
This article requires a subscription to view the full text. If you have a subscription you may use the login form below to view the article. Access to this article can also be purchased.
Graphical Abstract

Abstract
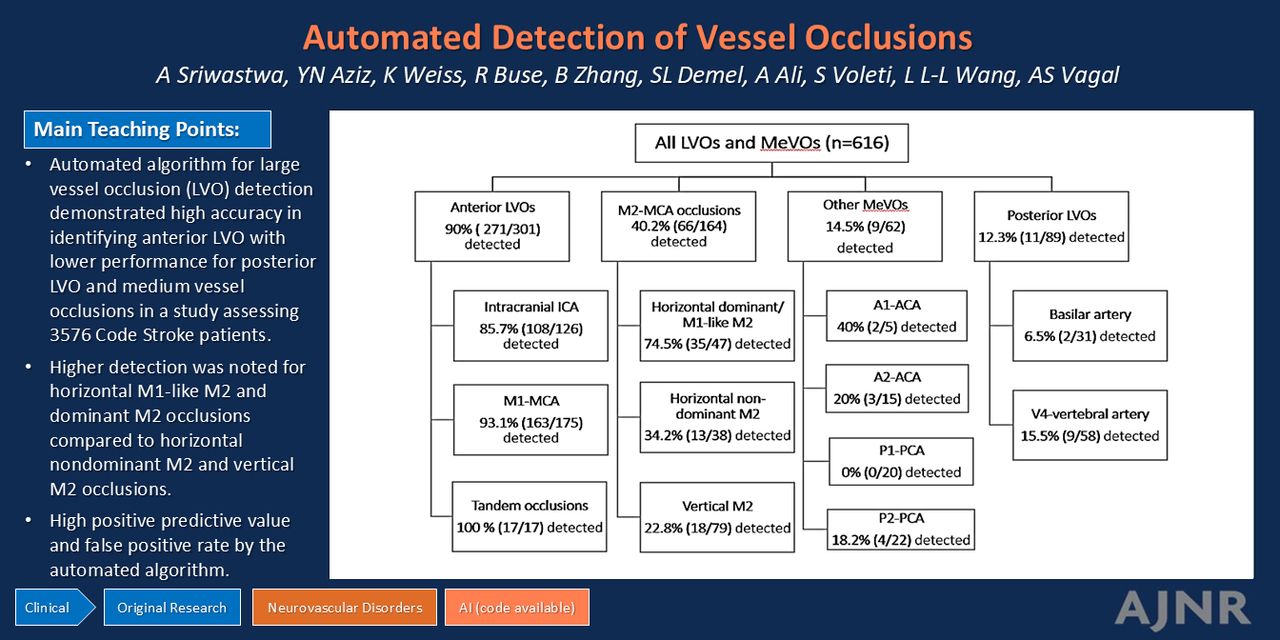
BACKGROUND AND PURPOSE: Fast, accurate detection of large (LVO) and medium vessel occlusion (MeVO) is critical for triage and management of acute ischemic stroke. Multiple artificial intelligence (AI)-based software programs are available commercially for automated detection and rapid prioritization of LVO. However, their ability, strengths, and limitations for detection of acute vessel occlusion in the context of expanding indications for mechanical thrombectomy are not entirely understood. We aimed to investigate the performance of a fully automated commercial detection algorithm to detect large and medium vessel occlusions in code stroke patients.
MATERIALS AND METHODS: We utilized a single-center, institutional, retrospective registry of all consecutive code stroke patients with CTA and automated processing by using Viz.ai presenting at a large comprehensive stroke center between March 2020 and February 2023. LVO was categorized as anterior LVO (aLVO), defined as occlusion of the intracranial ICA or M1-MCA, and posterior LVO (pLVO), defined as occlusion of the basilar artery or V4-vertebral artery. MeVO was defined as occlusion of the M2-MCA, A1/A2-anterior cerebral artery, or P1/P2-posterior cerebral artery. We compared the accuracy of Viz.ai by using STARD guidelines. Radiology reports from 12 board-certified radiologists were considered the reference standard. Our primary outcome was assessing accuracy of the automated software for aLVO. Our secondary outcome was assessing accuracy for 3 additional categories: all LVO (aLVO and pLVO), aLVO with M2-MCA, and aLVO with MeVO.
RESULTS: Of 3590 code stroke patients, 3576 were technically sufficient for analysis by the automated software (median age 67 years; 51% women; 68% white), of which 616 (17.2%) had vessel occlusions. The respective sensitivity and specificity for our prespecified categories were: aLVO: 91% (87–94%), 93% (92–94%); all LVO: 73% (68–77%), 92% (91–93%); aLVO + M2-MCA occlusion: 74% (70–78%), 93% (92–94%); and aLVO + all MeVO: 65% (61–69%), 93% (92–94%).
CONCLUSIONS: The automated algorithm demonstrated high accuracy in identifying anterior LVO with lower performance for pLVO and MeVO. It is crucial for acute stroke teams to be aware of the discordance between automated algorithm results and true rates of LVO and MeVO for timely diagnosis and triage.
ABBREVIATIONS:
- ACA
- anterior cerebral artery
- AI
- artificial intelligence
- aLVO
- anterior large vessel occlusion
- BA
- basilar artery
- EVT
- endovascular thrombectomy
- IQR
- interquartile range
- LVO
- large vessel occlusion
- MeVO
- medium vessel occlusion
- PCA
- posterior cerebral artery
- pLVO
- posterior large vessel occlusion
- VA
- vertebral artery
- © 2025 by American Journal of Neuroradiology
Log in using your username and password
Log in through your institution





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.