
Abstract
BACKGROUND AND PURPOSE: Venous pulsatile tinnitus is a disabling condition mainly caused by a stenosis of the lateral sinus. Here, we aimed to report a novel cause of venous pulsatile tinnitus, stenosis of the marginal sinus.
MATERIALS AND METHODS: We retrospectively analyzed patients with isolated venous pulsatile tinnitus for which the suspected cause was a stenosis of the marginal sinus, treated or not, between January 2017 and December 2020. Patient charts and imaging were systematically reviewed. All patients underwent noncontrast temporal bone CT and MR imaging.
RESULTS: Eight patients (7 women; median age, 36 years) were included. Six patients (75%) were overweight, and 1 patient had idiopathic intracranial hypertension. All patients presented with a typical venous pulsatile tinnitus. The stenosis of the marginal sinus was detected using oblique reconstructions on postcontrast 3D MR imaging. There was no other pathologic finding except ipsilateral stenosis of the lateral sinus in 3 patients. Four patients underwent endovascular therapy with placement of a stent in the marginal sinus, leading to complete resolution of the pulsatile tinnitus for all of them. No complication occurred. Of note, the symptoms of intracranial hypertension also regressed after stent placement in that patient.
CONCLUSIONS: Marginal sinus stenosis is a novel cause of venous pulsatile tinnitus, which can be easily detected on MR imaging. Marginal sinus stent placement is safe and efficient. We hypothesized that the marginal sinus stenosis pathophysiology is similar to that of lateral sinus stenosis, which is a common and well-known cause of venous pulsatile tinnitus, explaining the similar clinical presentation and endovascular management.
ABBREVIATIONS:
- IIH
- idiopathic intracranial hypertension
- LS
- lateral sinus
- MS
- marginal sinus
- OS
- occipital sinus
- PT
- pulsatile tinnitus
- SSS
- superior sagittal sinus
- VAS
- visual analog scale
Pulsatile tinnitus (PT) is an uncommon-but-disabling symptom, which has numerous causes, both vascular and nonvascular.1 Venous etiologies of PT are suspected when the tinnitus disappears by compressing the ipsilateral internal jugular vein. Venous etiologies of PT are increasingly reported and are related to venous abnormalities like lateral sinus (LS) stenosis,2 sigmoid sinus diverticulum,3,4 dehiscence,5 or a mastoid emissary vein.6 It is paramount to recognize such anomalies because they are often manageable by endovascular treatment.2,3,6
Here, we report the clinical and radiographic features as well as the therapeutic management of patients with PT caused by a stenosis of the marginal sinus (MS).
MATERIALS AND METHODS
Study Design
This is a single-center retrospective study. Consecutive patients between January 2017 and December 2020 with diagnosed PT caused by a stenosis of the MS were included. The medical charts of included patients were analyzed to evaluate patient backgrounds, clinical symptoms, treatment modalities, and clinical outcomes.
Tinnitus was defined as pulsatile when the patient described a sound synchronous with the heart rate. All patients underwent a complete clinical examination by our senior author (E.H.), including auscultation of the heart, neck, and the head, and vascular compression maneuvers at the neck. Disability was evaluated on a visual analog scale (VAS) from 0 (no disability) to 10 (unbearable and extreme disability).
On the basis of the clinical examination, PT was classified as venous if the sound disappeared or decreased during compression of the ipsilateral internal jugular vein and as arterial if the sound disappeared or decreased during compression of the ipsilateral carotid artery. If the vascular compression maneuvers had no effect on the intensity of the PT, it was classified as neutral.6,7
Imaging Protocol and Analysis
All patients underwent MR imaging examinations (3T, Magnetom Skyra; Siemens), which included the following sequences: 3D-TOF from the vertex to the foramen magnum (TR = 1470 ms, TE = 310 ms, 384 × 345, flip angle = 120°, number of excitations = 2, generalized autocalibrating partially parallel acquisition = 2, scan time = 5 minutes 6 seconds); a postcontrast (gadobutrol, Gadovist; Bayer Schering Pharma; 0.1 mL/kg) 3D T1 gradient-echo sequence (MPRAGE; TR = 1470 ms, TE = 310 ms, 384 × 345, flip angle = 120°, number of excitations = 2, generalized autocalibrating partially parallel acquisition = 2, scan time = 5 minutes 6 seconds); and high-resolution temporal bone CT (section thickness = 0.6 mm, 350 mAs, 140 kV(peak) per section) (Somatom Sensation; Siemens).
Imaging was reviewed by 2 experienced neuroradiologists. High-resolution temporal bone and MR images were analyzed to identify potential causes for PT. The MS and the occipital sinus (OS) are not usually visible on postcontrast MR imaging, except if they are enlarged.8 When the MS was enlarged on the side of the PT, oblique reconstructions from the postcontrast 3D T1 gradient-echo sequence aligning the superior sagittal sinus (SSS) with the OS and the MS were used to detect a stenosis. The ipsilateral LS was also evaluated as normal or hypoplastic and with or without stenosis if normal.9
Endovascular Procedure and Follow-up
If the patient’s symptom was >5/10 on the VAS, a treatment was proposed, and informed written consent was obtained before treatment. All procedures were performed with the patients under general anesthesia and heparinization (50-IU/kg intravenous bolus followed by 500 IU/h). Briefly, biplanar angiography (Artis zee Q; Siemens) was performed through femoral arterial access with a 4F catheter (Cordis). Jugular puncture was performed under roadmap guidance, and an 8F sheath was placed. Distal access was obtained using Neuron MAX 088 (Penumbra) and Sofia 6F 125-cm catheters (MicroVention). The MS was then catheterized to the jugular bulb via the LS and the OS using a Traxcess-14 microwire (MicroVention) to navigate a 21-inch Prowler Select Plus microcatheter (Codman & Shurtleff).
Then, a 0.014-inch Doppler velocity ComboWire in combination with ComboMap matching hardware (Volcano) was used to measure Doppler velocity at the level of the stenosis in the MS (velocity signals were recorded at 200 Hz).10 The results were expressed in centimeters per second. The acceleration of the blood velocity at the level of the stenosis was expressed as a velocity ratio (blood velocity at the stenosis/blood velocity in the OS). In our center, the velocity measurements are systematically performed before stent placement in case of PT because we believe that there is a correlation between blood flow velocity and the patient’s symptoms.10,11
If the blood acceleration was confirmed (velocity ratio > 2), a 5× 30 mm Carotid Wallstent (Boston Scientific) was deployed covering the stenosis and the MS. Because it was a new entity, a 7 × 50 mm Carotid Wallstent was used in the LS if a stenosis was noted. Heparinization was discontinued, and patients were allowed to recover for 24 hours before discharge if no complication was observed. Before stent placement, patients were given aspirin, 75 mg, and clopidogrel, 75 mg, daily for a week. Patients were tested for clopidogrel resistance, and if the patient was resistant, clopidogrel was switched to prasugrel (10 mg). Oral medication was continued for 3 months after the stent placement, followed by aspirin alone for 9 additional months.
Patients were clinically examined at 3 months and 1 year, and a venous contrast-enhanced CT was systematically performed to confirm the absence of stent thrombosis.
RESULTS
Patient Characteristics
A total of 8 patients were included (7 women and 1 man; median age, 36 years; range, 14–60 years). The median body mass index was 29.5 (range, 18–44), with 6 patients overweight (body mass index > 25), including 4 patients who were obese (body mass index = 30). No other significant comorbidities were found.
The PT was located more frequently on the right side (5 patients, 63%) and was systematically classified as a typical venous PT (100%). PT was responsible for a major disability (VAS > 5) in 5 patients (63%). Of note, 1 patient had associated headache and papilledema due to idiopathic intracranial hypertension (IIH).
Imaging Data
All 8 patients presented with a dilated MS ipsilateral to the PT associated with an extrinsic stenosis on the segment preceding the junction with the jugular bulb. The enlarged MS was unilateral or bilateral but was always preceded by an enlarged OS. The oblique reconstruction on the postcontrast MR imaging clearly depicted the stenosis in each patient (Figs 1–3). We noted different configurations of the LS: normal caliber with a stenosis in 3 patients, normal caliber without stenosis in 2 patients, and hypoplastic in the remaining 3 patients. All other causes of PT (including dural arteriovenous fistula and sigmoid sinus diverticulum) were eliminated after initial MR imaging and CT explorations.

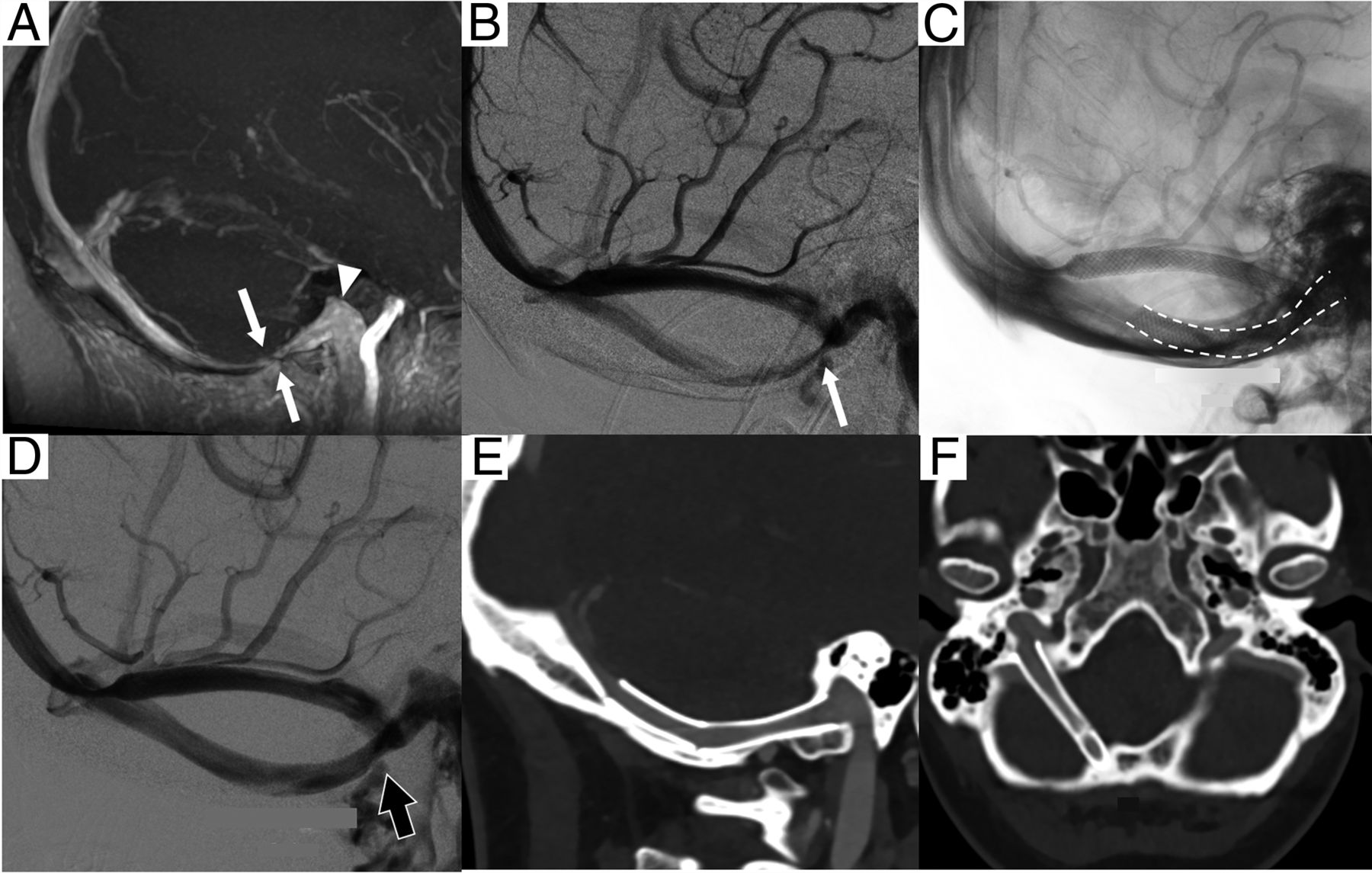
A patient presented with a right-sided venous PT. The patient initially underwent stenting of the lateral sinus, which was unsuccessful because the tinnitus was not modified. A, An oblique 3D contrast-enhanced T1 sequence depicts a stenosis (white arrows) of the right MS before joining the jugular bulb (white arrowhead). B, A lateral angiogram confirms the stenosis (white arrow). C and D, Two 5 ×30 mm Carotid Wallstents were placed in the MS (dashed white line), lifting the stenosis and restoring a normal laminar flow (black arrow). The patient’s tinnitus was completely cured after the procedure. E and F, In the control venous CTA at 3 months, oblique and axial reconstructions, no thrombosis is depicted. Note that the stent is in the jugular bulb, close to the temporal bone and the jugular foramen.

The patient presented with a right-sided venous PT. A, An oblique 3D contrast-enhanced T1 sequence depicts a stenosis (white arrows) of the right MS (white arrow). Lateral angiogram (B) and oblique phlebography (C) confirm the extrinsic stenosis of the MS (white arrow); an intrinsic stenosis of the LS was also depicted (black arrowhead). Doppler measurement of the venous flow using a ComboWire confirmed the accelerated blood flow at the level of the MS stenosis. D, Oblique phlebography shows the deployment of the 5 ×30 mm Carotid Wallstent in the MS after placement of a first stent in the LS. E and F, Stents were placed in the MS and LS (white arrowheads), lifting the stenosis and restoring a normal laminar flow (black arrow). The patient’s tinnitus was completely cured after the procedure. Jug indicates jugular vein.

A patient presented with a right-sided venous PT associated with symptoms of IIH. A, An oblique 3D contrast-enhanced T1 sequence depicts a stenosis (white arrows) of the right MS; no MS was noted on the left side. B, Oblique phlebography confirms the extrinsic stenosis of the MS (white arrow); the LS was normal on the right side and absent (hypoplastic) on the left side. C, Two 5 × 30 mm Carotid Wallstents are deployed in the right occipital-marginal sinus (white arrowheads) (D), lifting the stenosis and restoring a normal MS caliber. Both the tinnitus and the symptoms of IIH disappeared. Jug indicates jugular vein.
Endovascular Treatment
Of the 5 patients with a significant disability, 4 patients accepted the treatment (Table). In all 4 patients, stenting the MS permitted the complete resolution of the PT (VAS = 0). Patients 3 and 4 underwent stenting of both the MS and LS during the same procedure (in 1 case, LS stent placement followed the MS stent placement, whereas it was in the opposite order for the other case) (Fig 2). For patient 1, only the LS was stented during the first procedure (at the time, MS stenosis was not a suspected cause for PT), resulting in no modification of the PT immediately after the operation and at the 3-month follow-up. The second analysis of the MR imaging and an angiogram led to a proposal of a second intervention with stenting of the MS, which the patient accepted. This time the PT completely resolved after the procedure and remained healed at the 3-month and 1-year follow-ups (Fig 1).
Patients with MS stenosis
There was no technical limitation. The 5-mm-caliber stent was chosen because it corresponded to the caliber of the normal MS in all 4 patients. The stent was deployed starting at the junction between the MS and the jugular bulb, then over the stenosis in the MS. In 2 cases, a second 5 × 30 mm stent was used because of an acute angle formed between the distal part of the stent and the MS at the vertical junction with the OS segment. In these cases, the stent would extend to the OS (Fig 3).
Blood velocities were obtained for 3 patients (all except patient 1); the velocity ratio was an average of 4 (range, 3–5) with mean blood velocities of 10 cm/s (range, 9–11 cm/s ) at the level of the OS and at 38 cm/s at the level of the stenosis. For patients with LS stent placement during the same procedure, the velocity ratio in the LS was inferior in one case (2 versus 5 in the MS) and superior in the other case (5 versus 3 in the MS).
Follow-up
All patients treated remained free of PT (VAS = 0) at follow-up, and no complication was detected on physical or imaging evaluation. Furthermore, the patient with IIH was also improved after the stent placement, and papilledema resolved at the 1-year control.
DISCUSSION
In this study, we described 8 patients with venous PT, in whom the suspected cause was an MS stenosis. Four patients underwent stenting of the MS. The procedure was effective for all of them. To the best of our knowledge, this is the largest case series that highlights specifically the stenosis of the MS as a cause of PT. Preceding reports have described MS stenosis as a cause for venous PT12 or IIH.13,14 However, Li et al12 referred to it as a stenosis of the vein of the hypoglossal canal. We believe it is an inaccurate name because the sinus is reaching the jugular bulb without crossing the hypoglossal canal.
The MS is a dural venous sinus that connects the OS posteriorly and the basilar venous plexus and the distal part of the sigmoid sinus at the junction with the internal jugular bulb anteriorly. Generally, in human adults, the LS represents the main venous outflow, and the occipital-marginal sinus system, an alternative pathway. The dominance of LS over the occipital-marginal sinus system is believed to be an epigenetic adaptation acquired with bipedalism in early human species.15 During fetal growth, the OS and the MS develop simultaneously from a large plexiform configuration, and by full term, both tend to have regressed to a small accessory sinus.16 However, the occipital-marginal sinus system can be found enlarged or even dominant over the LS in approximately 4%–5% of the population.17
Here, we show that the MS is another potential location for dural venous sinus stenosis. MS stenosis clinical and imaging presentations were very similar to those of LS stenosis: Patients were predominantly overweight women with typical venous PT, and the stenosis could be identified on MR images. In our center, MR imaging with a postcontrast 3D T1 gradient-echo sequence is part of the initial exploration of PT. MS stenosis can be suspected when an enlarged OS (usually as large as the SSS) followed by an enlarged MS (ipsilateral to the PT) is present. Oblique 3D reconstructions aligning the SSS with the OS, the MS, and the jugular bulb were useful for easily detecting the stenosis.
The perception of a venous PT is linked to the turbulence of the blood flow following the venous stenosis, as described with the LS.10,11,18 Because the MS has a close relationship with the temporal bone, we hypothesized that the same pathophysiology is responsible for the PT in MS stenosis. Therefore, relieving the stenosis with a stent permitted the return of a laminar blood flow in the MS, and, thus, PT disappearance.2,19
In 1 patient, an MS stenosis was also responsible for IIH (Fig 3). Most interesting, the ipsilateral LS was present with a normal caliber (the contralateral LS was hypoplastic). All symptoms improved after the stenting of the MS, meaning that the right lateral sinus was not sufficient for a normal cerebral blood circulation and the patient was dependent on the MS as well. LS stenosis is often associated with IIH, and stenting of the LS is safe and effective.9,20 Two recent case reports of MS stenosis associated with IIH described clinical improvement after stenting of the sinus, supporting LS and MS stenosis being similar pathologies.13,14
Finally, 2 patients were treated for LS and MS stenoses during the same procedure, interpreted as a limitation of our results (because the responsibility of the MS stenosis is uncertain). However, performing 2 different interventions to test which stenosis was responsible for the PT was, in our opinion, not feasible outside a prospective clinical trial. In addition, the acceleration of the venous flow at the MS stenosis was confirmed by measurement of blood velocity before stent placement. We observed an acceleration ratio similar to the one reported for the LS (median velocity ratio of the SSS/LS stenosis, 3 [range, 2–7]).10 It is also common to find multiple causes of venous PT, like LS stenosis and sigmoid sinus ectasia.19,21 Moreover, in patient 1, we postponed the MS stent placement, limiting the treatment of the LS. The patient’s PT remained unchanged after the first procedure but was completely cured after the second procedure (stenting of the MS), emphasizing the role of the MS. Also, 4 patients were not treated, meaning that the responsibility of the MS stenosis remains untested for them as well. Nevertheless, all 4 patients had typical venous PT, and no other pathologic findings were detected on CT or MR imaging (including LS stenosis).
This study has several diagnostic and therapeutic implications. First, an MS stenosis should be looked for on a MRI done for the exploration of a venous PT (using the 3D oblique reconstruction if the OS is enlarged); and even if a stenosis of the LS is present as both (the MS and the LS) could contribute to the tinnitus. Second, treatment of the MS stenosis via stent placement is feasible and safe, as the large experience with LS stent placement could predict.
This study also has limitations. It is a retrospective study performed at a single academic center. The usual pressure measurements were not systematically performed or available and, therefore, are not reported here, though possibly being valuable information. Instead, we reported venous blood flow velocities, which limit the comparison with other studies. Finally, when both stenoses are present (MS and LS), it remains to determine which one is more “symptomatic” and whether they should be treated together.
CONCLUSIONS
In this study, we presented MS stenosis as a novel cause of venous PT. The clinical presentation of MS stenosis is similar to that of LS stenosis, which is a common and well-known cause of venous PT. MS stenosis can be easily detected on postcontrast 3D MR imaging using oblique reconstructions and could be safely and efficiently treated with a stent.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received June 2, 2021.
- Accepted after revision August 18, 2021.
- © 2021 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}