
Article Figures & Data
Figures
- FIG 1.
Trigeminal nerve, associated nuclei, and major branches. Sagittal graphic (A) shows the major branches of the trigeminal nerve (CN V), including the preganglionic or cisternal segment (black straight arrow), trigeminal ganglion (black arrowhead) in the trigeminal cave, ophthalmic division (white straight arrow, CN V1) entering the orbit via the superior orbital fissure, maxillary division (white arrowhead, CN V2) exiting at the foramen rotundum, and mandibular division (white curved arrow, CN V3) exiting the skull base at the foramen ovale before transiting the infrazygomatic masticator space. Sagittal graphic (B) highlights the brain stem nuclei of the trigeminal nerve, including the mesencephalic nucleus (orange shading, black straight arrow), main sensory nucleus (blue shading, black arrowhead), spinal nucleus (pink shading, white straight arrow), and motor nucleus (green shading, white arrowhead). Axial graphic (C) demonstrates the course of the trigeminal nerves, including the preganglionic segments (black straight arrows), trigeminal ganglia (black arrowheads), ophthalmic divisions (white straight arrows, CN V1), maxillary divisions (white arrowheads, CN V2), and mandibular divisions (white curved arrows, CN V3), as well as the sensory (blue shading, black curved arrows) and motor (green shading, black dashed arrows) nuclei. Axial graphic (D) shows the relationship of the auriculotemporal nerve (black straight arrow), a complex branch of the mandibular nerve (black arrowhead, CN V3) that transits the infrazygomatic masticator space and parotid space, serving as an extracranial “bridge” linking CN V3 and the intraparotid facial nerve (white straight arrow, CN VII). Graphics are reproduced with permission from Imaging Anatomy: Brain and Spine and Specialty Imaging: Head and Neck Cancer. Copyright Elsevier.
- FIG 2.
Facial nerve, associated nuclei, and major branches. Axial graphic (A) shows the segments of the facial nerve (CN VII), including the cisternal (black solid arrow), canalicular (black arrowhead), labyrinthine (white solid arrow), tympanic (white arrowhead), and proximal descending mastoid (black solid curved arrow) segments. Note additionally the geniculate ganglion (white solid curved arrow) and greater superficial petrosal nerve (white dashed curved arrow). The 3 brain stem nuclei of CN VII are seen at the level of the pons, including the motor (orange shading, white dashed straight arrow), superior salivatory (pink shading, black dashed curved arrow), and solitary tract nuclei (blue shading, black dashed straight arrow). Sagittal graphic (B) shows the motor, sensory, and parasympathetic fibers of the facial nerve and its major branches. Motor fibers (orange shading) give off the small stapedius motor nerve (white dashed curved arrow) before exiting the skull base at the stylomastoid foramen as the extracranial CN VII (white solid arrow), which is purely motor. Parasympathetic fibers (shaded pink) give off the greater superficial petrosal nerve (black dashed straight arrow) that innervates the lacrimal gland and contribute to the chorda tympani nerve (black solid arrow). The chorda tympani nerve also receives special sensory fibers, providing taste to the anterior two-thirds of the tongue in addition to providing parasympathetic innervation of the submandibular and sublingual glands. Sagittal graphic (C) shows the extracranial motor branches of CN VII, including the temporal (black solid arrow), zygomatic (black arrowhead), buccal (white solid arrow), mandibular (white arrowhead), cervical (black dashed straight arrow), and posterior auricular (white dashed straight arrow) branches. Graphics are reproduced with permission from Imaging Anatomy: Brain and Spine. Copyright Elsevier.
- FIG 3.
Glossopharyngeal nerve, associated nuclei, and major branches. Coronal graphic (A) shows the glossopharyngeal nerves (black solid arrows, CN IX) exiting the skull base at the jugular foramina. CN IX is a mixed nerve, including afferent sensory fibers to the spinal nucleus of CN V (purple shading, black arrowhead), afferent special sensory fibers (taste from posterior two-thirds of the tongue) to the solitary tract nucleus (blue shading, white solid arrow), efferent motor fibers from the nucleus ambiguus (green shading, white dashed straight arrow), and efferent parasympathetic fibers from the inferior salivatory nucleus (lavender shading, black dashed curved arrow). Axial graphic (B) shows CN IX (black solid arrows) departing the medulla laterally at the postolivary sulcus and exiting the skull base at the pars nervosa segment of the jugular foramina. Note the brain stem nuclei of CN IX, including the spinal nucleus of CN V (purple shading, black arrowheads), solitary tract nucleus (blue shading, white solid arrows), inferior salivatory nucleus (pink shading, black dashed curved arrows), and nucleus ambiguus (green shading, white dashed straight arrows). Sagittal graphic (C) demonstrates the complex extracranial innervation provided by CN IX, including motor innervation of the stylopharyngeus muscle (black solid arrow, magnified inset), sensory innervation from the middle ear and parasympathetic innervation to the parotid gland via the tympanic (Jacobson) nerve (white solid arrow, magnified inset), sensory and taste from the posterior two-thirds of the tongue (black arrowhead), sensory from the soft palate and oropharynx (white arrowhead), and viscerosensory to the carotid sinus and body (white dashed straight arrow). Graphics are reproduced with permission from Imaging Anatomy: Brain and Spine. Copyright Elsevier.
- FIG 4.
Vagus nerve, associated nuclei, and major branches. Coronal graphic (A) shows the vagus nerves (black solid arrows, CN X) exiting the skull base at the jugular foramina. CN X is a mixed nerve, including afferent sensory fibers to the spinal nucleus of CN V (purple shading, black arrowhead), afferent special sensory fibers (taste from epiglottis and valleculae) to the solitary tract nucleus (blue shading, white solid arrow), efferent motor fibers from the nucleus ambiguus (green shading, white dashed straight arrow), and both efferent parasympathetic fibers from and afferent viscerosensory fibers to the dorsal vagal nucleus (rose shading, black dashed curved arrow). Axial graphic (B) shows CN X (black solid arrows) departing the medulla laterally at the postolivary sulcus and exiting the skull base at the pars vascularis segment of the jugular foramina. Note the brain stem nuclei of CN X, including the spinal nucleus of CN V (purple shading, black arrowheads), solitary tract nucleus (blue shading, white solid arrows), dorsal vagal nuclei (rose shading, black dashed curved arrows), and nucleus ambiguus (green shading, white dashed straight arrows). Sagittal graphic (C) demonstrates the complex extracranial innervation provided by CN X, including motor innervation of the soft palate and constrictors via the pharyngeal plexus (black solid arrow); motor innervation of the muscles of the larynx (except cricothyroid) via the recurrent laryngeal nerve (black arrowhead); special sensory (taste) from the epiglottis and valleculae (white solid arrow); afferent sensory from the external ear and skull base; parasympathetic innervation of the cervical, thoracic, and abdominal viscera; and viscerosensory afferents (white arrowhead) from the larynx, visceral space, chest, and abdomen. Graphics are reproduced with permission from Imaging Anatomy: Brain and Spine. Copyright Elsevier.
- FIG 5.
A 55-year-old man with secondary otalgia due to cervical spondylosis. Axial bone algorithm CT shows marked left-sided facet arthropathy (white arrow), which along with uncovertebral hypertrophy (black arrow) results in narrowing of the C II to C III neural foramen (white arrowhead). Impingement of the C III nerve root can lead to otalgia via referred pain along the great auricular or lesser occipital nerves.
- FIG 6.
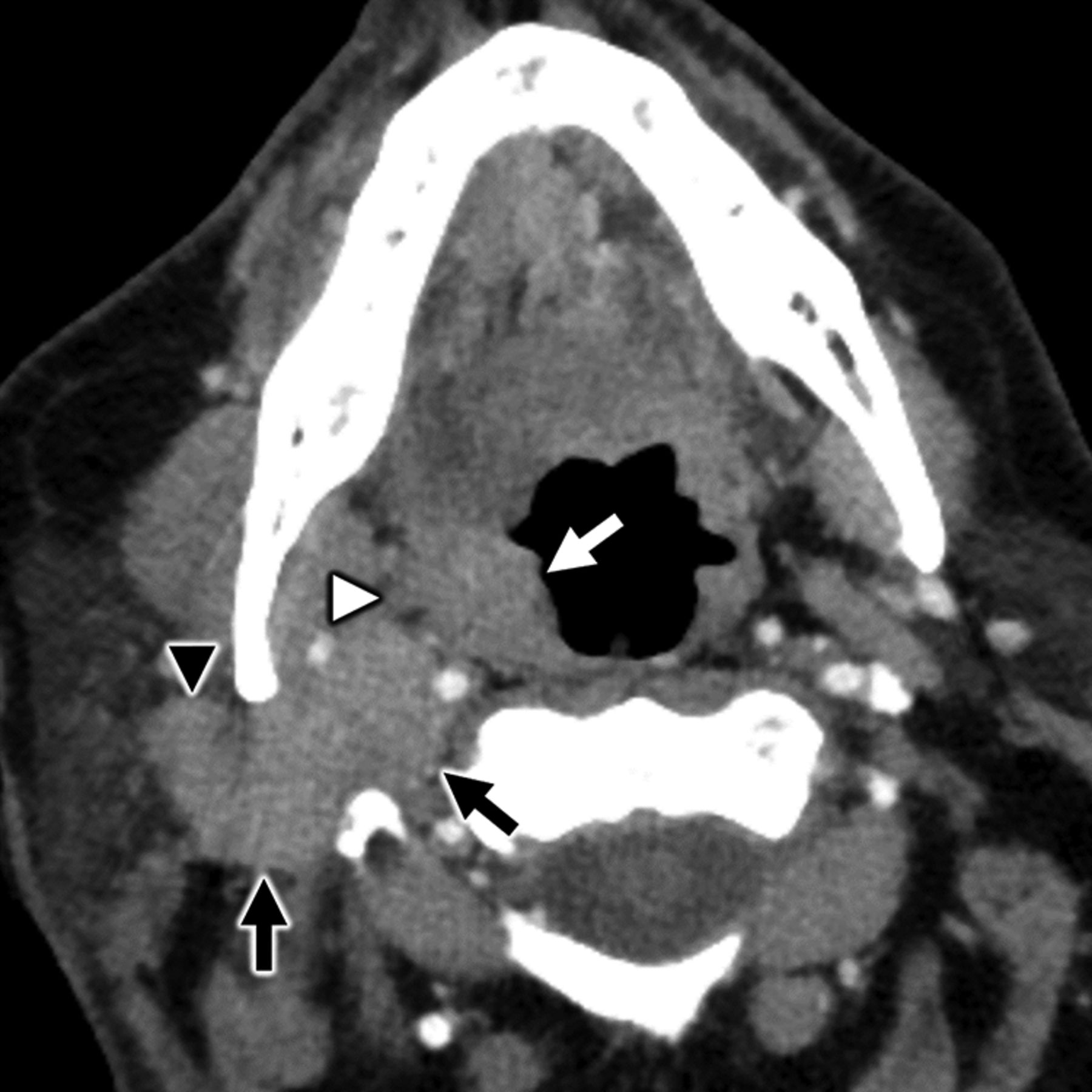
A 64-year-old man with secondary otalgia caused by palatine tonsil squamous cell carcinoma. Axial contrast-enhanced CT shows a right palatine tonsil mass (white arrow) with deep invasion through the superior constrictor (white arrowhead) into the parapharyngeal space. Conglomerate right level II cervical adenopathy (black arrows) with extracapsular spread displaces the carotid space and invades the parotid tail (black arrowhead). In this case, the patient’s referred otalgia may be caused by involvement of CN IX, CN X, and/or upper cervical nerve branches (great auricular or lesser occipital).
- FIG 7.
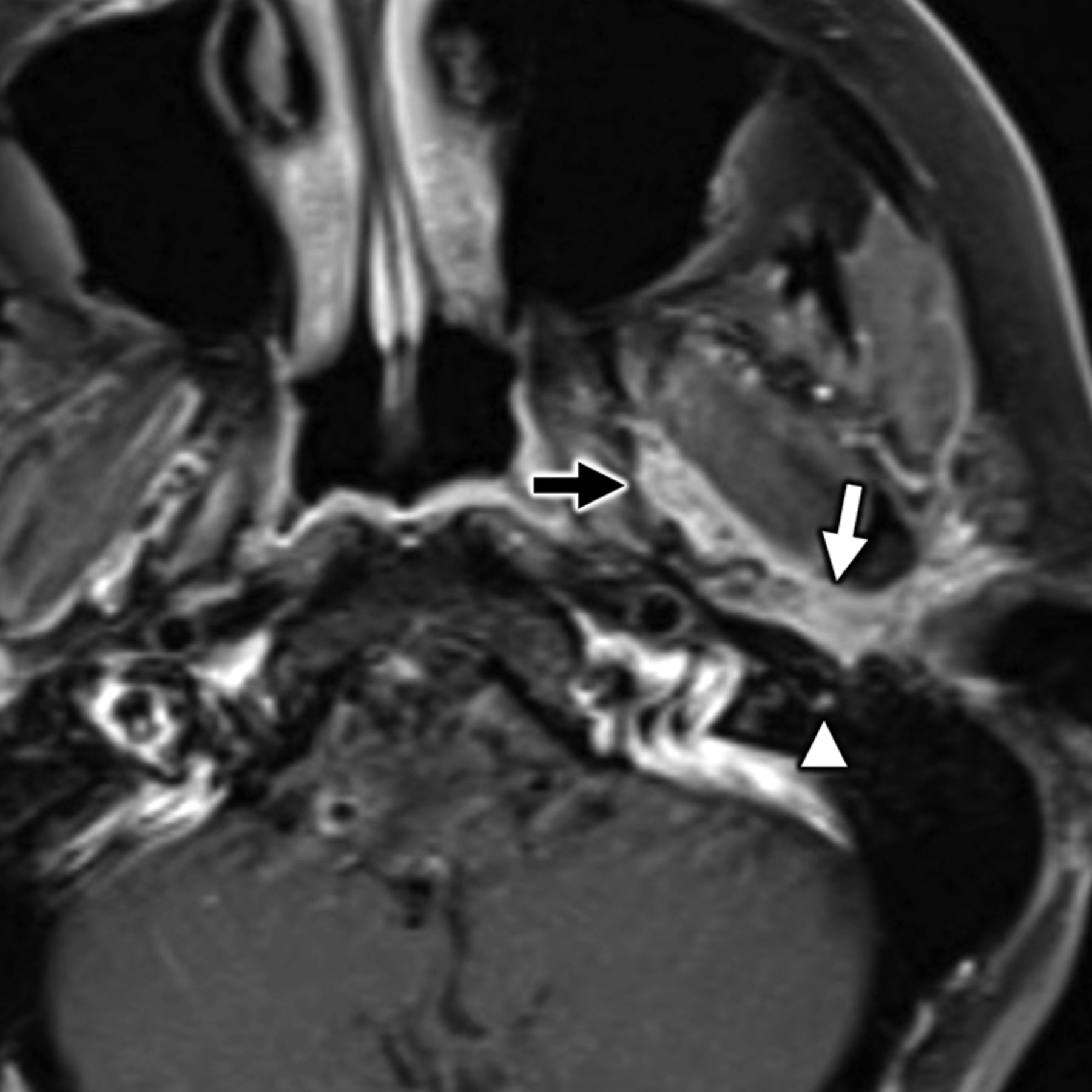
A 35-year-old man with secondary otalgia caused by perineural tumor spread from parotid adenoid cystic carcinoma. Axial T1-weighted postcontrast fat-saturated MR imaging shows cordlike enhancement (white arrow) along the course of the auriculotemporal nerve, which serves as an extracranial bridge linking the intraparotid facial nerve to CN V3 (black arrow) in the infrazygomatic masticator space. Note hyperenhancement along the descending mastoid segment of CN VII (white arrowhead) from additional perineural tumor spread. In this case, referred otalgia may occur along the auriculotemporal nerve, CN V3, and/or CN VII.
- FIG 8.
A 58-year-old woman with secondary otalgia caused by TMJ derangement. Oblique sagittal T1-weighted image in open-mouth position demonstrates irregularity and loss of normal biconcave morphology of the articular disk (white arrow), which has been displaced anteriorly. The disk does not recapture upon mouth opening, which prevents normal anterior translation of the mandibular condyle (white arrowhead) with respect to the articular eminence (black arrow). TMJ degeneration is a very common etiology of secondary otalgia with pain likely referred along CN V3.
- FIG 9.
Benign parotid pathology presenting with secondary otalgia. Axial contrast-enhanced CT in a 75-year-old man with right-sided ear pain shows obstructive calculous parotitis and sialodochitis with marked intraparotid ductal dilation (white arrow) and wall enhancement upstream of an obstructing sialolith (white arrowhead). Referred otalgia from intraparotid pathologies is thought to occur via the auriculotemporal nerve, a branch of CN V3.
- FIG 10.
A 42-year-old woman with secondary otalgia due to odontogenic infection. Axial T1-weighted postcontrast fat-saturated MR imaging shows a rim-enhancing subperiosteal abscess (white arrowhead). Note the corresponding hyperenhancing marrow (white arrow) from osteitis and hyperenhancing medial pterygoid (black arrow) and masseter (black arrowhead) muscles from myositis. Odontogenic infection is a common source of referred otalgia via CN V3 and its branches.
- FIG 11.
A 64-year-old woman with secondary otalgia caused by sinus mucosal disease. Axial bone algorithm CT shows a partially opacified right sphenoid sinus with marked hyperostosis and sclerosis of the sinus walls from long-standing mucoperiosteal reaction (white arrow) related to sinus mucosal disease. Note an air-fluid level (white arrowhead), which is a nonspecific finding that can be seen in the setting of acute inflammation related to the sinus mucosal disease. Sinus disease is a common source of secondary otalgia, thought to yield referred pain via CN VII parasympathetic branches or via CN V1 sensory branches.
- FIG 12.
A 52-year-old man with secondary otalgia caused by nasopharyngeal carcinoma (NPC). Axial T2-weighted fat-saturated MR imaging shows an intermediate signal intensity nasopharyngeal mass (white arrow) consistent with a cellular tumor, which extends laterally into the parapharyngeal space. Note the additional metastatic retropharyngeal adenopathy (white arrowhead) and left mastoid effusion. NPC may present with primary and secondary otalgia caused by mastoid–middle ear effusion (primary otalgia) and referred pain along CN IX (secondary otalgia).
- FIG 13.
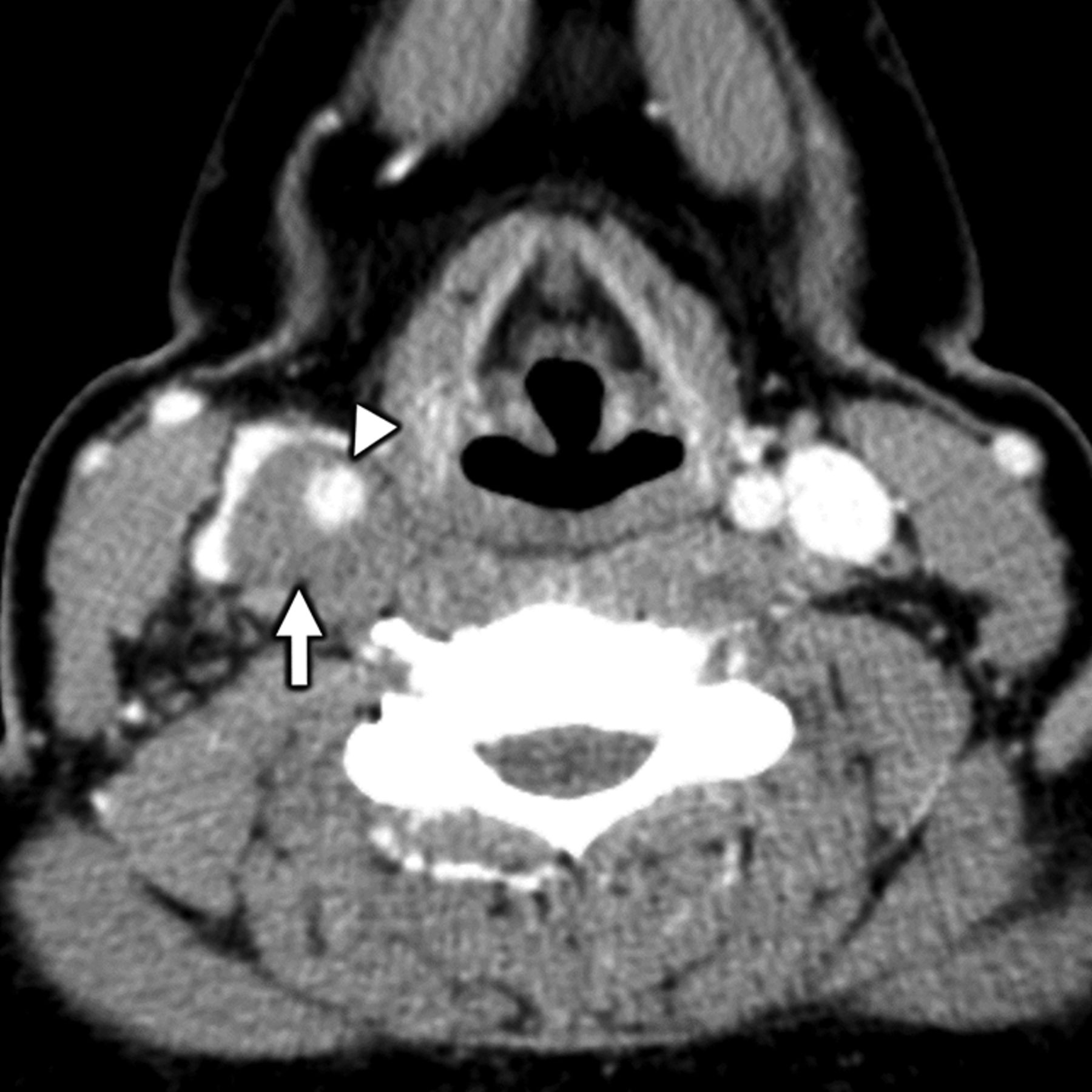
Transient perivascular inflammation of the carotid artery (TIPIC) syndrome presenting as otalgia. Axial contrast-enhanced CT in a 44-year-old woman with TIPIC syndrome shows characteristic segmental, eccentric soft tissue thickening (white arrow) around the wall of the common carotid artery. Note the lack of associated arterial stenosis (white arrowhead). TIPIC syndrome may yield referred otalgia via CN IX and/or CN X branches, depending on which segments of the carotid artery are involved.
- FIG 14.
A 58-year-old man with secondary otalgia caused by esophageal carcinoma. Coronal contrast-enhanced CT image shows segmental wall thickening (white arrow) of the distal cervical esophagus corresponding to the esophageal carcinoma. In this case, the referred otalgia likely occurred via CN X branches.














Tables
Nerve Primary Ear Sensory Innervation Origin Site of Referred Pain CN II and CN III Inferomedial and lateral pinna Skin overlying angle of mandible Pre- and postauricular skin Lateral neck Lobule Muscles of neck Upper cervical facet joints and nerve roots Atlantoaxial joint CN V Anterosuperior pinna Gingival and buccal mucosa of oral cavity External auditory canal Palate Tympanic membrane Floor of the mouth Anterior two-thirds of the tongue (sensory nerves) Mandibular teeth TMJ Mandible Nasal mucosa (sensory nerves) Paranasal sinus mucosa (sensory nerves) Parotid gland CN VII Conchal bowl Nasal mucosa (parasympathetic nerves) External auditory canal Sphenoid and ethmoid sinuses (parasympathetic nerves) Tympanic membrane Anterior two-thirds of the tongue (taste fibers) CN IX Tympanic membrane Stylopharyngeus muscle Posterior third of the tongue Palatine tonsil Carotid body Pharyngeal mucosa Parapharyngeal space Retropharyngeal space CN X Concha Oropharynx (vallecula and constrictor muscles) Postauricular skin Larynx Posterior external auditory canal Hypopharynx (pyriform sinus) Tympanic membrane Visceral space (thyroid, esophagus, and trachea) Component Specific Sites of Interest Ear and temporal bone External earExternal auditory canalMiddle ear, mastoidInner ear, otic capsule, and petrous apexPeriauricular soft tissues Central nervous system Midbrain, pons, and medullaUpper cervical spinal cord Upper cervical nerves (C II and C III) Occipitocervical and atlantoaxial jointsSpinal canal and neural foramina (C II and C III)Extracranial course of great auricular and lesser occipital nerves CN V, CN VII, CN IX, and CN X Cisternal segmentsSkull base or temporal bone segmentsExtracranial segments (masticator, parotid, and carotid spaces)Major waystations (pterygopalatine fossa and geniculate ganglion) “End organs” of innervation Major salivary glands (parotid, submandibular, and sublingual)OrbitsNose and sinonasal cavityOral cavity (tongue, mucosa, and palate)Maxilla and mandible (teeth and TMJ)Pharynx (nasopharynx, oropharynx, and hypopharynx)LarynxVisceral space (thyroid, esophagus, and trachea)Carotid space (carotid artery and internal jugular vein)Lymph nodes (cervical, retropharyngeal, and intraparotid) “Corners” of the examination Imaged portions of the brainImaged portions of the chest




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}