
Abstract
BACKGROUND AND PURPOSE: We performed this study to identify the effect of the nationwide iodinated contrast media shortage due to reduction in GE Healthcare production, initiated on April 19, 2022, on the evaluation of patients with stroke.
MATERIALS AND METHODS: We analyzed the data on 72,514 patients who underwent imaging processed with commercial software in a sample of 399 hospitals in United States from February 28, 2022, through July 10, 2022. We quantified the percentage change in the daily number of CTAs and CTPs performed before and after April 19, 2022.
RESULTS: The daily counts of individual patients who underwent CTAs decreased (a 9.6% reduction, P = .002) from 1.584 studies per day per hospital to 1.433 studies per day per hospital. The daily counts of individual patients who underwent CTPs decreased (a 25.9% reduction, P = .003) from 0.484 studies per day per hospital to 0.358 studies per day per hospital. A significant reduction in CTPs using GE Healthcare contrast media (43.06%, P < .001) was seen but not in CTPs using non-GE Healthcare contrast media (increase by 2.93%, P = .29). The daily counts of individual patients with large-vessel occlusion decreased (a 7.69% reduction) from 0.124 per day per hospital to 0.114 per day per hospital.
CONCLUSIONS: Our analysis reported changes in the use of CTA and CTP in patients with acute ischemic stroke during the contrast media shortage. Further research needs to identify effective strategies to reduce the reliance on contrast media–based studies such as CTA and CTP without compromising patient outcomes.
ABBREVIATIONS:
- LVO
- large-vessel occlusion
- PHI
- patient health information
- rCBF
- regional CBF
- Tmax
- time-to-maximum
On April 19, 2022, GE Healthcare notified medical facilities that orders for its iodinated contrast media products for CT would be rationed after a coronavirus disease 2019 (COVID-19) outbreak resulted in lockdown of its production facility in Shanghai, China.1,2 The lockdown resulted in the interruption of the production of the iodinated contrast media iohexol (Omnipaque; GE Healthcare) at the primary GE Healthcare manufacturing facility.2 Although there were other suppliers such as Bracco Diagnostics, Bayer AG, and Guerbet for iodinated contrast media, they were unable to rapidly increase production to meet the demand for iodinated contrast media. CT imaging including CTA and CTP using IV contrast media was the main technique for identification of patients with acute ischemic stroke who may be candidates for endovascular treatment at that time.3,4 Several strategies were introduced to modify the neuroimaging protocols for patients with acute ischemic stroke in various institutions, including selecting fewer patients for CTA and CTP after initial screening based on clinical criteria and a noncontrast CT scan, modifying the protocol for acquisition of CTA and CTP, and/or using MR imaging to triage patients with acute ischemic stroke.5⇓⇓-8 Although there are reports on the effect of the shortage of contrast media,9,10 the effect on a larger scale on neuroimaging evaluation of patients with stroke has not been quantified.
MATERIALS AND METHODS
We analyzed the data collected in a commercial neuroimaging data base associated with the Viz.ai software platform (viz.ai) as a surrogate for the quantity of neuroimaging evaluations that hospitals provided for patients with acute ischemic stroke. In routine use, neuroimaging for acute ischemic stroke comprising noncontrast CT, CTA of the head and neck, and/or CTP of the brain is transmitted in real-time from the point of acquisition to a local DICOM gateway that forwards the scans to the cloud hosting Viz.ai imaging software. Images are transmitted to the Viz.ai server in DICOM format with associated metadata that include patient age, sex, site of imaging, and date and the time of image acquisition. These data are processed by the Viz.ai server and sent to the appropriate clinical teams for patient care. Data are then anonymized by the Viz.ai server and transmitted to a central data warehouse. Viz.ai ensured compliance with Health Insurance Portability and Accountability Act (HIPAA) Privacy and Security Rule and Breach Notification Rule11 to protect sensitive patient health information (PHI). Viz.ai used a secure end-to-end process, securing PHI at both the hospital firewall and cloud Advanced Wireless Services network (https://k21academy.com/amazon-web-services/aws-solutions-architect/networking-fundamental/), with biometric, multifactorial access and a secure de-identification process. Viz.ai shared Customer Data in accordance with the Customer Agreement and in compliance with applicable law and legal process. The analysis of de-identified data does not constitute human subject research as defined at 45 CFR 46.102 (https://www.ecfr.gov/current/title-45/subtitle-A/subchapter-A/part-46/subpart-A/section-46.102) and therefore did not require institutional review board review.12
Patient-Related Variables
We divided patients’ ages into 4 groups: younger than 40 years, 40–59 years, 60–79 years, and 80 years of age or older. Two measures of stroke severity were used, defined by 2 imaging parameters on CTP: time-to-maximum (Tmax) > 6 seconds and regional cerebral blood flow (rCBF) < 30%. For both parameters, patients were divided into 4 groups based on the affected volume as 0 mL, 1–30 mL, 31–60 mL, 61–90 mL, 91–119 mL, and ≥120 mL. Imaging data included automatically calculated volumes of rCBF of <30% and hypoperfusion from CTP data. Hypoperfusion volume, which corresponds to areas of the brain that are critically hypoperfused regardless of reversibility, is estimated within Viz.ai as regions with Tmax of the residue function of >6 seconds.
Contrast Media Used
The contrast source information was based only on studies in which contrast media could be identified on the basis of DICOM information. The contrast agent information was calculated from the Contrast/Bolus Agent Attribute DICOM tag (0018,0010) in which Omnipaque and iodixanol (Visipaque) agents counted as GE Healthcare contrast agents and iopamidol (Isovue; Bracco Diagnostics) and ioversol (Optiray; Guerbet) counted as non-GE Healthcare contrast agents. Only 16 institutions (4% of total institutions in the analysis) used both GE Healthcare and non-GE Healthcare contrast, and only 3 institutions had >20 patients and used the alternate contrast in >10% of the total patients. The data were too small to be analyzed as a separate group, and institutions were classified on the basis of the predominant contrast used.
Hospital Characteristics
The hospitals were divided into Comprehensive Stroke Centers, Primary Stroke Centers, Thrombectomy-Capable Stroke Centers, and Acute Stroke Ready Hospitals according to definitions provided by The Joint Commission.13 Both Comprehensive Stroke Centers and Thrombectomy-Capable Stroke Centers are required to perform 15 mechanical thrombectomies during the past 12 months (or 30 during past 24 months), but a Comprehensive Stroke Center is additionally required to treat 20 patients with subarachnoid hemorrhage, perform endovascular or surgical treatment for 15 patients with intracranial aneurysms, and administer IV thrombolytics 25 times annually.
Additional Variables
Large-Vessel Occlusion Alert.
The large-vessel occlusion (LVO) alert feature is based on automated detection of LVO located in the ICA and the MCA (M1 and M2 segments).
Data and Statistical Analysis
Outcome data were measured as daily counts of patients per hospital who underwent CTA for acute ischemic stroke using the Viz.ai platform, including all hospitals. The percentage decline was calculated from the ratio of daily counts of patients per hospital before and after April 19, 2022, as well as for each individual month prior (March) and after (May, June, and July) that date. We performed a subgroup analysis of hospitals that perform CTPs for acute ischemic stroke using the Viz.ai platform. We used the Mann Kendall test for trend to determine statistical significance. The data in various strata defined by patient characteristics (age, sex, stroke severity), hospital characteristics (Primary or Comprehensive Stroke Centers, Thrombectomy-Capable, or Stroke Ready Centers), and contrast media used (GE Healthcare and non-GE Healthcare) were plotted on a weekly basis from February 28, 2022, through July 10, 2022.
RESULTS
We analyzed the anonymized data on 72,514 patients (including 79,053 studies) who underwent imaging processed with Viz.ai software in a sample of 399 hospitals in the United States from February 28, 2022, through July 10, 2022 (Online Supplemental Data). The daily counts of individual patients who underwent CTAs decreased (a 9.6% reduction, P = .002) from 1.584 studies per day per hospital before April 19, 2022, to 1.433 studies per day per hospital after April 19, 2022. The daily counts of individual patients who underwent CTA decreased from 1.585 studies per day per hospital in March to 1.427 studies per day per hospital in May, 1.408 studies per day per hospital in June, and 1.367 studies per day per hospital in July (Fig 1A). The lowest CTA count was 3798 individual patients observed between June 6 and 12. A significant reduction in CTAs performed was seen in patients 40–59 years of age (P < .001), 60–79 years of age (P < .001), 80 years of age or older (P = .002), but not in those younger than 40 years of age (P = .09) (Online Supplemental Data).

The weekly trend in daily counts of unique patients undergoing the study is presented. CTA (A) and CTP (B).
The daily counts of individual patients who underwent CTPs decreased (a 25.9% reduction, P = .003) from 0.484 studies per day per hospital before April 19 to 0.358 studies per day per hospital after April 19 in 185 hospitals that performed CTPs. The daily counts of individual patients who underwent CTP decreased from 0.484 studies per day per hospital in March to 0.346 studies per day per hospital in May, 0.333 studies per day per hospital in June, and 0.350 studies per day per hospital in July (Fig 1B). The lowest CTP count was 367 individual patients observed between May 23 and 29. A significant reduction in CTPs performed was seen in patients with Tmax values of zero (P = .004), <30 mL (P = .004), and 90–119 mL (P = .003), but not in those with values of 31–60 mL (P = .14), 61–90 mL (P = .85), and >120 mL (P = .62). A significant reduction in CTPs performed was seen in patients with rCBF values of zero (P = .007), <30 mL (P = .04), and 61–90 mL (P = .04), but not in those with values of 31–60 mL (P = .16), 90–119 mL (P = .52), and >120 mL (P = .47).
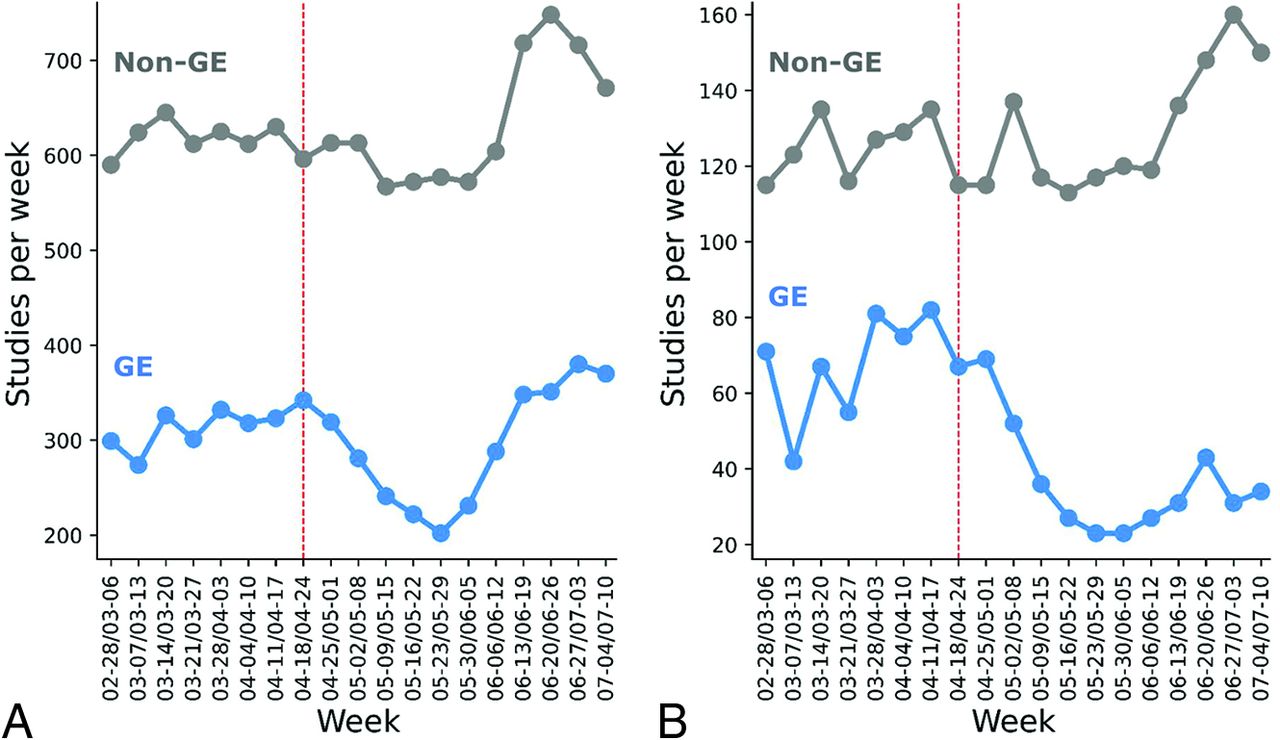
A nonsignificant reduction in CTAs using GE Healthcare contrast media was seen (12.42%, P = .32) but was not seen in CTAs using non-GE Healthcare contrast media (2.11%, P = .55) before and after April 19 in an analysis of data from 99 hospitals that provided the manufacturer of contrast media (Fig 2A). A significant reduction in CTPs using GE Healthcare contrast media (43.06%, P < .001) was seen but not in CTPs using non-GE Healthcare contrast media (increased by 2.93%, P = .29) (Fig 2B). Among hospitals that used GE Healthcare contrast media, the daily counts of individual patients who underwent CTA decreased (a 25.06% reduction) in May from 0.550 studies per day per hospital in March to 0.412 studies per day per hospital in May. Among hospitals that used non-GE Healthcare contrast media, the daily counts of individual patients who underwent CTAs decreased (a 11.40% reduction) in May from 1.062 studies per day per hospital in March to 0.941 studies per day per hospital in May.

The weekly trend in daily counts of unique patients undergoing the study is presented according to manufacturer of contrast media used, CTA (A) and CTP (B). GE indicates GE Healthcare.
The daily counts of individual patients who underwent CTA decreased in Comprehensive Stroke Centers (a 11.36% reduction, P = .027) and Primary Stroke Centers (a 11.57% reduction, P < .001) but not in Thrombectomy-Capable Stroke Centers or Acute Stroke Ready Hospitals (a 2.27% decrease, P = .72, and a 1.86% increase, P = .48, respectively) before April 19 to after April 19 in an analysis of data from 130 hospitals, which provided certification status. The daily count of individual patients who underwent CTP decreased in Primary Stroke Centers (40.39%, P = .004) and Comprehensive Stroke Centers (31.94%, P = .004), with a nonsignificant increase in Acute Stroke Ready Hospitals (17.14%, P = .48) and Thrombectomy-Capable Stroke Centers (11.11%, P = .056).
In Comprehensive Stroke Centers, the daily counts of individual patients who underwent CTA decreased (a 17.32% reduction) from 4.043 studies per day per hospital in March to 3.343 studies per day per hospital in May (Fig 3A). The daily counts of individual patients who underwent CTA in June, 3.669 studies per day per hospital, and July, 2.404 studies per day per hospital, remained lower than in March. A corresponding pattern appears in CTPs in these centers with a 42.71% reduction in May, from 0.924 studies per day per hospital in March to 0.534 studies per day per hospital in May. The daily counts of individual patients who underwent CTP in June, 0.628 studies per day per hospital, and July, 0.615 studies per day per hospital, remained lower than in March (Fig 3B).

The weekly trend in daily counts of unique patients undergoing the study is presented according to type of hospital. CTA (A) and CTP (B).
Overall, 6260 studies had alerts (positive LVO detection), and 72,793 studies did not have alerts. The proportion of patients with LVO alerts (ICA, M1 or M2) among those undergoing CTA did not change before and after April 19 (7.82% versus 7.98%, P = .054). However, the daily counts of individual patients with LVO decreased (a 7.69% reduction) from 0.124 per day per hospital before April 19 to 0.114 per day per hospital after April 19. The daily counts of individual patients with LVO in March (0.125 per day per hospital) remained higher than in May (0.112 per day per hospital) and June (0.110 per day per hospital); however, they increased in July (0.129 per day per hospital) (Fig 4). The proportions of patients with LVO alert according to hospital type before and after April 19 was as follows: Comprehensive Stroke Centers (9.47% and 9.75), Primary Stroke Centers (7.4% and 7.17%), Thrombectomy-Capable Stroke Center (8.68% and 7.82%), and Stroke Ready Hospitals (6.61% and 7.53%). Among patients who underwent CTP, the LVO alert rate increased from 12.56% to 16.09% after April 19 without any disproportionate changes in strata defined by CTP parameters of Tmax > 6 seconds and rCBF of <30% (Online Supplemental Data).

The weekly trend in daily counts of unique patients with LVO alert is presented. CTA (A) and CTP (B).
DISCUSSION
Our analysis provides a quantitative estimate of the effect of contrast media shortage on the performance of CTA and CTP in patients with acute ischemic stroke derived from a large sample of health care systems in the United States. The daily counts of individual patients who underwent CTA decreased (a 9.6% reduction) after April 19. The magnitude of reduction was smaller than expected, presumably because many facilities routinely store variable amounts of GE Healthcare contrast media. There was also the availability of products by other contrast media suppliers such as iohexol and iopamidol and GE Healthcare’s ability to provide approximately 20% of the demand.2 Furthermore, increased use of unenhanced imaging or alternate tests such as MR imaging and ultrasound for other body systems preserving contrast for CTA and CTP and use of reduced contrast media volume in CTA and CTP in patients with acute ischemic stroke may have resulted in a smaller (than expected) magnitude of reduction.6,8 Although the reduction in daily counts of individual patients undergoing CTA was seen immediately after April 19, the reduction in daily counts of individual patients undergoing CTP was not seen until the middle of May, suggesting that the reductions on various components of multimodal CT evaluations were not the same. The daily counts of individual patients undergoing CTA or CTP demonstrated an increase in counts toward the end of June, but the counts remained well below the counts seen before April 19. The lag in recovery was seen despite GE Healthcare reporting that production was up to 60% of baseline production by May 21, 2022, and up to 100% by June 8, 2022,14 and may be attributable to delays in distribution chains and/or continuation of acute stroke imaging protocols in institutions that avoided use of contrast media–based CTA and CTP.
The reduction in daily counts of individual patients undergoing CTA was consistent in various strata defined by the patient’s age, with possibly a lesser reduction in patients younger than 40 years of age. There appeared to be a greater reduction in CTP in patients with either rCBF < 30% or Tmax > 6-second volume of zero or <30 mL. These parameters correlate with minor or resolving neurologic deficits,15,16 indicating that patients with ischemic strokes with minor deficits or those with TIAs were less likely to undergo CTPs during the period of contrast media shortage. The selective exclusion of patients with minor or resolving neurologic deficits from undergoing CTP appears to be one of the strategies to reduce the need for contrast because these patients are unlikely to be candidates for endovascular treatment.3
Reductions in daily counts of individual patients undergoing CTA and particularly CTP using GE Healthcare contrast media was seen but not in daily counts of individual patients undergoing CTA and CTP using non-GE Healthcare contrast media. There was an increase in daily counts of individual patients undergoing studies using non-GE Healthcare contrast media by late June to greater counts than those before April 19, suggesting that more institutions may have started using non-GE Healthcare contrast media to avoid any future reductions in supply. Overall, non-GE Healthcare contrast media was more commonly used in a study sample of hospitals before April 19, which may have reduced the overall impact of the contrast media shortage.
When stratified on the basis of the characteristics of hospitals, the reduction in daily counts of individual patients undergoing CTA and CTP was highest in Comprehensive Stroke Centers and Primary Stroke Centers. An important part of this magnitude of reduction was the much larger volume of studies performed in Comprehensive Stroke Centers. Comprehensive Stroke Centers have a large proportion of patients undergoing interventional procedures requiring contrast media, which may result in contrast media availability for the performance of CTA.17,18 Comprehensive Stroke Centers are usually based in larger hospitals with competing needs for contrast media–based imaging studies for patients with trauma and cardiac disease.19,20 The reduction in CTAs and CTPs at Comprehensive Stroke Centers may be partly attributed to more effective triage of patients with acute ischemic stroke, including the use of prehospital LVO-detection tools, transport paradigms, in-hospital workflows, acute stroke neuroimaging protocols, and angiography suite workflows.21 Comprehensive Stroke Centers may have greater access to emergent MR imaging and cerebral angiography, allowing substitution of or bypassing CTA and CTP for emergent neuroimaging in patients with acute ischemic stroke.
We did not identify any differences in the proportion of patients with LVO alerts among those undergoing CTA before or after April 19, despite the reduction in CTAs performed. The daily counts of individual patients with LVO alerts in March (0.125 per day per hospital) was higher than that seen in May (0.112 per day per hospital) and June (0.110 per day per hospital). The possibility of suboptimal detection of LVOs and adverse effects on the quality of care is not supported by single-center studies.9,22 We cannot further analyze this possibility because the total number of patients with acute ischemic stroke presenting to the hospitals was not available, preventing us from determining the fraction of patients with acute ischemic stroke undergoing CTA before and after April 19. We found a greater reduction in daily counts of individual patients undergoing CTA among patients with less severe strokes (based on imaging criteria), also suggesting that patients at lower risk of LVO were selectively excluded from CTA. If we were to assume that only patients at a higher risk of LVO after initial screening based on clinical criteria and noncontrast CT were undergoing CTA and CTP, the proportion of LVO alerts should be higher. Therefore, it is more likely that other imaging modalities substituted for CTA and CTP.23⇓-25
There are several issues that require consideration before interpretation of the findings. The sample is based on all the 399 hospitals that use the Viz.ai imaging platform. The results presented here may not be reflective of practices at those hospitals that use the alternate Rapid.AI platform (https://www.rapidai.com/about)26,27 or do not use any imaging software despite CTA acquisitions. Several analyses such as those for reduction in daily counts of individual patients undergoing CTA according to the manufacturer of contrast media were performed on a smaller sample of patients. The comparison between CTA and CTP performed before and April 19 was restricted to the year 2022. A comparison with the same time period in 2021 was not reliable because the number of hospitals using the Viz.ai platform had increased and we could not adjust for differences in hospital number and characteristics in such a comparison. The short period of observation before contrast media shortage reduces the data available for analysis, subsequently reducing the power of the study and increasing the margin of error,28 and reducing the inability to exclude seasonal fluctuations in the incidence of acute ischemic stroke.29 The LVO alert and quantitation of infarction volume and hypoperfusion were based on using an automated algorithm, which has been previously validated.30,31 In an analysis of 650 CTAs performed in patients with acute ischemic stroke,30 Viz.ai demonstrated a sensitivity of 82%, specificity of 94%, positive predictive value of 77%, and negative predictive value of 95% for the detection of LVO compared with an independent neuroradiologist’s interpretation. In another analysis of 2544 CTAs performed in patients with acute ischemic stroke in 139 US hospitals,31 Viz.ai demonstrated a sensitivity of 96% and specificity of 94% for the detection of LVO compared with an independent radiologist’s interpretation.
However, we acknowledge that detection of LVOs was not based on the interpretation of an independent neuroradiologist in our study and cannot exclude the possibility of false-positive and false-negative alerts. The anonymized data used in the analysis do not provide any access to patient records and other imaging modalities used. We were unable to document the magnitude of increase in the use of other imaging or diagnostic approaches (such as MR imaging) during the study period. We were also unable to determine whether there were changes in the criteria for selecting patients for CTA and CTP after April 19 and whether there were any differences in quality indicators such as in the time interval between hospital arrival and endovascular treatment or in patient outcomes. We were also unable to assess whether institutions changed the dose of contrast media administered and used a lower dose after April 19. A single-center study9 did not identify any change in the rates of successful reperfusion, average time to recanalization, average radiation dose, and favorable outcome at discharge before and after the contrast media shortage. We also acknowledge that mitigation strategies at institutions may be dynamic and various strategies (as mentioned earlier) may have been used at different time points. We are also unable to comment on the effect of the contrast media shortage on CTA performed for other indications such as for detection of intracranial aneurysms or traumatic vascular injuries.
CONCLUSIONS
Our analysis reported changes in the use of CTA and CTP in patients with acute ischemic stroke and identified some of the factors that influenced the change in use during contrast media shortage. Future studies should go into greater depth in studying the contrast media shortage–related changes with particular emphasis on the effect on the quality of care and patient outcomes. Several strategies were implemented in various institutions during the contrast media shortage, including increased use of alternate tests such as MR imaging, reducing contrast media volume, and increased reliance on clinical criteria and noncontrast CT scans.6,8,9 Data accrued during the period of contrast media shortage may help in identifying effective strategies to reduce reliance on contrast media–based studies such as CTA and CTP23 without compromising patient outcomes.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received November 10, 2022.
- Accepted after revision May 31, 2023.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}