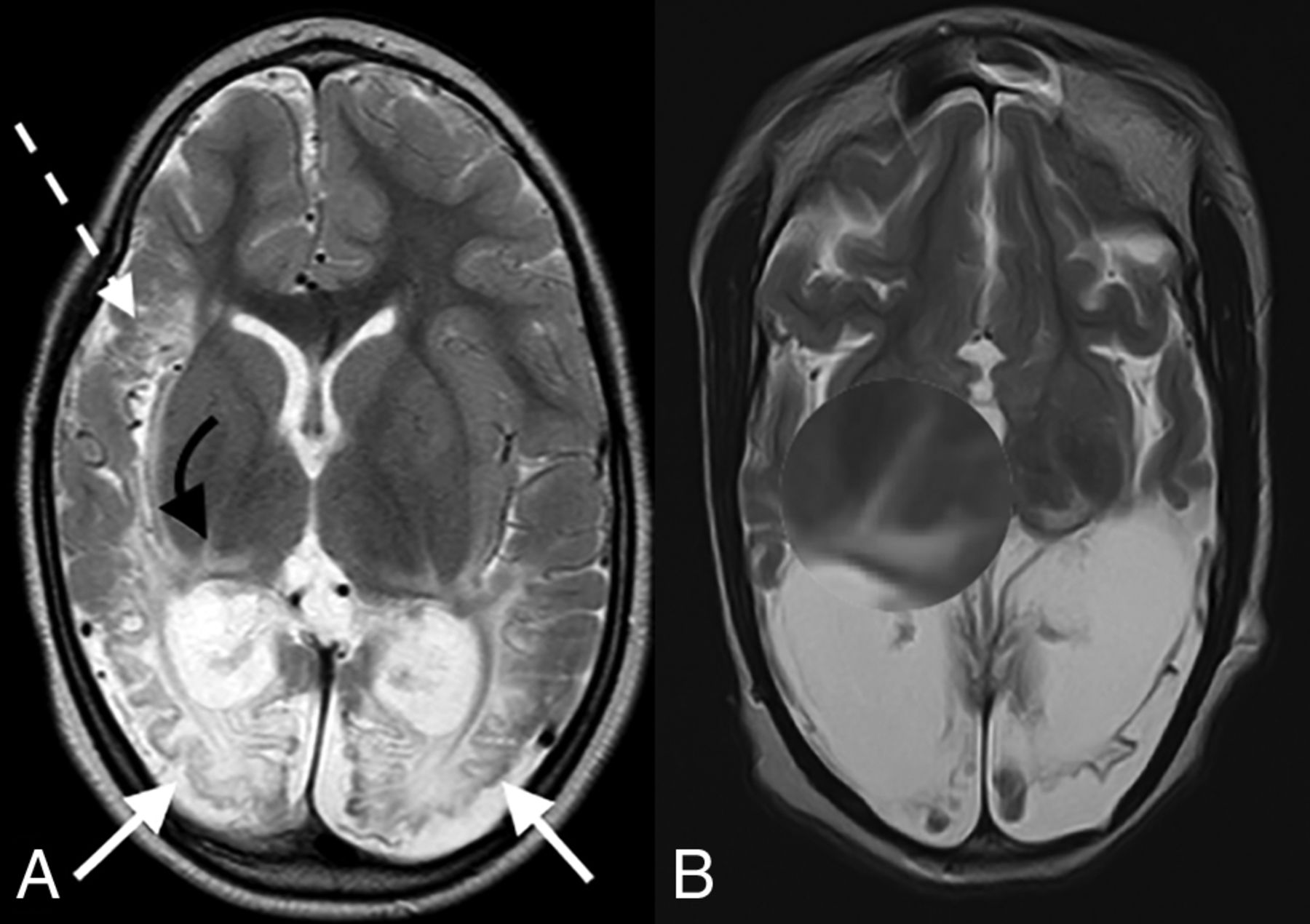
- FIG 2.
Axial T2-weighted images in a child with partial, prolonged HIBI demonstrating interarterial injuries at the peri-Sylvian (dashed white arrow) and posterior parieto-occipital (solid white arrows) watershed regions. Note the thalamus L-sign (curved arrows in A and highlighted by the loupe in a second patient in B).
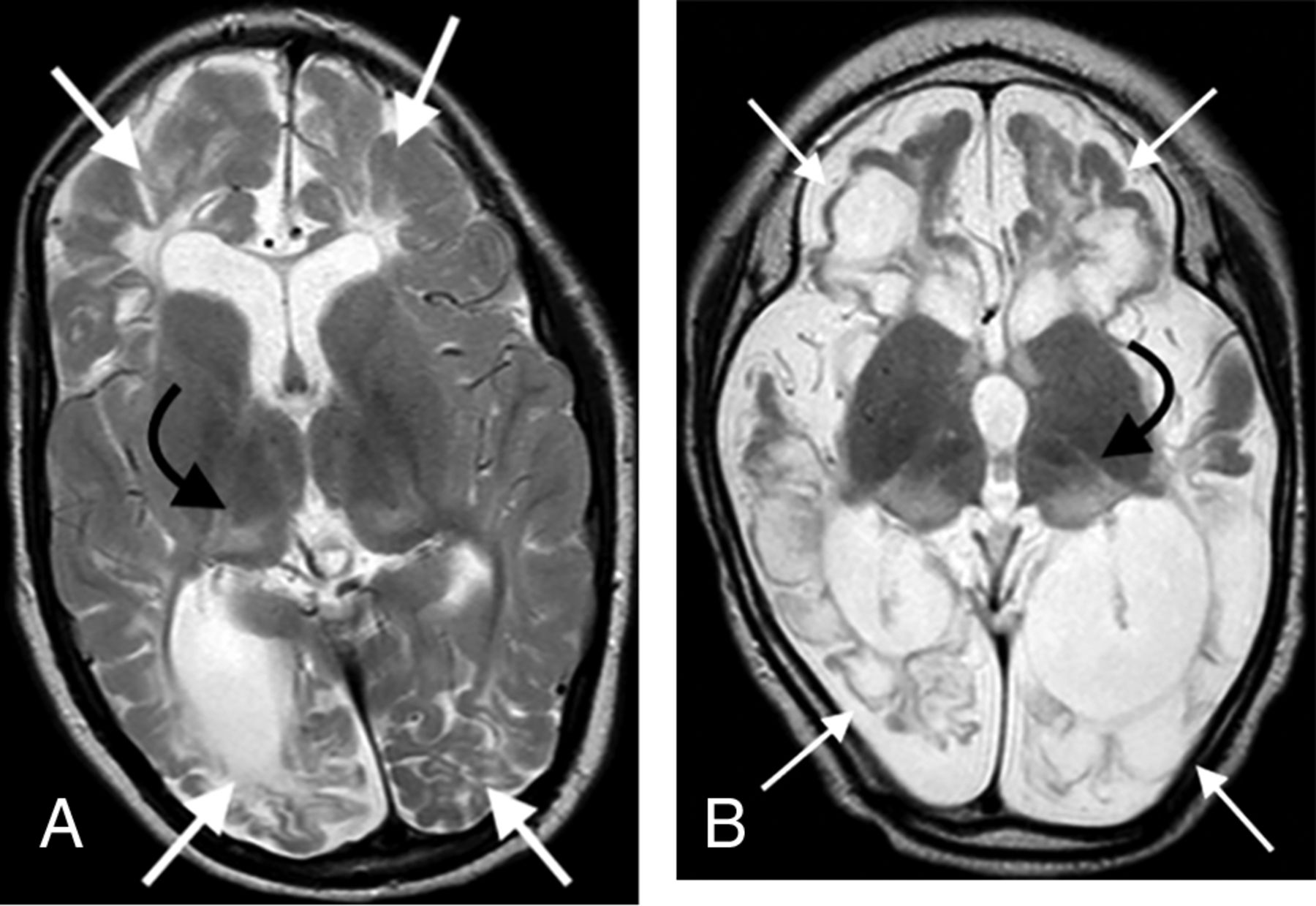
- FIG 3.
Axial T2-weighted images in 2 children with proved neonatal hypoglycemia. There is bilateral occipital lobe encephalomalacia (arrows) related to hypoglycemic brain injury. Note the absence of any thalamic injury.
- FIG 4.
Combined hypoxic-ischemic and hypoglycemic brain injury in 2 children with documented neonatal encephalopathy. Note the exaggerated signal abnormality and thalamic volume loss (black arrows). There are multiple watershed areas (white arrows) demonstrating encephalomalacia change.
- FIG 5.
The key thalamic nuclei identified as components of the thalamus L-sign (dotted line) include the pulvinar, the lateral geniculate nucleus, and the reticular formation nuclei. Illustration by Neil Northey.





Tables
Lobe/Structure Features Subtype 1 Subtype 2 Subtype 3 Subtype 4 Subtype 5 Subtype 6 Subtype 7 Overall Anterior (n = 10) Peri-Sylvian (n = 1) Posterior (n = 1) Anterior + Peri-Sylvian (n = 6) Peri-Sylvian + Posterior (n = 15) Anterior + Posterior (n = 7) All 3 Zones (n = 59) (n = 99) Thalamic injury location (No.) (%) Nil 1 (16.7) 3 (30.0) 4 (4.0) Atypical 2 (33.3) 7 (70.0) 1 (14.3) 10 (10.1) Thalamus L-sign 1 (100.0) 1 (100.0) 3 (50.0) 15 (100.0) 6 (85.7) 59 (100.0) 85 (85.9) Thalamus score (No.) (%) Not/less involved 1 (100.0) 1 (100.0) 6 (100.0) 14 (93.9) 10 (100.0) 6 (85.7) 53 (89.8) 91 (91.9) Markedly destroyed 1 (6.7) 1 (14.3) 6 (10.2) 8 (8.1) Parietal (No.) (%) Not involved 3 (50.0) 6 (60.0) 1 (14.3) 10 (10.1) Involved 1 (100.0) 1 (100.0) 3 (50.0) 15 (100.0) 4 (40.0) 6 (85.7) 59 (100.0) 89 (89.9) Occipital (No.) (%) Not involved 1 (100.0) 7 (70.0) 8 (8.1) Involved 1 (100.0) 6 (100.0) 15 (100.0) 3 (30.0) 7 (100.0) 59 (100.0) 91 (91.9) Frontal (No.) (%) Not involved 1 (100.0) 8 (53.3) 1 (10.0) 1 (1.7) 11 (11.1) Involved 1 (100.0) 6 (100.0) 7 (46.7) 9 (90.0) 7 (100.0) 58 (98.3) 88 (88.9) Temporal (No.) (%) Not involved 3 (20.0) 6 (60.0) 3 (42.9) 3 (5.1) 15 (15.2) Involved 1 (100.0) 1 (100.0) 6 (100.0) 12 (80.0) 4 (40.0) 4 (57.1) 56 (94.9) 84 (84.8) Cerebellum (No.) (%) Not involved 1 (100.0) 4 (66.7) 10 (66.7) 7 (70.0) 5 (71.4) 40 (67.8) 67 (67.7) Involved 1 (100.0) 2 (33.3) 5 (33.3) 3 (30.0) 2 (28.6) 19 (32.2) 32 (32.3) Brainstem (No.) (%) Not involved 1 (100.0) 1 (100.0) 6 (100.0) 14 (93.3) 10 (100.0) 7 (100.0) 49 (83.1) 88 (88.9) Involved 1 (6.7) 10 (16.9) 11 (11.1) - Table 2:
Key features involved in thalamus L-sign injury compared with other thalamic injuries (nil and atypical)
Lobe/Structure Features Thalamus L-Sign (n = 85) Other (n = 14) Overall (n = 99) P Value Thalamus score (No.) (%) Not/less involved 77 (90.6) 14 (100.0) 91 (91.9) <.001 Markedly destroyed 8 (9.4) Parietal (No.) (%) Not involved 3 (3.5) 7 (50.0) 10 (10.1) <.001 Involved 82 (96.5) 7 (50.0) 89 (89.9) Occipital (No.) (%) Not involved 1 (1.2) 7 (50.0) 8 (8.1) <.001 Involved 84 (98.8) 7 (50.0) 91 (91.9) Frontal (No.) (%) Not involved 10 (11.8) 1 (7.1) 11 (11.1) 1.000 Involved 75 (88.2) 13 (92.9) 88 (88.9) Temporal (No.) (%) Not involved 9 (10.6) 6 (42.9) 15 (15.2) .007 Involved 76 (89.4) 8 (57.1) 84 (84.8) Cerebellum (No.) (%) Not involved 57 (67.1) 10 (71.4) 67 (67.7) 1.000 Involved 28 (32.9) 4 (28.6) 32 (32.3) Brainstem (No.) (%) Not involved 74 (87.1) 14 (100.0) 88 (88.9) .355 Involved 11 (12.9) 11 (11.1) Lobe/Structure RR 95% CI P Value Parietal 3.07 1.19−7.93 .020 Occipital 7.38 1.18−46.23 .033 Frontal 0.94 0.76−1.15 .539 Temporal 1.51 0.99−2.29 .055 Cerebellum 1.03 0.87−1.21 .738 Brainstem 1.19 1.09−1.30 <.001 Parietal + occipital 2.79 1.25−6.23 .012 Note:—RR indicates relative risk.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.