
Abstract
BACKGROUND AND PURPOSE: The Bern score is a quantitative scale characterizing brain MR imaging changes in spontaneous intracranial hypotension. Higher scores are associated with more abnormalities on brain MR imaging, raising the question of whether the score can serve as a measure of disease severity. However, the relationship between clinical symptom severity and the Bern score has not been evaluated. Our purpose was to assess correlations between Bern scores and clinical headache severity in spontaneous intracranial hypotension.
MATERIALS AND METHODS: This study was a single-center, retrospective cohort of patients satisfying the International Classification of Headache Disorders-3 criteria for spontaneous intracranial hypotension. Fifty-seven patients who completed a pretreatment headache severity questionnaire (Headache Impact Test-6) and had pretreatment brain MR imaging evidence of spontaneous intracranial hypotension were included. Pearson correlation coefficients (ρ) for the Headache Impact Test-6 and Bern scores were calculated. Receiver operating characteristic curves were used to assess the ability of Bern scores to discriminate among categories of headache severity.
RESULTS: We found low correlations between clinical headache severity and Bern scores (ρ = 0.139; 95% CI, −0.127−0.385). Subgroup analyses examining the timing of brain MR imaging, symptom duration, and prior epidural blood patch showed negligible-to-weak correlations in all subgroups. Receiver operating characteristic analysis found that the Bern score poorly discriminated subjects with greater headache severity from those with lower severity.
CONCLUSIONS: Pretreatment Bern scores show a low correlation with headache severity in patients with spontaneous intracranial hypotension. This finding suggests that brain imaging findings as reflected by Bern scores may not reliably reflect clinical severity and should not replace clinical metrics for outcome assessment.
ABBREVIATIONS:
- AUC
- area under the curve
- EBP
- epidural blood patch
- HIT-6
- Headache Impact Test-6
- ROC
- receiver operating characteristic
- SIH
- spontaneous intracranial hypotension
Spontaneous intracranial hypotension (SIH) is a condition that usually presents with orthostatic headaches and demonstrates ≥1 typical finding on brain MR imaging in most cases.1⇓-3 The Bern score is a quantitative scoring system based on these brain MR imaging findings that predicts the probability of extradural CSF on subsequent spinal imaging, with higher scores reflecting greater imaging abnormalities.4
Changes of SIH on MR imaging typically reverse following successful treatment.5,6 Given that Bern scores reflect the degree of abnormality on brain imaging, these scores could be used as a metric of disease severity and potentially as an outcome measure after interventions. To be useful as a severity measure, however, higher Bern scores should be correlated with higher levels of clinical severity because clinical symptom severity (typically headache severity) is the primary factor that motivates patients to seek medical care. The correlation between the severity of brain imaging abnormalities, as measured by the Bern score, and clinical severity has not yet been evaluated, to our knowledge.
The purpose of this investigation was to determine the degree of correlation between Bern scores and headache severity in SIH. Specifically, we sought to determine whether a correlation exists between pretreatment Bern scores and headache severity as measured by a validated headache severity questionnaire. Secondarily, we assessed the ability of the Bern score to discriminate patients with SIH whose headaches caused greater impact from those patients who were less clinically impacted.
MATERIALS AND METHODS
Subjects
This is a single-center, retrospective cohort of consecutive adult (18 years of age or older) patients who underwent a work-up for SIH at our institution between April 2016 and February 2018. As part of standard clinical care, patients routinely completed a questionnaire assessing clinical headache severity (the Headache Impact Test [HIT-6]) at presentation.7 This study was approved by our institutional review board and is compliant with the Health Insurance Portability and Accountability Act.
We included patients with pretreatment brain MR imaging showing signs of SIH, defined as the presence of any one of the following: diffuse pachymeningeal enhancement, brain sagging, or venous distension. Subjects were excluded if available pretreatment brain MR imaging was >6 months from the date that the HIT-6 questionnaire was administered or if HIT-6 data were missing. Subjects were also excluded if the brain MR imaging was performed without IV contrast, because these studies lacked sufficient data to calculate an accurate Bern score.
Evaluation of Headache Severity
All subjects completed a headache severity questionnaire before their visit to our institution. The 6-item HIT-6 is a validated instrument used to assess adverse headache impact and is used widely in clinical research and practice.8 HIT-6 scores range from 36 to 78, with a larger score indicating worse impact of headaches, stratified into 4 categories: little or no impact (≤49), some impact (50–55), substantial impact (56–59), and severe impact (60–78).8
Bern Score Calculation
Bern scores were calculated using established methodology previously described in the literature.4 A neuroradiology fellow with prior research experience in assessing brain MR imaging changes of SIH completed a supervised training set of cases constituting approximately 20% of the study population, to establish concordance with scores provided by a board-certified neuroradiologist with 14 years of experience in treating SIH. Bern scores for each subject were then calculated by the fellow, who was blinded to patient HIT-6 scores.
Statistical Analysis
Demographics, HIT-6 scores, and Bern scores were reported using the mean (SD) for continuous data or counts and percentages for categoric data for the overall cohort and the subgroups on the basis of the timing of brain MR images, symptom duration, and a prior epidural blood patch (EBP). The Pearson correlation coefficient (ρ) and 95% CIs using the Fisher Z-transform were calculated to assess correlations between the HIT-6 and Bern scores for the overall cohort and the subgroups.
Subgroup Analyses
We conducted subgroup analyses to determine whether correlations were affected by 3 variables: the timing of brain MR imaging, symptom duration, and a history of a prior EBP. To assess the impact of the length of time since brain MR imaging on the correlation between Bern scores and HIT-6 scores, we calculated correlation coefficients for the subgroups of patients whose MR imaging was obtained either 0–3 months or 3–6 months before HIT-6 assessment. To assess the impact of symptom duration, we calculated correlation coefficients between Bern scores and HIT-6 scores for the subgroups of patients whose symptoms started either <3 months or >3 months before brain MR imaging. Finally, correlation coefficients were calculated for the subgroups of patients who had or did not have an EBP performed in the interval between brain MR imaging and HIT-6 administration.
Receiver Operating Characteristic Analysis
To determine the ability of the Bern score to discriminate between subjects falling into the most severe headache stratum from those in less severe strata, we conducted a receiver operating characteristic (ROC) analysis. We grouped the HIT-6 scores into categories of severe (≥60) and not severe (<60) and constructed an ROC curve for the overall cohort to assess the ability of the Bern score to discriminate between these 2 groups. An ROC curve was also generated for the subgroup of subjects who completed the HIT-6 questionnaire within 0–3 months of brain MR imaging. There were insufficient data to generate an ROC curve for the subgroup of patients with brain MR images obtained 3–6 months before completing the HIT-6 questionnaire because all subjects were in the severe category. The area under the curve (AUC) and the 95% CI using a normal approximation were reported for each ROC curve.9
RESULTS
A total of 105 subjects with positive findings on pretreatment brain MR imaging were initially included. Forty-two patients were excluded because the MR imaging with positive findings was obtained >6 months from the HIT-6 score evaluation, and 5 patients were excluded because the initial MR imaging of the brain was performed without contrast administration, therefore providing an incomplete Bern score calculation. One patient was excluded due to an incomplete HIT-6 questionnaire.
The final study population thus consisted of 57 subjects, of whom 35 (61.4%) were women. The mean age was 53.6 (SD, 10.6) years (range, 30–73 years). CSF leaks were found to be caused by CSF-venous fistulas in 7 cases (12.3%), ventral dural tears in 13 cases (22.8%), lateral dural tears (ie, nerve root sleeve diverticula) in 9 cases (15.8%), and undetermined etiology with no visible epidural fluid in 28 cases (49.1%). Eighteen (31.6%) subjects had received a blood patch between brain MR imaging and HIT-6 administration.
The distribution of HIT-6 and Bern scores for the overall cohort and subgroups is listed in the Online Supplemental Data. Most subjects had reported the headache impact falling into the most severe category (n = 50, 87.7%), with only 1 (1.8%) subject's score reflecting “some impact,” with no subjects falling into the lowest category of “little to no impact.” Regarding Bern scores, most subjects (n = 44, 77.2%) fell into the high-probability category (ie, Bern score ≥5), with few subjects (n = 2, 3.5%) in the low-probability category (ie, Bern score ≤2). Because the presence of at least 1 sign of SIH on brain MR imaging was an inclusion criterion for this study, no subjects had a Bern score of 0.
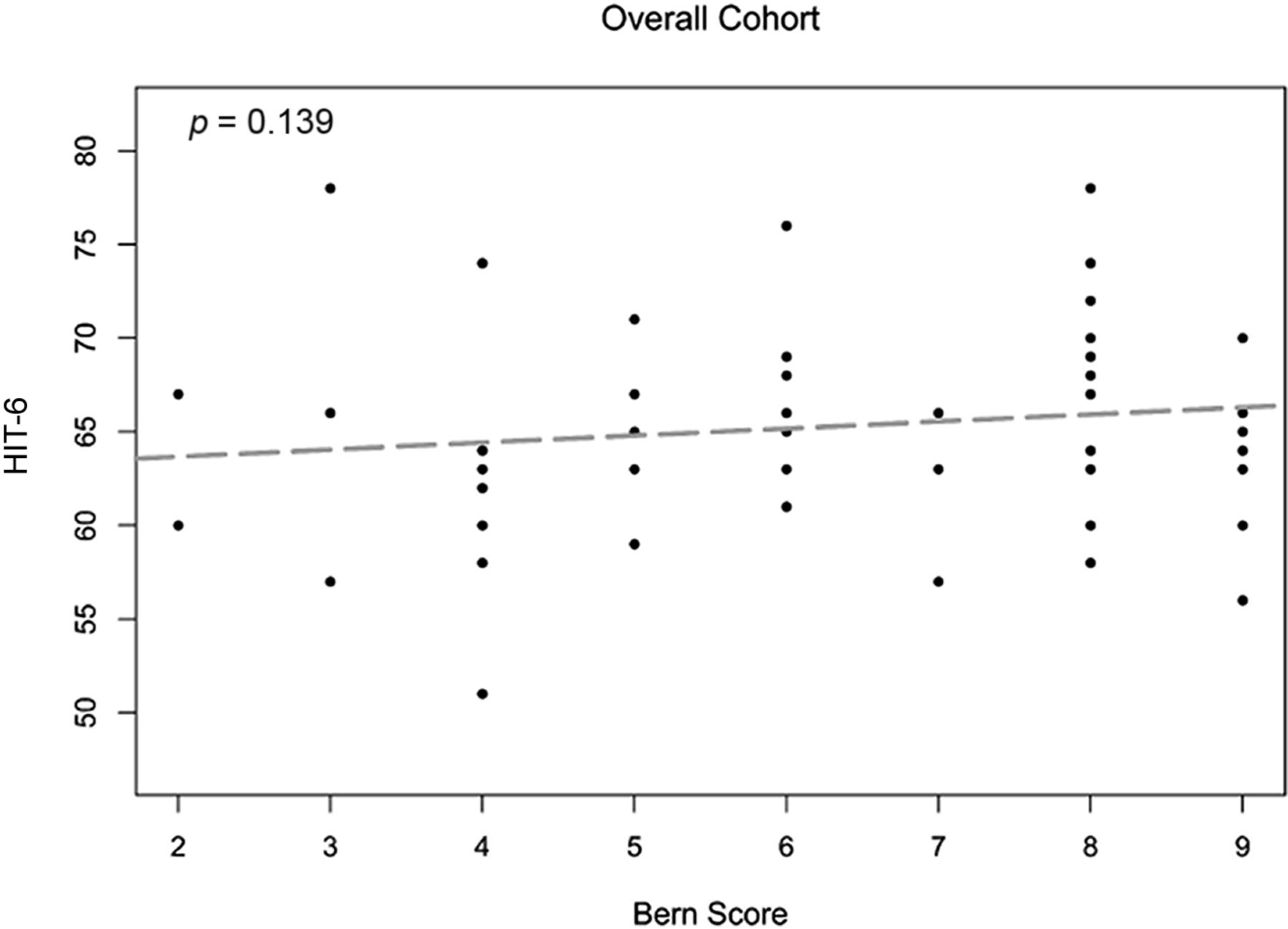
In the overall cohort, the correlation between paired HIT-6 and Bern scores was negligible (ρ = 0.139; 95% CI, −0.127−0.385) (Fig 1).

Scatterplot with best-fit line for the overall cohort shows a negligible correlation between the HIT-6 and Bern scores.
Subgroup Analysis Results
The correlations were negligible for both subgroups on the basis of the length of time between brain MR imaging and HIT-6 administration (Fig 2), with slightly lower correlation values in the group with brain MR imaging obtained 3–6 months before HIT-6 score collection (ρ = 0.070; 95% CI, −0.459 −0.562) compared with the group with brain MR imaging obtained 0–3 months before HIT-6 administration (ρ = 0.162; 95% CI, −0.150−0.444).

Subgroup analysis of subjects based on the time interval between brain MR imaging and HIT-6 administration. Scatterplots with best-fit lines show negligible correlations between the Bern score and the HIT-6 score in both the 0- to 3-month and 3- to 6-month subgroups.
Similarly, for subgroups based on the time from symptom onset to brain MR imaging (Fig 3), there was negligible correlation in the subgroup whose symptoms started >3 months before brain MR imaging (ρ = 0.078; 95% CI, −0.218−0.360). A slightly stronger but still overall weak correlation was seen in the subgroup whose symptom onset was 0–3 months before brain MR imaging (ρ = 0.343; 95% CI, −0.323−0.782).

Subgroup analysis of subjects based on symptom duration before brain MR imaging. Scatterplots with best-fit lines show weak correlation between Bern scores and HIT-6 scores for subjects with symptoms of 0- to 3-month duration and negligible correlation for subjects with symptoms of >3 months' duration.
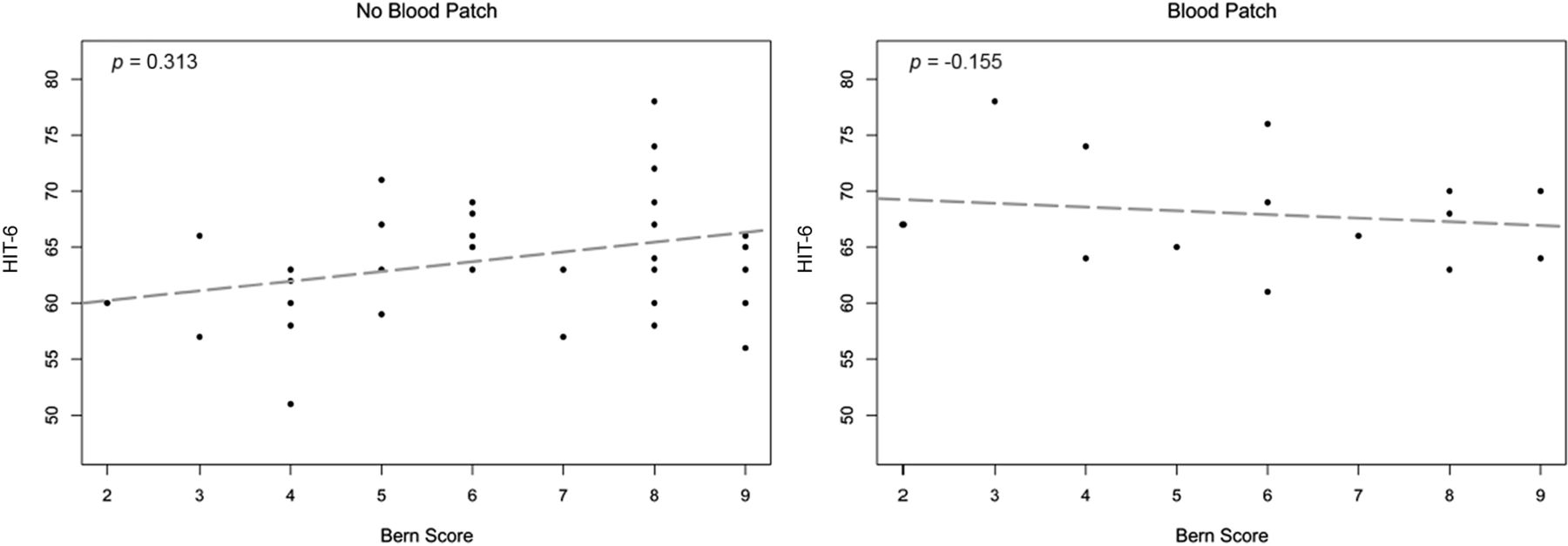
For subgroups based on whether subjects had received an EBP in the interval between brain MR imaging and HIT-6 administration (Fig 4), there was negligible correlation for those who had received an EBP (ρ = −0.155; 95% CI, −0.580−0.337) and a weak correlation for those who had not received an EBP (ρ = 0.313; 95% CI, −0.002−0.572).

Subgroup analysis of subjects who received or did not receive an EBP in the interval between brain MR imaging and HIT-6 administration. Scatterplots with best-fit lines show negligible correlation between HIT-6 and Bern scores in subjects who received an EBP and weak correlation in subjects who did not receive an EBP.
The Bern score performed poorly at discriminating subjects who fell into the headache severity categories of severe versus not severe in the overall cohort, as well as in the subgroup of subjects whose brain MR imaging was obtained 0–3 months before completing the HIT-6 score (AUC = 0.606; 95% CI, 0.347−0.864, and AUC = 0.635; 95% CI, 0.385−0.884, respectively) (Fig 5). Wide 95% CIs for the AUC values reflect the relatively small number of patients whose headaches did not fall into the severe subgroup.

ROC curves depicting the ability of the Bern score to discriminate severe from not severe HIT-6 groups in both the overall cohort (AUC = 0.606; 95% CI, 0.347–0.864) and subgroup of subjects with brain MR imaging 0–3 months from completion of the HIT-6 (AUC = 0.635; 95% CI, 0.385–0.884). Bern scores performed poorly in both groups in discriminating clinical headache severity.
DISCUSSION
Our investigation found a low correlation between clinical headache severity, as measured by HIT-6, and Bern scores. We also found that Bern scores showed limited ability to distinguish patients with the most severe headaches from those with lower headache severity. These findings suggest that brain imaging manifestations of SIH are poor predictors of clinical headache severity; thus, imaging findings in isolation may have limited utility as primary outcome measures when assessing treatment response.
Correlations between the Bern score and HIT-6 scores were slightly higher, but still weak, among those patients whose symptom onset was <3 months before brain MR imaging compared with those with a longer symptom duration. This result likely reflects brain imaging findings tending to become less pronounced with time,10 tending to weaken correlations between imaging and clinical symptomatology. We also found that subjects who had not undergone an EBP showed slightly higher correlation compared with those who had not undergone an EBP, likely reflecting partial treatment effect as a result of this treatment. Still, even among these subgroups in which correlations were slightly stronger, the magnitude of the correlations between HIT-6 and the Bern score was still weak.
The Bern score was developed as a tool for predicting which patients with SIH would have a visible epidural fluid leak on either conventional dynamic myelography or CT myelography.4 Although the initial derivation of the score did not include patients with CSF-venous fistulas, a subsequent investigation of patients with SIH with no epidural fluid found that the Bern score also predicted which patients would have a visible CSF-venous fistula on a lateral decubitus digital subtraction myelogram.11
Because the Bern score reflects brain imaging abnormalities and those abnormalities can reverse after treatment, it is tempting to consider that improvement in this score might serve as an indicator of successful treatment. An objective score based on brain imaging such as the Bern score would be especially attractive in light of the fact that rebound intracranial hypertension often occurs after successful closure of CSF leaks and can produce headaches that confound a clear posttreatment assessment of headache severity.12,13 To be useful, however, the score would need to strongly correlate with clinical symptomatology, because it is clinical symptoms that impact patient quality of life and thus drive treatment. Unfortunately, we found low correlations between Bern scores and headache severity, suggesting that while the Bern score clearly reflects physiologic alterations underlying SIH, more severe scores do not necessarily imply a more severe clinical manifestation of disease.
Limitations of this study include its retrospective nature and the single-institution design; our patient cohort consists of patients seeking care at a quaternary care center, which may impact generalizability and introduce spectrum bias. Second, readers of the brain MR imaging were not blinded to the diagnosis of SIH, which could have potentially biased Bern score assignments, though they were blinded to the HIT-6 score. Although all patients in this cohort met the criteria for SIH, we cannot guarantee that coexisting headache syndromes were not present. Additionally, the HIT-6 has not yet been validated specifically in SIH; however, it remains a widely validated scale to assess the impact of headache severity on the quality of life in other headache types, including episodic and chronic migraine, and has been used in clinical trials to assess disability due to headache.8,14 Moreover, from a practical perspective, there are no headache severity scores that have been specifically validated in SIH that could serve as alternatives.
Future effort to develop validated clinical outcome measures for SIH that account for the diversity of clinical presentations and posttreatment rebound intracranial hypertension is still very much needed, particularly because novel interventional techniques are developed for treatment of various leak subtypes. While this investigation suggests that assessment of brain imaging alone is unlikely to supplant clinical assessment as a surrogate marker of outcomes, the Bern score remains a valuable tool for standardizing assessment of brain imaging features and has been shown to be predictive of the diagnostic yield of spine imaging in multiple investigations. It will likely continue to be useful as part of the pre- and posttreatment assessment of patients with SIH.
CONCLUSIONS
Pretreatment Bern scores show a low correlation with clinical headache severity as measured by the HIT-6 in patients with SIH. This finding suggests that Bern scores do not reliably reflect headache severity and should not replace clinical outcome measures when assessing the effectiveness of SIH treatment.
Footnotes
This work is supported by the Biostatistics, Epidemiology, Research Design Methods Core funded through grant award No. UL1TR002553 from the National Center for Advancing Translational Sciences, a component of the National Institutes of Health.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received April 3, 2023.
- Accepted after revision July 6, 2023.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Assessing the Diagnostic Value of Brain White Matter Hyperintensities and Clinical Symptoms in Predicting the Detection of CSF-Venous Fistula in Patients with Suspected Spontaneous Intracranial Hypotension
- Early brain MRI changes following transvenous embolization of cerebrospinal fluid-venous fistulas in spontaneous intracranial hypotension
- Spinal CSF Leaks: The Neuroradiologist Transforming Care
- Perspectives from the Inaugural "Spinal CSF Leak: Bridging the Gap" Conference: A Convergence of Clinical and Patient Expertise
- Identifying Patients with CSF-Venous Fistula Using Brain MRI: A Deep Learning Approach