
Abstract
BACKGROUND AND PURPOSE: Several CT findings are thought to be indicative of vocal cord paralysis; however, these signs have never been validated in a blinded fashion. This study attempts to compare and validate these signs and determine their accuracy in predicting vocal cord paralysis.
MATERIALS AND METHODS: A retrospective chart review was performed, and CT scans from patients with known unilateral vocal cord paralysis and known normal vocal cord movement were reviewed by 3 radiologists who were blinded to the status of the patients’ laryngeal function. The scans were reviewed and scored for 8 accepted signs of vocal cord paralysis as well as for predicting a final diagnostic conclusion. Statistical analysis using odds ratios for signs and the Fleiss κ for criterion agreement among the radiologists was performed for diagnostic accuracy.
RESULTS: The presence of medial displacement of the posterior ipsilateral vocal fold margin and ipsilateral laryngeal ventricular dilation yielded the greatest positive predictive value. Other signs demonstrated high specificity, but interrater discrepancy was greater than expected and diminished the reliability of these signs in predicting vocal cord paralysis. Overall, sensitivity and negative predictive values were low.
CONCLUSIONS: Predicting vocal cord paralysis on the basis of CT findings is not as accurate or straightforward in prospectively predicting vocal cord paralysis as implied in prior studies.
ABBREVIATION:
- UVFP
- unilateral vocal fold paralysis
Unilateral vocal fold paralysis (UVFP) is a relatively common disease process frequently seen by otolaryngologists. A definitive diagnosis of UVFP is dependent on visualization of the glottis; therefore, the exact incidence is not known.1 Patients with UVFP most commonly present with dysphonia, dyspnea, and dysphagia, all of which may be sudden or gradual in onset.2 This disease process develops as a result of injury to the vagus nerve or recurrent laryngeal nerve, a branch of the vagus nerve. Up to 40% of cases are idiopathic.3 UVFP can result from an injury at any point along the nerve as it courses from the jugular foramen to the mediastinum, around the subclavian artery on the right or the aortic arch on the left, and finally through the tracheoesophageal grooves before entering the larynx at the cricothyroid joint.
There are a variety of etiologies of UVFP, with iatrogenic injury historically being the leading cause, followed by malignancy and idiopathic, neuropathy, trauma, and inflammatory etiologies.4 In the absence of a history of a neck or cervical spinal operation, laryngeal trauma, or known malignancy, the standard diagnostic work-up includes CT from the skull base through the mediastinum to assess a lesion along the course of the nerve. Although cord palsy is often diagnosed clinically, up to 30% of cases may be asymptomatic and clinically unsuspected.5 There are many imaging signs to suggest vocal cord paralysis with varying degrees of sensitivity and specificity (Table 1).4⇓⇓-7 Representative examples of these signs are presented in Fig 1. Of note, the 3 most specific signs of cord palsy reported in the literature include dilation of the laryngeal ventricle, medial deviation and thickening of the aryepiglottic fold, and dilation of the piriform sinus.6

CT findings of UVFP images from 2 patients with proven left UVFP. A, Coronal CT image demonstrates dilation of the left laryngeal ventricle (star) and loss of the subglottic arch (arrow). B, Axial CT image demonstrates medial positioning of the left posterior vocal fold margin (arrow). C, Axial CT image demonstrates anterior positioning of the left arytenoid cartilage (arrow). D, Axial CT image demonstrates rotation and thickening of the left aryepiglottic fold and enlargement of the left pyriform sinus (star). E, Axial CT image demonstrates the mushroom sign, tilting toward the left (star).
CT signs of UVFP as previously described4-7
Although laryngoscopic evaluation by an otolaryngologist remains the criterion standard to establish the definitive diagnosis of vocal cord paralysis, the presence of these signs noted incidentally on CT may cause the interpreting radiologist to question vocal cord paralysis in examinations ordered for other indications. This issue may result in significant expense, psychological stress, and physical discomfort for the patient in obtaining a definitive diagnosis through evaluation by an otolaryngologist. To our knowledge, all previous studies have evaluated the usefulness of CT signs (Table 1) in patients with a known, laryngoscopically-established diagnosis of vocal cord paralysis. This article tests the utility of these signs by blinding the interpreting radiologists to randomized CT scans of patients with and without UVFP. Thus, we attempted to identify the most useful signs for prospectively raising concern for UVFP.
MATERIALS AND METHODS
Patient Characteristics and Study Setting
A retrospective chart review of patients from Loyola University Medical Center in Maywood, Illinois between 2009 and 2019 was performed on 2 groups of patients. One group consisted of patients diagnosed with unilateral vocal cord paralysis with a confirmatory laryngoscopy performed by an attending otolaryngologist <3 months before a CT neck soft-tissue examination. Only patients with complete, unilateral vocal cord paralysis were included; patients with hypomobile vocal fold movement or bilateral vocal cord paralysis were not included. The other group consisted of patients with normal vocal cord movement, which was also confirmed on laryngoscopy by an attending otolaryngologist <3 months before a CT neck soft-tissue examination. Of note, neck CTs were performed at many institutions, given the nature of our tertiary center, and followed various protocols, but included examinations were performed with ≤3-mm section thickness, and coronal and sagittal reformats were also available.
Patients were excluded from the study if they had any of the following: prior radiation therapy to the neck, laryngeal/pharyngeal cancer, a history of laryngeal/pharyngeal trauma, a history of a laryngeal/pharyngeal operation, and intubation or a tracheostomy tube at the time of imaging. CT scans were evaluated by 3 radiologists, including 2 neuroradiologists with Certificates of Added Qualification with 5 and 22 years’ experience, respectively, and 1 neuroradiology fellow. All 3 were blinded as to in which group the patient belonged. Radiologists indicated the presence and absence of each of the 8 UVFP signs as described in Table 1: 1) dilation of the ipsilateral pyriform sinus, 2) medial rotation of the ipsilateral aryepiglottic fold, 3) thickening of the ipsilateral aryepiglottic fold, 4) dilation of the ipsilateral laryngeal ventricle, 5) medial displacement of the posterior aspect of the ipsilateral true vocal fold, 6) the mushroom sign, 7) anterior displacement of the ipsilateral arytenoid cartilage, and 8) loss of the subglottic arch. The 3 radiologists met to review and discuss how to evaluate the various CT signs before the study initiation. Differences in the assessment of the presence of a criterion were resolved via consensus of the radiologists. The final radiologic diagnosis of vocal cord paralysis was based on majority consensus.
Statistical Analysis
Patient demographics were presented overall and stratified by an otolaryngologist’s diagnosis of UVFP based on the laryngoscopic examination (reference standard). Variables were compared between those with and without UVFP on the basis of the laryngoscopic examination using a t test for age and a χ2 test for sex. CT scan criterion agreement among the 3 raters was assessed using the Fleiss κ. Data were summarized for each patient to determine the CT findings by a majority of radiologists, and odds ratios were estimated for the CT finding associated with the reference standard for UVFP. Measures of diagnostic accuracy (sensitivity, specificity, positive predictive value, and negative predictive value) were used as a part of the analytic approach. Combinations of CT findings were considered using best subsets logistic regression, and candidate models were compared using likelihood ratios tests. For the final chosen model, goodness of fit was assessed, and adjusted odds ratios were presented for CT findings associated with UVFP. Analyses were performed using SAS, Version 9.4 (SAS Institute).
RESULTS
A total of 147 patients met the inclusion criteria for this retrospective study. Four of these patients could not be evaluated due to the breath-hold examination (n = 2) and motion (n = 2). Therefore, a total of 143 patients could be analyzed. The mean age was 63 (SD, 15) years, and half were women (n = 72, 50.3%). Those with vocal cord paralysis were older (66 [SD, 14] years versus 56 [SD, 15] years, P < .001), and most had paralysis on the left (n = 76, 73.1%) (Table 2).
Patient characteristics by true UVFP status
Agreement between raters was highest for findings of ipsilateral pyriform dilation (κ = 0.77; 95% CI, 0.68–0.86) and the aryepiglottic fold medial and rotated (κ = 0.66; 95% CI, 0.56–0.75), followed by medial displacement of the postipsilateral cord margin (κ = 0.54; 95% CI, 0.42–0.65), ipsilateral laryngeal ventricle dilation (κ = 0.50; 95% CI, 0.39–0.61), and anteromedial displacement of the ipsilateral arytenoid cartilage (κ = 0.46; 95% CI, 0.34–0.57). Agreement was poor-to-fair for less frequently detected findings, including aryepiglottic fold thickening (κ = 0.32), the mushroom sign (κ = 0.19), and subglottic arch loss (κ = 0.15). The final diagnosis of UVFP had moderate agreement (κ = 0.58; 95% CI, 0.48–0.69) (Table 3).
Agreement of radiologic diagnoses
The sensitivity and specificity of the imaging criteria were evaluated on the basis of consensus of radiologists. The criteria with the highest levels of sensitivity included medial displacement of the posterior margin of the ipsilateral vocal fold (78.8%), dilation of the ipsilateral laryngeal ventricle (69.2%), and dilation of the ipsilateral pyriform sinus (68.3%). The 3 signs with the highest degree of specificity also demonstrated higher positive predictive values: mushroom sign (97.4%), loss of the subglottic arch (97.4%), and thickening of the ipsilateral aryepiglottic fold (94.9%), and anteromedial displacement of the ipsilateral arytenoid cartilage (89.7%). The negative predictive value was low across all signs. When the radiologists were asked to make a final diagnosis of UVFP based on all radiographic findings, the final diagnosis had a sensitivity of 68.0% (70/103) in detecting a UVFP and a specificity of 64.1% (25/39), with a positive predictive value of 83.3% (70/84) (presented in Tables 4 and 5, respectively).
Radiologic diagnoses to predict vocal cord paralysis
Radiologist-versus-otolaryngologist diagnosis of vocal cord paralysis
A 2-variable model that included medial displacement of the postipsilateral cord margin and ipsilateral laryngeal ventricle dilation was identified as an improvement over univariable models and the acceptable goodness of fit (χ2 = 0.26, P = .62). Models with additional parameters did not show statistically significant improvement. On the basis of this model, the odds of UVFP were higher for those with medial displacement of the postipsilateral cord margin (adjusted OR = 3.09; 95% CI, 1.32–7.24) and with ipsilateral laryngeal ventricle dilation (adjusted OR = 2.40; 95% CI, 1.03–5.55) (Table 6). Based on the presence of either finding, this model provides a combined sensitivity and specificity of 86.5% and 41.0%, respectively. The presence of both findings demonstrates 61.5% sensitivity and 74.4% specificity (Table 7).
Model to predict vocal cord paralysis from radiology findings
Predictive value by combination of positive radiology findings
DISCUSSION
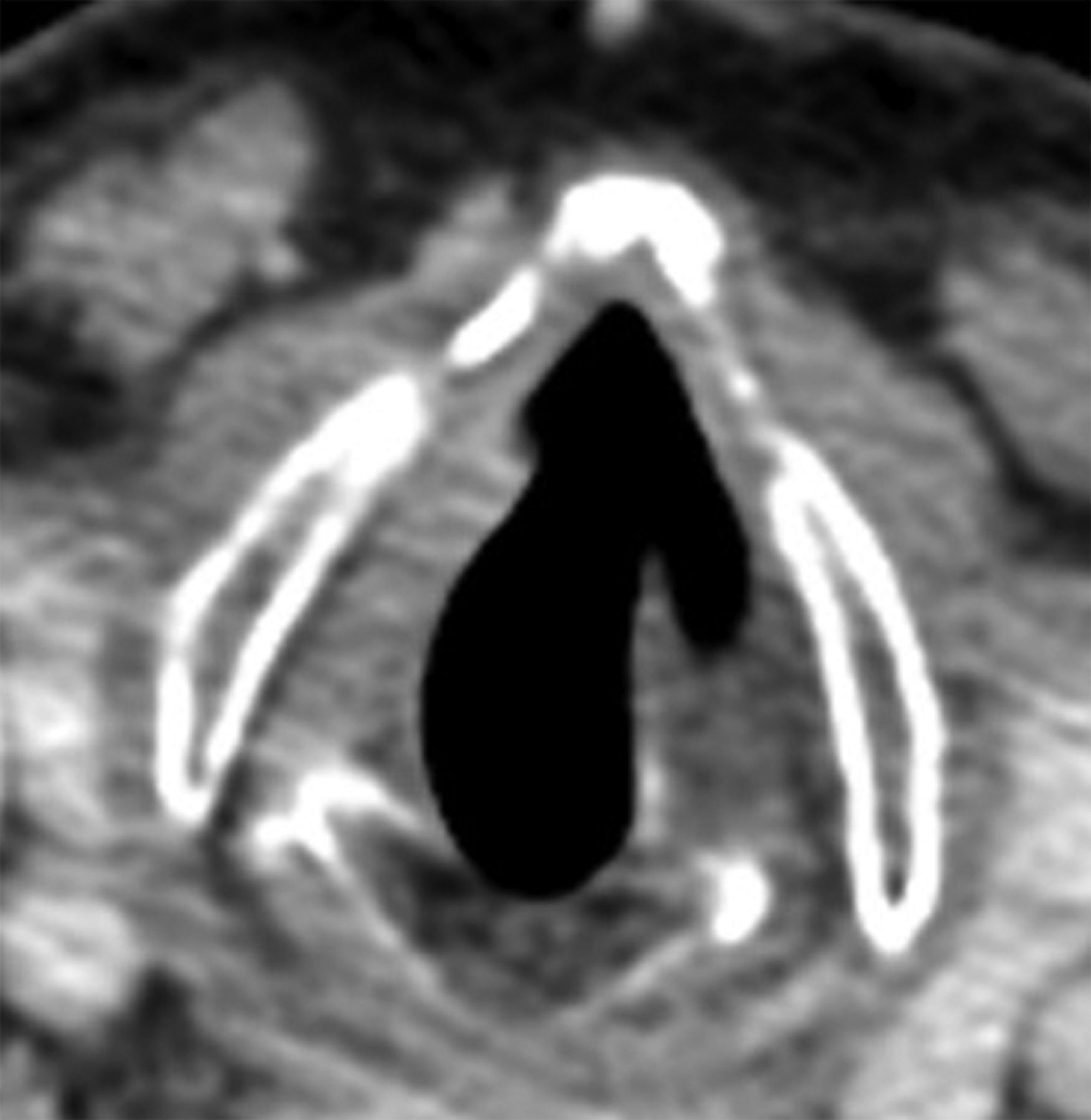
This is the first study to help identify UVFP on CT prospectively, using signs established as helpful in prior studies.4⇓⇓-7 As shown in our study, agreement among the radiologists was not as high as expected, suggesting a subjectivity in the evaluation based on varying thresholds. The surprising lack of objectivity of the various other signs diminishes their usefulness in prospectively predicting vocal cord paralysis. For example, although the mushroom sign and the loss of the subglottic arch sign were the most specific, they were also rated the lowest in the radiologists’ agreement. Their poor interrater reliability minimizes their usefulness (Fig 2).

Radiologists’ subjectivity on a single axial postcontrast CT scan demonstrates questionable findings of the mushroom sign. This was read by 2 radiologists as negative for this sign and by 1 radiologist as positive for the sign with the left side as the affected side. By laryngoscopic examination, this patient did indeed have left-sided vocal fold paralysis.
In our study, the presence of medial displacement of the posterior ipsilateral vocal fold margin and ipsilateral laryngeal ventricular dilation combined yielded a positive predictive value of 87% and a specificity of 74%. These signs also had good agreement among the interpreting neuroradiologists, which is important if these signs are to be used to raise concern for UVFP and thus initiate further evaluation by an otolaryngologist. Most interesting, our findings are somewhat different from those in the study of Chin et al,6 in which the authors retrospectively evaluated 40 patients with the knowledge of UVCP (but did not know the laterality). While they found dilation of the laryngeal ventricle to be a very useful sign, they also found medial deviation and thickening of the aryepiglottic fold as well as dilation of the piriform sinus to be as helpful. These latter 2 signs were also helpful in our study but did not reach statistical significance.
Our study demonstrates that it is much less straightforward to prospectively raise concern for UVFP compared with interpreting examinations when a laryngoscopic diagnosis of UVFP is confirmed. If medial displacement of the posterior ipsilateral vocal fold margin and ipsilateral laryngeal ventricular dilation are present, concern should be raised for UVFP prospectively and a thorough evaluation of the course of the vagus and recurrent laryngeal nerves from the skull base through the mediastinum should be performed on the available neck CT examination. Mimics of UVFP should also be excluded when possible.4
Limitations to our study include uneven distribution of patients with UVFP versus healthy controls, excluding patients with bilateral vocal cord paralysis, and agreement between neuroradiologists. Despite meeting beforehand to discuss how to evaluate the various CT signs, discerning the presence or absence of some signs proved subjective in this study, largely due to varying thresholds for calling the presence of a sign for each neuroradiologist based on their own experience. Imaging findings of a high vagal nerve palsy were not included in our study. Additional, albeit less common, signs of UVFP such as subglottic fullness and a widened vallecula5 were also not included in our study.
CONCLUSIONS
It is not as accurate or straightforward to prospectively predict vocal cord paralysis based on CT findings as previously implied in prior studies. CT scan sensitivity and negative predictive value are low for vocal cord paralysis. Because the implied diagnosis of vocal cord paralysis necessitates further work-up, expense, and procedures, care must be taken to translate suspicious findings appropriately.
References
- Received May 3, 2021.
- Accepted after revision January 8, 2022.
- © 2022 by American Journal of Neuroradiology




{kind=link}
{kind=link}