
Article Figures & Data
Figures
- FIG 1.
Anatomy of the brachial plexus. A frontal illustration (A) shows the anatomy of the brachial plexus as it arises from the neural foramina from the C4 to T1 levels, coursing between the anterior and middle scalene muscles and giving rise to many nerve branches. The cervical nerve roots of the brachial plexus are numbered 1 higher than the level where they originate (eg, the C5 nerve root arises from the C4 level, the C6 root from the C5 level, and so forth) because the C1 nerve root arises from above the C1 vertebral body at the skull base, and subsequently, there is a C8 nerve root but not a C8 vertebral body. The brachial plexus is divided into 5 roots, 3 trunks, 6 divisions, 3 cords, and terminal branches. A cross-sectional illustration (B) shows the anatomy of the proximal portions of the brachial plexus and nerve rootlets as they exit the spinal cord. Fibers from the dorsal rootlet complex with first-order sensory nerves in the dorsal root ganglion and fibers from both ventral and nerve rootlets blend before separating into ventral and dorsal nerve rami outside the neural foramina. The ventral rami go on to become the roots of the brachial plexus.
- FIG 2.
Inclusion and exclusion criteria. A flowchart delineates the inclusion and exclusion criteria used in this study, resulting in a case group of 36 and a control group of 50.
- FIG 3.
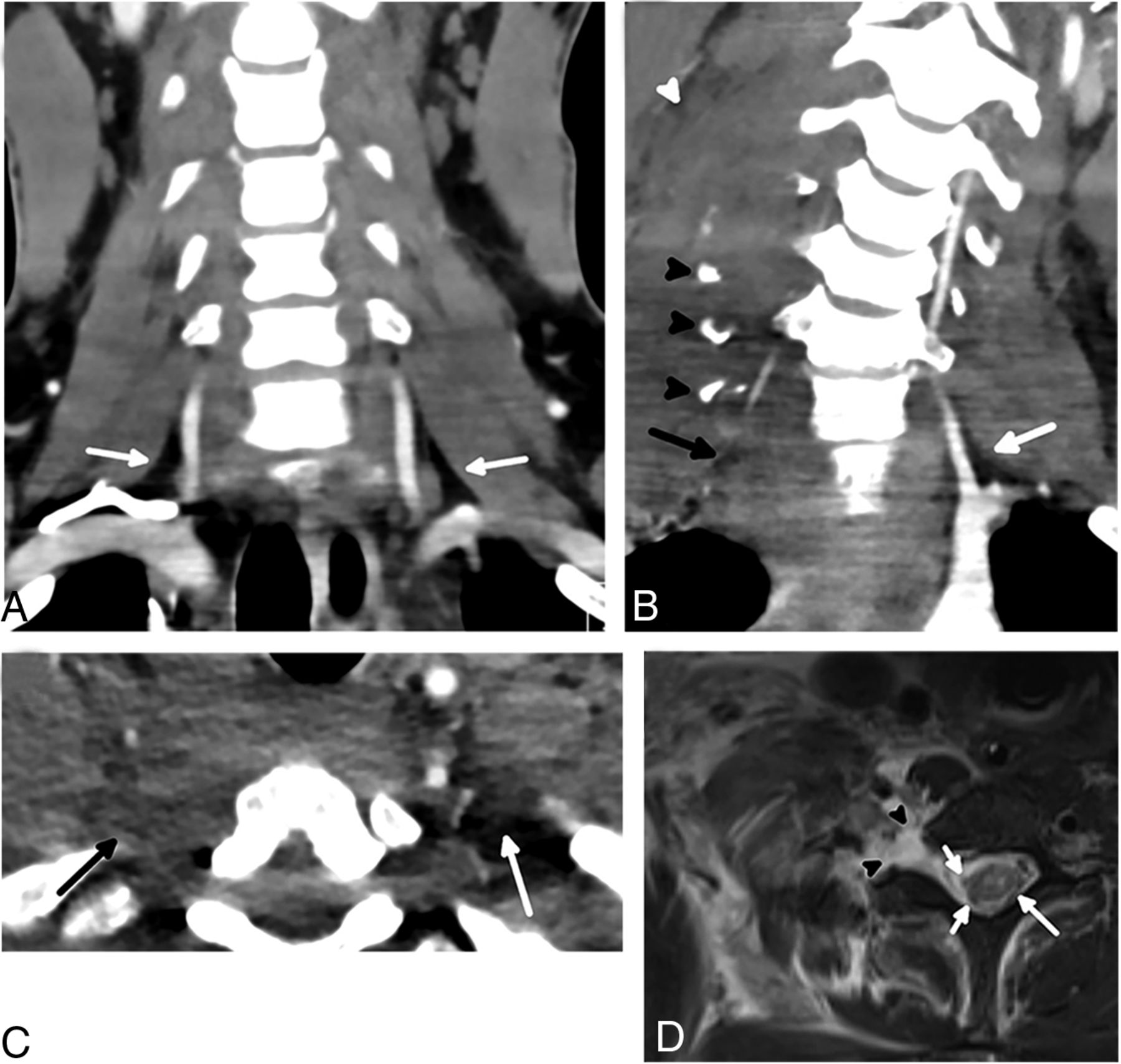
Normal and abnormal scalene muscles in different patients. An axial CT image in a 48-year-old man (A) without BPI shows normal anterior (black arrow), middle (white arrow), and posterior (arrowhead) scalene muscles without enlargement or edema. An axial CT image in a 52-year-old man (B) with BPI shows enlargement of the right scalene muscles (arrows) with extensive surrounding edema (arrowhead). A coronal CT image in the same patient (C) shows the extent of the asymmetric edema (arrows). A coronal T2 STIR MR imaging performed a day later in the 52-year-old patient (D) again shows scalene enlargement and edema (black arrow). Thickening and signal hyperintensity within the right C7 root (white arrow) are consistent with a stretch injury; similar findings were present at other levels.
- FIG 4.
Normal and abnormal interscalene fat pads in different patients. A coronal CT scan in a 26-year-old man (A) without BPI demonstrates smoothly marginated scalene muscles with normal interscalene fat pad (arrows). The coronal plane is a good place to assess the interscalene fat pad quickly by looking for this triangle of fat in the region of the proximal vertebral arteries, which should not have any stranding or hematoma. A coronal CT scan in a 25-year-old man (B) with BPI shows complete effacement of the right interscalene fat pad (black arrow) compared with the normal left interscalene fat pad (white arrow). Multiple displaced cervical transverse process fractures (black arrowheads) with scalene enlargement and edema (white arrowhead) are also present. An axial CT in the 25-year-old patient (C) shows the interscalene fat pad effacement (black arrow) in a different plane, compared with the normal left interscalene fat pad (white arrow). An axial T2-weighted MR imaging with fat saturation (D) performed a day later in the injured patient shows avulsion of the ventral and dorsal nerve rootlets (short white arrows), which was better appreciated when reviewing multiple sequential images. The spinal cord is slightly eccentric to the left and has abnormally increased signal (long white arrow), most pronounced within the gray matter. A large pseudomeningocele is present (arrowheads).
- FIG 5.
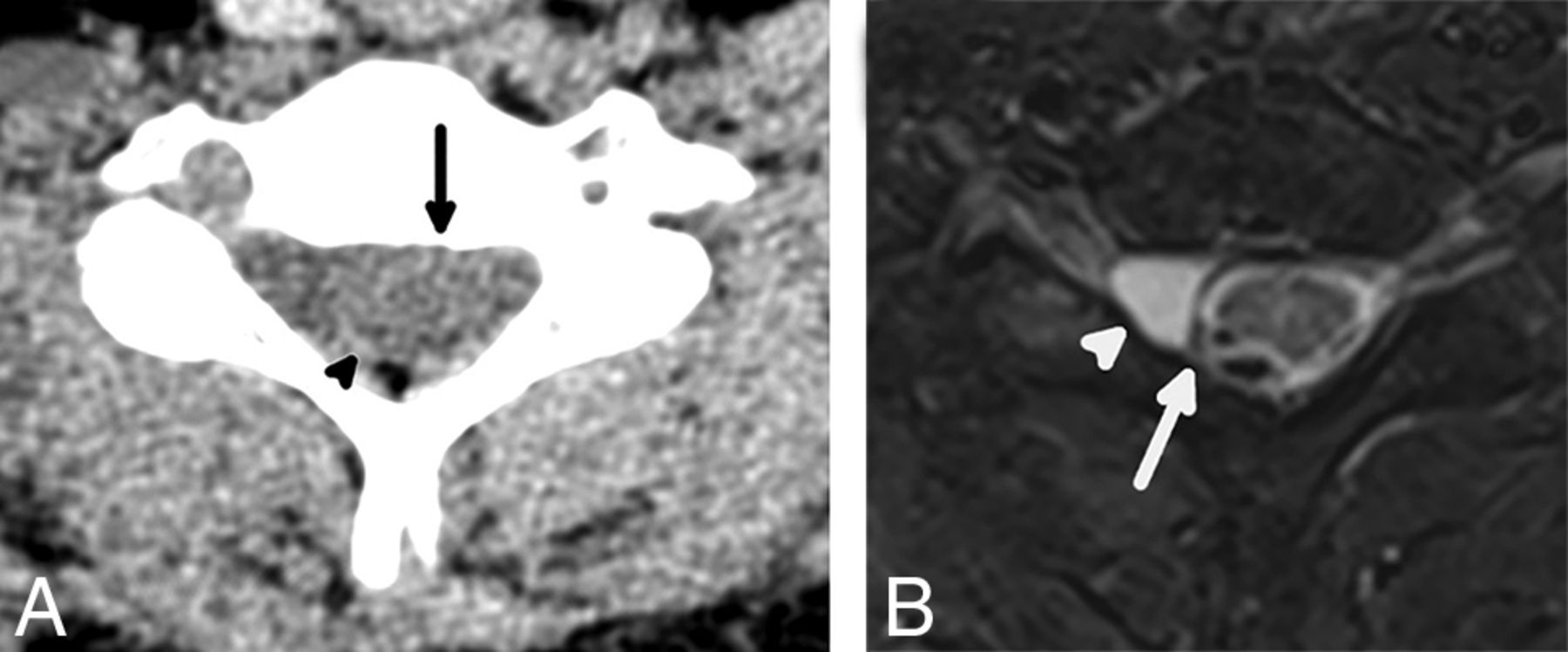
A 42-year-old man with preganglionic BPI and extra-axial hemorrhage. An axial CT image (A) shows a large extra-axial hematoma centered at the left of the spinal canal (arrow), which appears to compress the eccentric spinal cord (arrowhead). An axial T2 STIR MR imaging (B) in the same patient performed a day later shows an extra-axial hematoma (arrow); the hematoma and motion artifacts on the examination limit the diagnostic quality, but multilevel nerve rootlet avulsions are evident on sequential images. There is also severely abnormal signal hyperintensity (arrowhead) and a probable focus of hemorrhage (focal T2 hypointenisty) in the spinal cord.
- FIG 6.
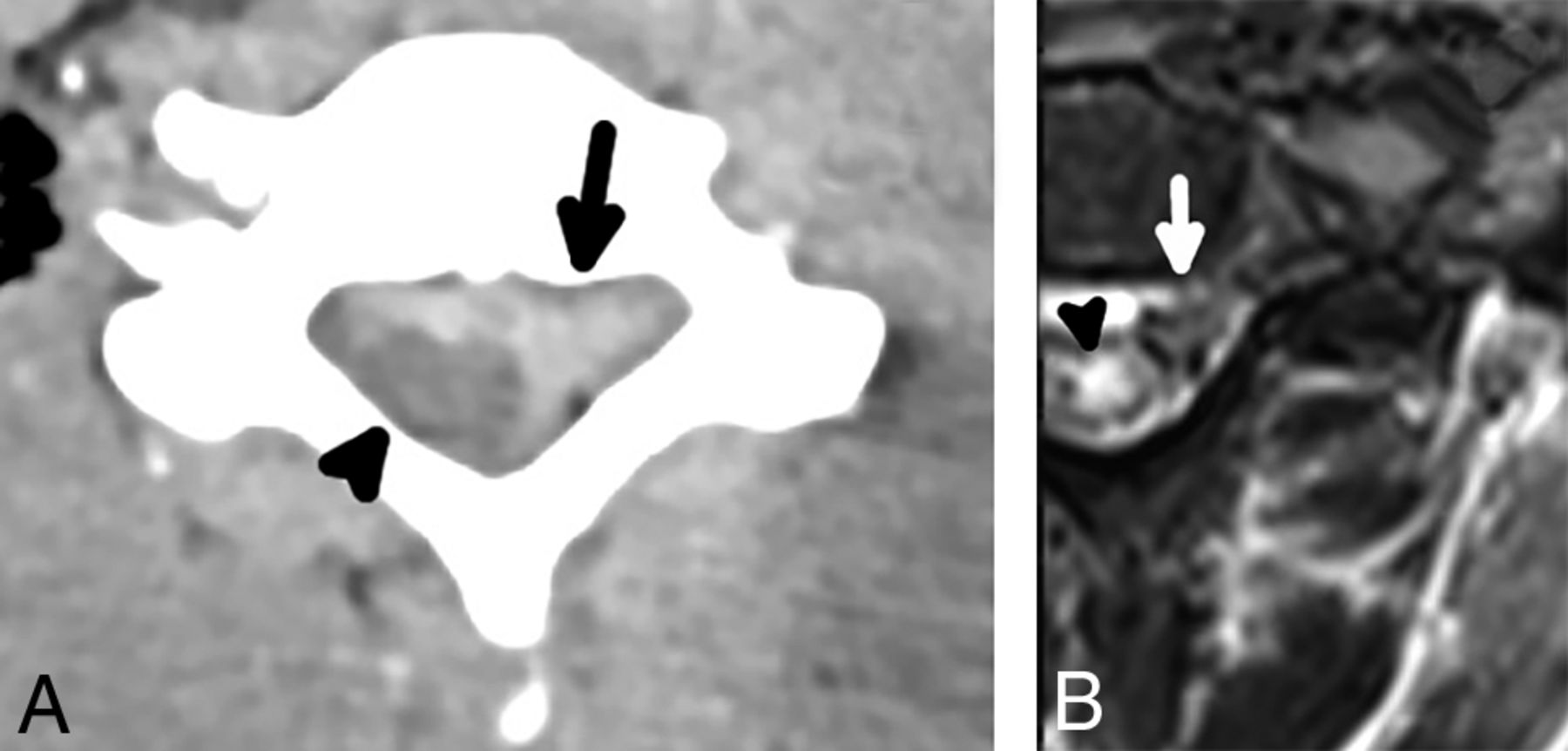
A 26-year-old man with preganglionic BPI and eccentricity of the spinal cord. An axial CT image (A) shows subtle eccentricity of the spinal cord and thecal sac (arrow) with an asymmetric amount of CSF in the right aspect of the spinal canal, which is indicative of a pseudomeningocele. There is also thin extra-axial hemorrhage (arrowhead) along the posterior aspect of the spinal cord. An axial T2 STIR MR imaging performed a day later in the same patient (B) shows complete avulsion of the ventral and dorsal nerve rootlets with eccentricity of the spinal cord (arrow), which is lateralized to the left of the spinal canal, compatible with preganglionic BPI. A small pseudomeningocele is confirmed on MR imaging (arrowhead) and is a finding highly associated with nerve rootlet avulsion.






Tables
Characteristic Cases (n = 36) Controls (n = 50) Age (range) (mean) (yr) 18–75 (38.7) 18–73 (41.5) Sex Male 29 36 Female 7 14 Mechanism of injury Motor vehicle collision 26 25 Motorcycle collision 5 1 Fall from heighta 3 8 All-terrain vehicle accident 2 0 Motor vehicle vs pedestrian 0 7 Assault 0 4 Fall from standing 0 3 Fall from horse 0 1 Bicycle accident 0 1 ↵a Fall from height = (>10 ft, 3.048 m).
Finding Cases (n = 36) Controls (n = 50) Sensitivity (95% CI) Specificity (95% CI) OR, P Value (95% CI) Scalene muscle edema/enlargement 34 6 94.44 (81.86–98.46) 88.00 (76.19–94.38) 130.33; P < .001 (24.77–685.87) Interscalene fat pad effacement 34 5 94.44 (81.86–98.46) 90.00 (78.64–95.65) 153.00; P < .001 (27.97–836.89) First-rib fracture 14 7 38.89 (24.78–55.14) 86.00 (73.81–93.05) 3.91; P = .01 (1.38–11.09) Cervical lateral mass or transverse process fracture 20 4 55.56 (39.58–70.46) 92.00 (81.16–96.85) 14.38; P < .001 (4.27–48.45) Extra-axial spinal canal hemorrhage 10 0 27.78 (15.85–43.99) 100.00 (92.86–100) 40.02; P = .01 (2.26–709.90) Spinal cord eccentricity 5 0 13.89 (6.08–28.66) 100.00 (92.86–100) 17.63; P = .05 (0.9425–329.97)





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.