
Abstract
BACKGROUND AND PURPOSE: The purpose of this study was to evaluate the sensitivity and specificity of renal/ureteric opacification on postmyelographic CT as a sign of CSF leak.
MATERIALS AND METHODS: We performed a retrospective review of postmyelographic CT scans from 49 consecutive patients seen between January 2008 and August 2018 with imaging and/or clinical findings related to intracranial hypotension. Each scan was evaluated by both a neuroradiology fellow and a board-certified neuroradiologist for the presence of contrast in the renal excretory system. A similar assessment was also performed on 90 consecutive control subjects who underwent CT myelography for alternative indications.
RESULTS: Among the 49 patients with suspected CSF leak, 21 (43%) had an overt CSF leak on postmyelographic CT (group 1) and 28 (57%) did not (group 2). Overall, renal contrast was identified in 7/49 patients (14.3%): 5 (24%) patients in group 1, and 2 (7%) patients in group 2. Renal contrast was not seen in any of the 90 controls on postmyelographic CT.
CONCLUSIONS: Renal contrast was exclusively seen in patients with a clinically or radiographically suspected CSF leak. Given its 100% specificity, identification of this finding should prompt a second look for subtle myelographic contrast extravasation or an underlying CSF-venous fistula. Our results suggest that this sign may be considered an additional diagnostic criterion for CSF leak in the absence of an identifiable leak.
ABBREVIATIONS:
- CTM
- CT myelogram
- CVF
- CSF-venous fistula
- ICH
- intracranial hypotension
Spinal CSF leaks resulting in intracranial hypotension are an important and common cause of chronic postural, and often debilitating, headaches1⇓-3 in young and middle-aged individuals. Causes of spinal CSF leak include iatrogenic (operation, epidural injections, and fluoroscopically guided spinal interventions) or noniatrogenic traumatic injury to the dura, degenerative changes (ie, osteophytes), and the recently described CSF-venous fistula (CVF). Imaging plays a central role both in establishing the diagnosis of intracranial hypotension and in identifying the location of a CSF leak.4⇓⇓⇓-8 However, despite the advances in imaging, the number of cases without an identifiable cause remain high and can reach 46%–55% of cases in spontaneous intracranial hypotension (SIH).9,10 For optimal management of these patients, it is important that a firm diagnosis of intracranial hypotension and underlying CSF leak be established, even in the absence of an overt CSF leak.
Schievink et al4 have proposed 3 diagnostic criteria for spontaneous CSF leak and intracranial hypotension, which are independently diagnostic: A, B, and C. Criterion A is demonstration of spinal CSF leak on any spinal imaging. Criterion B is demonstration of cranial MR imaging related to intracranial hypotension such as a subdural fluid collection and brain sagging plus the presence of at least 1 of the following: low opening pressure (60 mm H2O or less), spinal meningeal diverticulum, or improvement of symptoms after epidural blood patching. Criterion C is the presence of all of the following or the presence of orthostatic headache and at least 2 of the following: low opening pressure (60 mm H2O or less), spinal meningeal diverticulum, and/or improvement of symptoms after epidural blood patching.4
CT myelography is often used to establish the source of spinal CSF leak, given its wide availability and relative ease of interpretation across different subspecialties compared with MR myelography and radionuclide cisternography. We have anecdotally observed opacification of the renal excretory system on CT myelograms obtained in patients with a suspected CSF leak. The purpose of this retrospective study was to assess whether the opacification of the renal excretory system could be used as an additional diagnostic sign of underlying CSF leak on CT myelograms (CTMs).
MATERIALS AND METHODS
An approval from the institutional review board at the Washington University in Saint Louis was obtained for this Health Insurance Portability and Accountability Act–compliant retrospective case-control research project.
Patient Selection
From our spine procedure data base, all consecutive adult patients (older than 18 years of age) who had undergone CT myelography between January 2008 and August 2018 in the setting of imaging and/or clinical findings of intracranial hypotension were included (Table 1). We additionally included 90 consecutive controls (Table 1) in whom lumbar CT myelography had been performed for indications other than suspected CSF leak. Patients who had received intravenous iodinated or gadolinium-based contrast within 48 hours preceding myelography were excluded. Studies that did not include the CT images of the lumbar spine or kidneys were also excluded. Indications for myelography in the control group were back pain (n = 79), radiculopathy (n = 4), spinal stenosis (n = 3), lower extremity weakness (n = 2), scoliosis (n = 1), fracture (n = 1), postfusion hardware failure (n = 1), and myelopathy (n = 1).
Distribution of cases with clinical and/or imaging concern for CSF leak and the control group
The 49 cases with imaging and/or clinical signs concerning for a spinal CSF leak that met the inclusion but not exclusion criteria were divided into 2 groups: Group 1 patients had CTM evidence of a CSF leak, and group 2 patients did not have any CTM evidence of a CSF leak. Group 2 was further assessed with respect to the presence or absence of imaging evidence of intracranial hypotension (ICH) on cranial MR imaging or a fluid collection on spinal MR imaging. These groups were then further evaluated for a response to the epidural blood patch and other pertinent clinical information.
Imaging Review and Statistical Analysis
Each CTM had initially been interpreted by a neuroradiology fellow and a board-certified neuroradiologist to evaluate a CSF leak. A neuroradiology fellow and a neuroradiology attending physician re-assessed these imaging studies for evidence of renal contrast, as evidenced by subjective visual recognition of opacification of the renal excretory system (ie, calyces, renal pelvis, ureters, or urinary bladder). In addition, the average Hounsfield unit of renal pelvises was calculated by averaging the Hounsfield unit of each renal pelvis as determined by placing a circular ROI measuring between 8 and 10 mm within it. ROIs were placed centrally unless an off-center location had to be selected due to the presence of streak artifacts or partial collapse of the central aspect of the renal pelvis. The Hounsfield unit value was not recorded if the small size of the renal pelvis or the presence of artifacts prevented placement of an ROI of >8 mm.
Both readers recorded the location of the CSF leak and epidural collection if they were present. They also reviewed other pertinent clinical and imaging records for categorization of patients based on the diagnostic criteria proposed by Schievink et al.4 The time from the start of the procedure (ie, initial fluoroscopic image obtained before access to the intrathecal space) to the time when the CT for the CTM was performed was recorded for all patients.
The mean and SD were calculated for the Hounsfield unit for patients with (groups 1 and 2) suspicion of CSF leak and for controls. Differences between these groups were tested for significance using an unpaired 2-sample t test. A P value < .05 was considered significant.
All the examinations were performed as single-energy CT on a Somatom Definition (Siemens, Erlangen, Germany) 128-section scanner with the following parameters: pitch = 0.9, kilovolt = 120, milliampere-second = 400, section thickness = 2 mm with a multiplane reconstruction increment of 1 mm. Both soft-tissue and bone kernels were included.
RESULTS
Of the 49 total patients with imaging and/or clinical signs concerning for a spinal CSF leak, 41 patients demonstrated clinical symptoms of headaches, orthostatic headaches, chronic headaches, and/or positional headaches with the remainder demonstrating various nonspecific symptoms of back pain, gait problems, falls, and so forth.
Direct evidence of CSF leak on CTM was seen in 21 patients (Fig 1, group 1: 7 men; mean age, 47.7 years; and 14 women; mean age, 45.8 years). Of these, 12 (57%) demonstrated cranial MR imaging findings of intracranial hypotension (Fig 2), whereas 5 (23%) did not. The remaining 4 patients did not have MR imaging of the brain. In 16/21 group 1 patients, an intraspinal epidural CSF leak was seen. The leak was foraminal in location in remaining 5 cases. Renal contrast on the CT myelogram was seen in 5/21 (23%) group 1 patients (On-line Table).

A 35-year-old man with trauma and MR imaging demonstrating a spinal fluid collection worrisome for CSF leak. Postmyelographic CT (A and B) reveals a ventral epidural fluid collection in the cervical spinal canal with right foraminal extension corresponding to an epidural CSF. A sagittal postmyelographic CT image (C) reveals gross extravasation of contrast into the interspinous space at C7–T1 at the suspected site of a ligamentum flavum injury. Axial images in soft-tissue windows demonstrate contrast in both renal collecting systems in this CTM without visualized intravenous contrast.

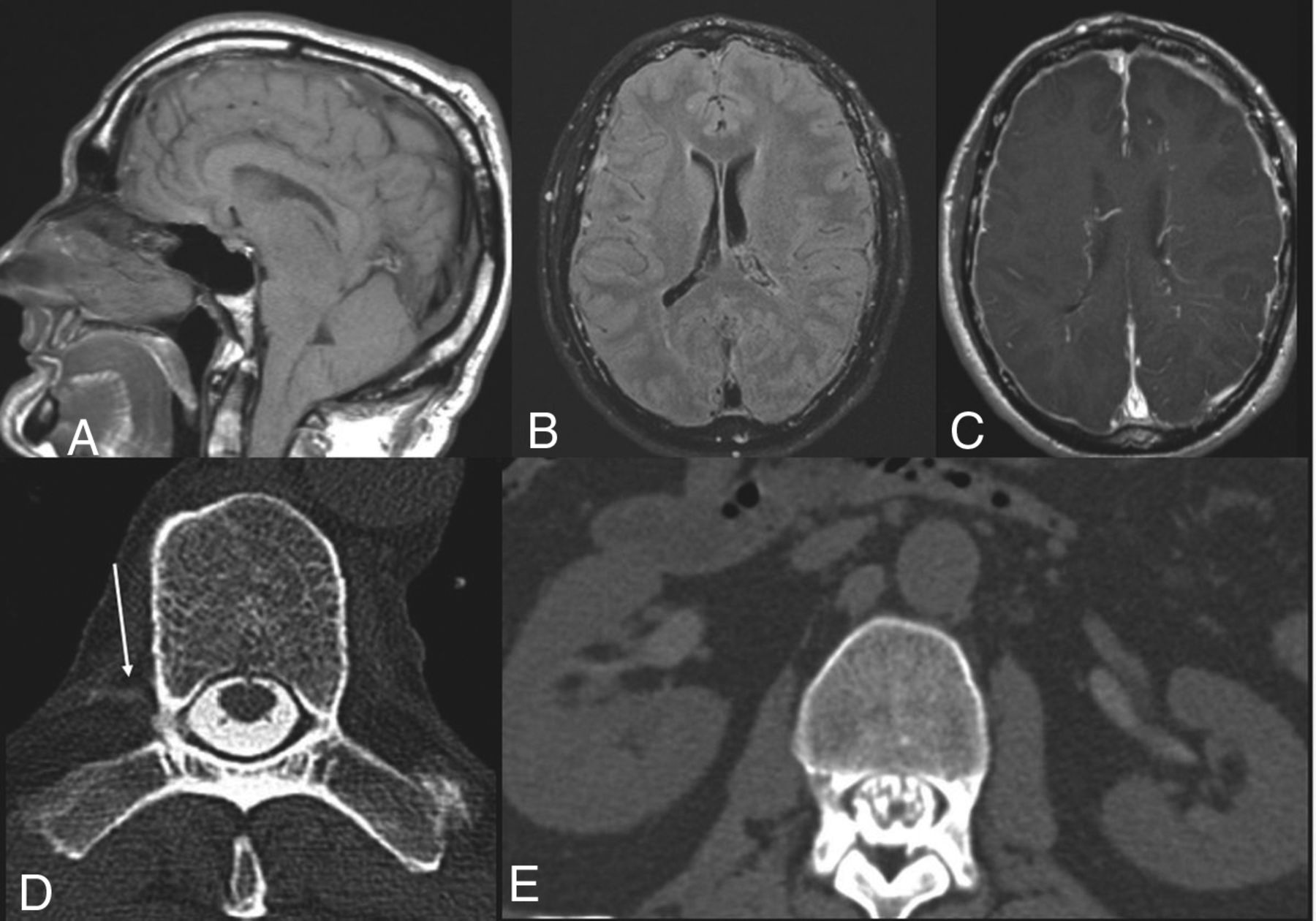
Upper images demonstrate signs of intracranial hypotension on brain MR imaging as demonstrated by cerebellar tonsillar descent through the foramen magnum (A), dilated venous sinuses (B), and diffuse pachymeningeal thickening and enhancement (C). Lower images demonstrate a CT myelogram in the same patient with a subtle CSF-venous fistula in the thoracic spine (arrow) and opacified renal collecting systems.
Those patients with a clinically suspected CSF leak without confirmatory evidence on CTM (group 2) included 8 men (average age, 37.9 years) and 20 women (average age, 55.5 years). Of these 28 patients, 8 patients met criterion B for the diagnosis of ICH and spinal CSF leak.4 Of the remaining 20 patients, 10 met neither criterion B nor C for the diagnosis of spinal CSF leak or ICH, and the other 10 could not be characterized using the criteria due to a lack of MR imaging or clinical data.
Only 2/28 (7.1%) patients in group 2 demonstrated renal contrast, both of whom met criterion B as demonstrated by MR imaging evidence of ICH as well as clinical symptom improvement with the epidural blood patch procedure. The first patient underwent an additional nuclear medicine examination for evaluation of a CSF leak, which demonstrated findings consistent with persistent CSF leak, confirming the diagnosis (On-line Table).
None of the controls demonstrated any renal or ureteric opacification on CT (Fig 3).

Contrast seen in the renal excretory system (renal contrast) in dark gray and total cases in each group in light gray.
Successful measurement of Hounsfield units of the renal collecting system could be performed in 68 controls and 34 patients (including 7 in whom the presence of excreted contrast in the collecting system was visually evident). Patients in whom myelography was performed to look for CSF leaks had higher mean Hounsfield units of the renal pelvises compared with the control group (Table 2, P < .001). Even patients without visually evident opacification of the renal collecting system had higher mean Hounsfield units compared with the control group (Table 2, P < .001).
Mean Hounsfield unit values of the renal collecting systems for each group
The time between intrathecal contrast administration and CT examination ranged between 45 and 74 minutes with a mean of 57 minutes for our cases positive for renal contrast. The average time from the first fluoroscopy image obtained to the CT scan was 57 minutes in the patients with a suspected CSF leak and without renal contrast and 58 minutes in the control group. There was no statistical difference for the fluoroscopy-to-CT scan time interval among all 3 groups, with the P values for cases positive for renal contrast and the control group being .94, the control group and suspected CSF leak without contrast being .81, and suspected CSF leak without contrast and contrast-positive cases being .89.
DISCUSSION
CSF leak is a source of substantial patient morbidity and remains a challenging diagnosis. While most patients present with typical postural headaches, a subset of patients present with vague or atypical symptoms that can result in a delay in diagnosis. Additionally, not all patients demonstrate the classic intracranial or spinal MR imaging findings of ICH. The acknowledgment of such diagnostic challenges and yet the need for rapid and definitive diagnosis of CSF leak and ICH have recently led to increased use of and dependence on imaging to establish the diagnosis with incorporation of imaging in the diagnostic criteria of ICH.4,11
Reliance on imaging to detect spinal sources of CSF leak will continue to increase, given the recent evidence suggesting that most spontaneous intracranial hypotension can be predominantly attributed to spinal sources (mechanical tears, CVFs, and leaking nerve root sleeves) and the increased rate of detection of a CSF leak with dynamic CT myelography.6,8,12⇓-19 Despite these advances, detection of the site of CSF leak continues to remain elusive, and in some cases, establishing the diagnosis of CSF leak or ICH remains uncertain.
The primary goal of imaging of patients with positional headaches or suspected ICH is to establish the diagnosis of CSF leak, and if possible, the source of the leak. Our study suggests that visualization of contrast within the renal collecting system or ureters (renal contrast) on CT myelography can serve to firmly establish the diagnosis of a CSF leak. Contrast opacification of the renal collecting excretory system was 100% specific for CSF leak. This subjective visual assessment was further confirmed objectively by a statistically significant difference between the mean Hounsfield unit in the collecting system between the control group and group 2. The objective measurement of the collecting system Hounsfield unit further adds validity to this finding and can, in combination with the visual assessment, serve as an additional sign of CSF leak.
Renal and ureteric renal opacification was noted in patients across multiple pathophysiologies, including traumatic dural tears, degenerative mechanical tears, CVF, and no identifiable CSF leak source. Renal and ureteric contrast opacification was also noted in patients with and without brain MR imaging findings of ICH and in patients with or without spinal fluid collections on MR imaging (slow or fast leak). This consistency across multiple pathophysiologies and positive or negative MR imaging findings supportive of CSF leak and/or ICH combined with 100% specificity makes this finding excellent for confirmation of a leak and an extremely valuable marker for occult spinal CSF leaks. As a result, renal contrast on CT myelography can be used as a definitive predictor or a major component of the diagnostic criteria for CSF leak.
Kinsman et al12 have recently shown similar results with renal contrast on CT myelography only detected in patients with spontaneous intracranial hypotension. However, in their study, renal contrast visualization was highly correlated with the presence of CSF venous fistulas in patients with spontaneous intracranial hypotension and was noted less frequently in patients with dural tears. This finding differs from those in our retrospective study because our study found that only 1 of the 7 cases was due to a CSF-venous fistula. However, because both studies are limited by power, studies with larger numbers of case series or a large-volume literature meta-analysis are needed to estimate the relative proportion of each etiology before associating this specific finding with a particular pathophysiology of CSF leak.
The underlying pathophysiology of this finding remains unclear. A potential explanation is the presence of direct communication between CSF and the venous system and, thus, rapid clearance of contrast by the collecting system as noted in CVF. However, the lack of consistency of this finding in all patients with CVF suggests an additional mechanism for this finding.12 Also, the presence of this finding, in our series and of that of Kinsman et al,12 in patients without CVF further supports additional factors contributing to the rapid renal clearance of CSF in selective patients with CSF leak. An interesting observation in our study is that subjective contrast opacification of the renal system on CT myelography was detected only in patients meeting the Schievink diagnostic criteria A or B, with none seen in patients meeting criterion C. This finding was similar to that of Kinsman et al because their study showed contrast opacification in patients with a detected leak on CT myelography (criterion A), patients with findings of ICH (criterion B), and patients with CVF.
Quantitative Hounsfield unit assessment revealed significant differences between the control group (average 3 Hounsfield units) and patients with suspected CSF leak without visually apparent renal contrast (average of 12 Hounsfield units). There was also a significant difference between the mean Hounsfield unit of the collecting system between groups 1 and 2. This may indicate that the extent of renal contrast excretion occurring by the time a postmyelogram CT is obtained is also a function of how much contrast ends up extravasating from the thecal sac. While arguing for measuring Hounsfield units of the renal pelvises, it also suggests the possible role of techniques such as dual-energy CT myelography in bringing out these inherent subtle contrast differences.20,21
Recognition of this sign has important implications in the management of patients with suspected ICH. It is well-recognized that identification and localization of a CSF leak can sometimes require multiple imaging studies, especially in patients who end up being diagnosed with CVF. Our results suggest that recognition of renal contrast on CT myelography should prompt a thorough review of CT myelography for subtle signs of CSF leak, and if not found, an active pursuit with additional imaging, including digital subtraction myelography to look for underlying pathology including a CVF or focal dural tear, should be performed.8,10,22
Limitations and Future Research
While our study highlights an important finding that can aid in establishing the diagnosis of spinal leak, prompting a search for a leak source in subtle or occult cases, we acknowledge several limitations. The first limitation was the relatively small sample size of the patient population. While we acknowledge that the sensitivity of our study for detection of CSF leak may be low, given the high specificity of the positive findings and the relatively large control group, these were not thought to limit the significance of the finding. Furthermore, the high specificity of this finding may prove helpful when applied to larger populations of patients. However, the small sample size limits association of this finding with specific CSF leak pathophysiology. Second, the recorded time between intrathecal contrast injection and the CT examination start was longer than the actual interval between the 2 examinations because the myelographic examination start was recorded from the first fluoroscopic acquisition rather than from the time of intrathecal contrast injection. However, this difference was not a significant limitation because the time interval between the 2 examinations remained relatively short and there was no significant difference in the time interval among all 3 groups. Third, a direct CSF leak was not detected on CT myelography in many of the cases; this finding may have been, at least partially, due to a combination of interval resolution of the presumed spinal CSF leak between initial symptom presentation and CTM acquisition and/or clinical misdiagnosis. Last, in the study design, the attending neuroradiologist and neuroradiology fellow who designed and completed this retrospective project were not blinded to the study and data collection. However, the conclusion derived by this nonblinded review is firmly supported by the objective, quantitative Hounsfield unit measurements.
CONCLUSIONS
Renal contrast was exclusively seen in the presence of CSF leak. Given its 100% specificity, identification of this finding should prompt a closer second look for subtle myelographic contrast extravasation or an underlying CVF. Our results suggest that this sign may be considered as an additional diagnostic criterion for CSF leak in the absence of an identifiable leak. This could be used in conjunction with known diagnostic criteria of CSF leak in SIH.4
References
- Received June 29, 2019.
- Accepted after revision December 9, 2019.
- © 2020 by American Journal of Neuroradiology




{kind=link}
{kind=link}
{kind=link}