
Abstract
SUMMARY: The carotid arteries, classically described as taking a relatively straight course through the neck, deviate medially in a minority of patients. At the extreme, the internal carotid arteries may “kiss” in the midline, coming extremely close to the pharyngeal wall. In this clinical report, we describe 5 patients with primary hyperparathyroidism, all with ectopic retropharyngeal parathyroid adenomas but all with varying carotid artery anatomy. We describe these variations using a previously developed clinical grading system that highlights 1) the relationship between carotid artery location and risk of injury during pharyngeal procedures and 2) the importance of universal, objective criteria to classify carotid anatomy. Radiologists should be familiar with variations in carotid anatomy and communicate them to the operative team.
ABBREVIATIONS:
- PHPT
- primary hyperparathyroidism
- MIBI
- technetium Tc99m sestamibi
- PTH
- parathyroid hormone
Although the carotid arteries classically run straight to the base of the skull, abnormalities in their anatomy may include tortuosity, kinking, or coiling of 1 or both of the arteries.1 The vessels may deviate medially so much that they come together at the midline, colloquially referred to as “kissing carotids.” Previously, there was no official classification system for carotid anatomy, making it difficult to estimate how common these anomalies are. Anatomic and radiologic studies have reported incidences ranging from 0.2% to 30% depending on the criteria used to define “abnormal.”1⇓⇓⇓-5 Pfeiffer et al5 recognized the need for a universal classification system and developed a convenient grading scale of I through IV based on the minimal distance from the internal carotid artery to the pharyngeal wall and the level of the pharynx (nasopharynx, oropharynx, or hypopharynx) where this occurs.
It is critical that radiologists be aware of these variations in carotid anatomy and, when discovered incidentally on preoperative imaging, accurately report these findings to the surgeon. Aberrant carotid arteries can have serious implications if un-known or unreported before procedures involving the pharyngeal area, such as tracheal intubation, tonsillectomy, retropharyngeal abscess drainage, removal of neoplasms, or removal of an ectopic parathyroid adenoma.6⇓-8 They can also cause symptomatic widening of the retropharyngeal space.9,10 In the Pfeiffer et al5 classification system, class I indicates a normal distance between the ICA and the pharynx, representing a presumably low risk for injury during pharyngeal procedures, and grade IV indicates a severely medialized ICA that poses a very high risk.
The retropharyngeal (paraesophageal) space is a common location for ectopic parathyroid glands.11 The incidence of ectopic glands is as high as 11%–16% among patients undergoing parathyroid surgery, and missed ectopic adenomas are a leading cause of persistent hyperparathyroidism requiring reoperation.11⇓-13 Because of advances in imaging techniques such as technetium Tc99m sestamibi (MIBI), often performed with SPECT/CT, and more recently the multiphase parathyroid 4D CT, radiologists are now frequently able to localize these adenomas before surgery.14,15
Anomalies of both the parathyroid glands and the ICAs have been well described independently, but there is no literature that draws an association between the two. We present preoperative imaging and intraoperative findings of 5 patients with primary hyperparathyroidism (PHPT) who presented for surgical consultation and were found to have ectopic parathyroid adenomas in the retropharyngeal space. The patients had varying carotid anatomy, ranging from a unilateral, slightly medialized ICA to “kissing” ICAs. Here we report on their presentation, work-up, and surgical procedures.
Case Series
Patient characteristics are described in the Table. All 5 patients were diagnosed with PHPT after routine screening laboratory studies revealed hypercalcemia, and all met the International Workshop on Asymptomatic Primary Hyperparathyroidism criteria for parathyroidectomy.16 For surgical planning, per institutional protocol for PHPT, all patients underwent 4D CT, and all but 1 also had MIBI SPECT/CT performed at the same time using a combined acquisition method.17 We classified the ICAs of each patient using the grading system developed by Pfeiffer et al5 (Table). In the 4 patients who underwent parathyroidectomy, intraoperative parathyroid hormone (PTH) levels fell appropriately by greater than 50% from pre-excision to 10 minutes postexcision, and final pathology was consistent with parathyroid adenoma. There were no complications, and all patients had normalized serum calcium levels at 6 months after surgery. One patient’s operation was delayed because of the coronavirus 2019 pandemic.
Patient characteristics
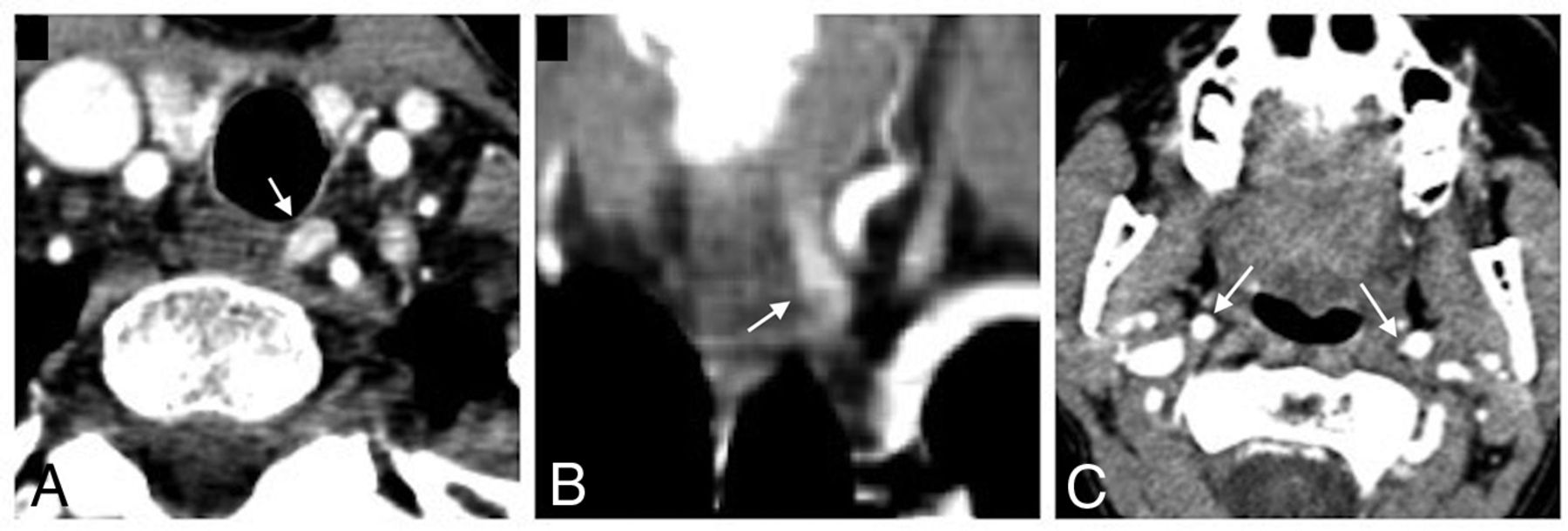
In case 1, 4D CT revealed an ectopically located right superior parathyroid adenoma in the retropharyngeal space (14 mm × 9 mm × 5 mm), posterior to the larynx at the level of the piriform sinuses, slightly right of midline (Fig 1A, -B). The adenoma was MIBI avid on SPECT/CT. The bilateral carotid arteries appeared medialized such that they nearly “kissed” immediately posterior to the oropharynx and larynx (Fig 1C, -D). The patient underwent a focused parathyroidectomy. After the right thyroid lobe and thyroid cartilage were mobilized and retracted, the bilateral internal carotid arteries were noted to be very medialized as expected. Posterior to the larynx in the retropharyngeal space, just anterior to the spine, a well-defined parathyroid adenoma was identified and resected.

Case 1. Contrast-enhanced CT scan shows axial (A) and coronal (B) images of the retropharyngeal parathyroid adenoma (arrow) and axial (C) and coronal (D) images of the nearly “kissing” carotid arteries (arrow).
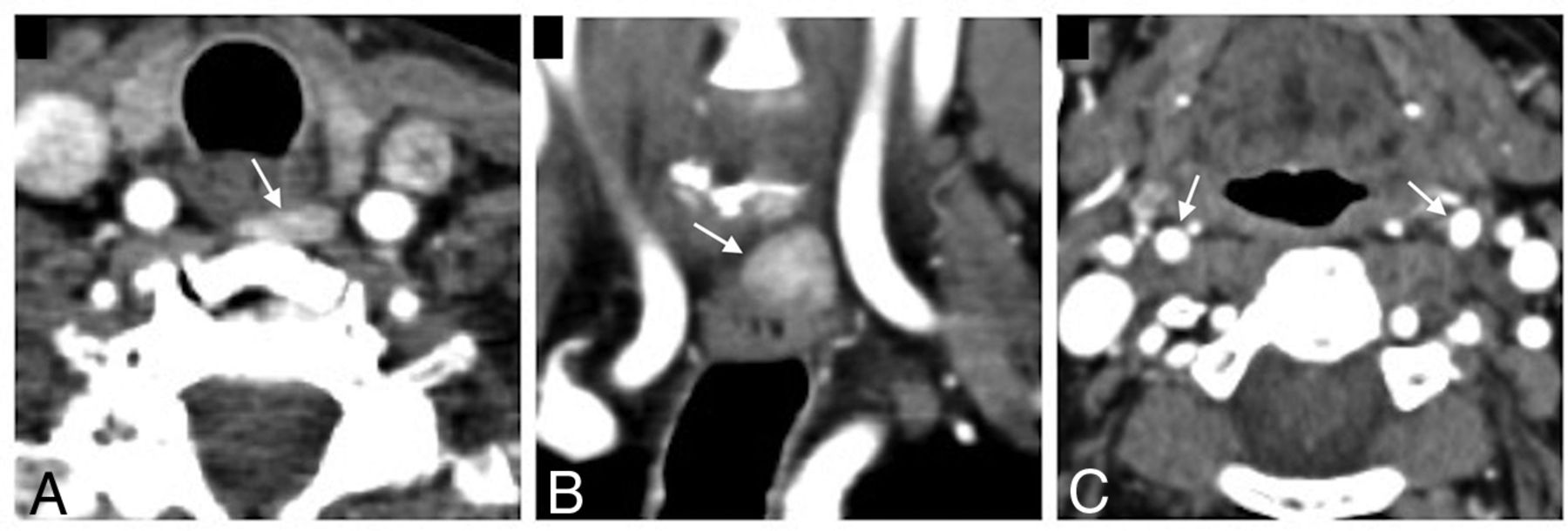
In case 2, 4D CT revealed a 6 mm × 9 mm × 20 mm enhancing paraesophageal nodule, consistent with a left upper parathyroid adenoma (Fig 2). The adenoma was MIBI avid on SPECT/CT. The adenoma was approximately 9 mm posterior to the lower pole of the left thyroid lobe and immediately anteromedial to the left carotid artery. The patient underwent a focused parathyroidectomy. The left thyroid lobe and thyroid cartilage were mobilized and retracted anteromedially. In the retropharyngeal space, posterior to the left lower pole, a well-defined parathyroid adenoma was identified, dissected, and excised.

Case 2. Contrast-enhanced CT scan shows axial (A) and coronal (B) images of the paraesophageal adenoma (arrow) and an axial (C) image of the bilateral internal carotid arteries (arrow) at the level of the oropharynx.
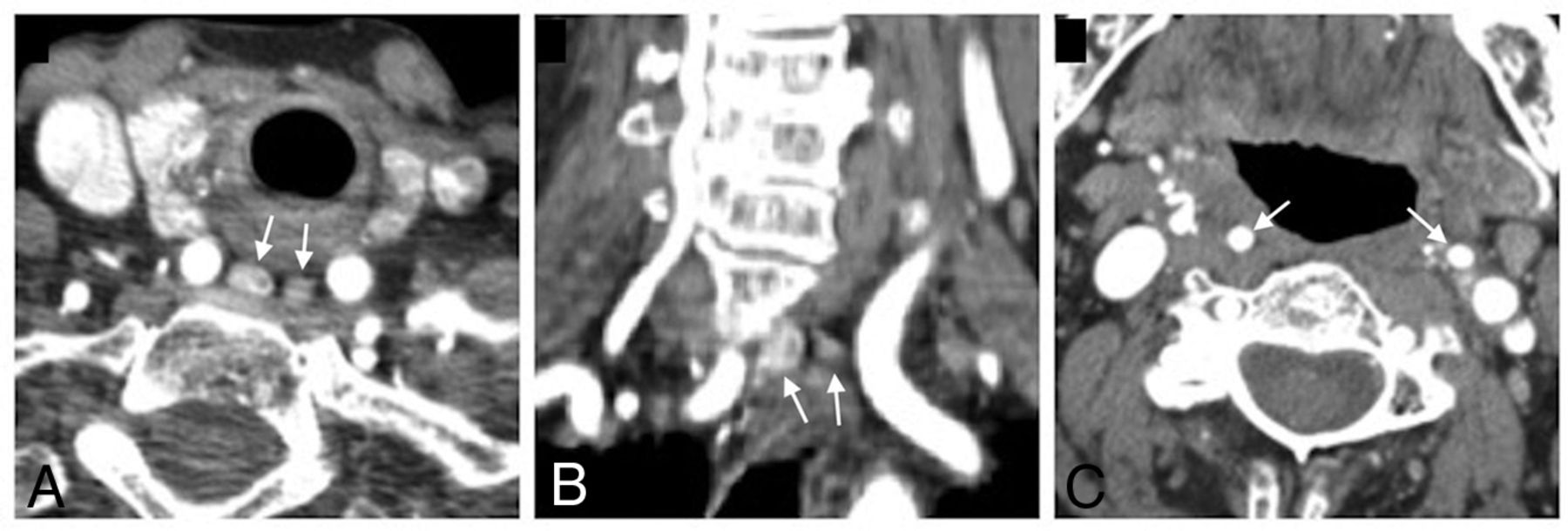
In case 3, the patient had undergone 2 neck explorations with resection of right upper and left lower adenomas 7 years and 2 years, respectively, before presenting to our institution for work-up of persistent hyperparathyroidism. An ectopic parathyroid adenoma (21 mm × 14 mm × 6 mm) was identified on 4D CT in the left retropharyngeal space immediately posterior to the esophagus and medial to the left common carotid artery (Fig 3), with corresponding increased MIBI uptake on SPECT/CT. The bilateral common carotid arteries appeared to be retropharyngeal and medialized with the adenoma in between the 2 arteries. The patient underwent a third parathyroidectomy. The left thyroid lobe was mobilized and retracted anteriorly, at which point the left common carotid artery was noted to be significantly medial, preventing easy identification of the parathyroid adenoma. After switching to a “backdoor” lateral approach (retraction of the sternohyoid and sternothyroid muscles anteriorly and more posterior dissection anterior to the sternocleidomastoid muscle), a classic parathyroid adenoma was accessed and identified in the retropharyngeal space posterior to the esophagus and medial to the left common carotid artery. The adenoma was dissected and excised.

Case 3. Contrast-enhanced CT scan shows axial (A) and coronal (B) images of the retropharyngeal parathyroid adenoma (arrow) between the common carotid arteries and an axial (C) image of the bilateral internal carotid arteries (arrow) at the level of the oropharynx.
In case 4, 4D CT revealed a left superior retroesophageal adenoma (12 × 12 × 5 mm), located immediately posterior to the left upper thyroid gland, 2 mm medial to the left common carotid artery (Fig 4). There was also an additional smaller hyperenhancing nodule adjacent to the right thyroid suggestive of a potential additional adenoma. The bilateral carotid arteries appeared to be in a relatively typical position. Because imaging suggested 2 potential adenomas, the patient underwent a bilateral neck exploration. Although imaging had suggested a left upper parathyroid adenoma, the left upper, left lower, and right lower glands all appeared to be of normal size and color in their usual positions. The retropharyngeal adenoma appeared to be an adenomatous right upper parathyroid gland, which was dissected and excised.

Case 4. Contrast-enhanced CT scan shows axial (A) and coronal (B) images of the retropharyngeal parathyroid adenoma (arrow) and an axial (C) image of the bilateral carotid arteries (arrow) at the level of the oropharynx.
In case 5, 4D CT revealed bilateral superior parathyroid adenomas (double adenomas) in the retropharyngeal space: right (8 × 7 × 14 mm) and left (5 × 4 × 8 mm) (Fig 5). Both adenomas were located immediately medial to medialized bilateral carotid arteries and posterior to the esophagus. The right superior adenoma was approximately 5 mm posterior to the right mid-thyroid gland, and the left superior adenoma was 12 mm posteromedial to the left mid-thyroid gland. On SPECT/CT, the larger right adenoma was MIBI avid, but the smaller left adenoma was not. The patient is currently taking cinacalcet (Sensipar) for medical management of PHPT and was scheduled for parathyroidectomy, but this was delayed because of the coronavirus 2019 pandemic. Of note, 6 months before her 4D CT, she underwent a left adrenalectomy for a left pheochromocytoma with elevated plasma metanephrines and normetanephrines. Given the patient’s age, both diseases were likely unrelated, sporadic, and not attributable to a genetic predisposition.

Case 5. Contrast-enhanced CT scan shows axial (A) and coronal (B) images of the double retropharyngeal parathyroid adenomas (arrow) and an axial (C) image of the bilateral carotid arteries (arrow) at the level of the oropharynx.
DISCUSSION
We have presented 5 patients with retropharyngeal parathyroid adenomas with varying anatomy of the carotid arteries. After applying the previously discussed grading system, all of these patients had at least 1 ICA that was grade II or higher, suggesting at least a moderate risk during pharyngeal procedures.5 Fortunately, all 4 patients who underwent surgery experienced no complications from intubation or the operation itself. To our knowledge, we are the first to report on a possible association between ectopic adenomas and medial deviations of the carotid arteries.
Theoretically, it is possible that these variants are related secondary to anomalous embryonic development in the neck. The parathyroid glands originate from the third (inferior glands) and fourth (superior glands) pharyngeal pouches, and the common carotid arteries and proximal ICAs derive from the third pharyngeal arch.7 Unsurprisingly, ectopic parathyroid glands are often found within structures that derive from neighboring embryologic tissues and descend into the neck, such as the thyroid, thymus, and carotid sheath.18 Other common locations for ectopic glands include the aforementioned retropharyngeal space, the tracheoesophageal groove, the thyro-thymic ligament, and elsewhere in the mediastinum.11
Clinically, this series highlights the importance of imaging for operative planning in parathyroid surgery. Advances in preoperative imaging have made it possible to localize disease and perform a focused parathyroidectomy in many patients, whereas the previous standard was a bilateral neck exploration.15 However, the utility of imaging in PHPT is dependent on the experience of the radiologist, who must be trained and experienced in parathyroid imaging to accurately interpret preoperative scans. Furthermore, when the radiologist suspects a retropharyngeal adenoma, it is especially critical to communicate to the surgeon any aberrant carotid anatomy that is at increased risk of injury when dissecting into the retropharyngeal space.
In summary, our experience with 5 patients raises the question of whether some association exists between retropharyngeal ectopic parathyroid adenomas and abnormal carotid artery anatomy, which could have implications for the radiologist and the parathyroid surgeon. Radiologists and surgeons alike should be aware of variations in carotid anatomy, and we agree with Pfeiffer et al5 on the importance of using a universal grading system to describe these variations objectively and relate them to operative risk.
Footnotes
Disclosures: James Lee—UNRELATED: Board Membership: Medscape, Summus; Expert Testimony: Various firms on individual basis.
References
- Received June 6, 2020.
- Accepted after revision November 24, 2020.
- © 2021 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}