
Abstract
BACKGROUND AND PURPOSE: Medullary tegmental cap dysplasia is a rare brainstem malformation, first described and defined by James Barkovich in his book Pediatric Neuroimaging from 2005 as an anomalous mass protruding from the posterior medullary surface. We describe the neuroimaging, clinical, postmortem, and genetic findings defining this unique malformation.
MATERIALS AND METHODS: This is a multicenter, international, retrospective study. We assessed the patients’ medical records, prenatal ultrasounds, MR images, genetic findings, and postmortem results. We reviewed the medical literature for all studies depicting medullary malformations and evaluated cases in which a dorsal medullary protuberance was described.
RESULTS: We collected 13 patients: 3 fetuses and 10 children. The medullary caps had multiple characteristics. Associated brain findings were a rotated position of the medulla, a small and flat pons, cerebellar anomalies, a molar tooth sign, and agenesis of the corpus callosum. Systemic findings included the following: polydactyly, hallux valgus, large ears, and coarse facies. Postmortem analysis in 3 patients revealed that the cap contained either neurons or white matter tracts. We found 8 publications describing a dorsal medullary protuberance in 27 patients. The syndromic diagnosis was Joubert-Boltshauser syndrome in 11 and fibrodysplasia ossificans progressiva in 14 patients.
CONCLUSIONS: This is the first study to describe a series of 13 patients with medullary tegmental cap dysplasia. The cap has different shapes: distinct in Joubert-Boltshauser syndrome and fibrodysplasia ossificans progressive. Due to the variations in the clinical, imaging, and postmortem findings, we conclude that there are multiple etiologies and pathophysiology. We suggest that in some patients, the pathophysiology might be abnormal axonal guidance.
ABBREVIATIONS:
- AMCD
- anterior mesencephalic cap dysplasia
- BPAN
- β propeller protein-associated neurodegeneration
- CC
- corpus callosum
- FOP
- fibrodysplasia ossificans progressive
- INAD
- infantile neuroaxonal dystrophy
- JBTS
- Joubert-Boltshauser syndrome
- MTCD
- medullary tegmental cap dysplasia
- PTCD
- pontine tegmental cap dysplasia
- TOP
- termination of pregnancy
Medullary tegmental cap dysplasia (MTCD) is a rare brainstem malformation, first described and defined by James Barkovich1 in his book Pediatric Neuroimaging from 2005, as an anomalous mass protruding from the posterior medullary surface. MTCD shares common features with 2 other brainstem malformations, both suspected to result from impaired axonal guidance or abnormal neuronal migration: pontine tegmental cap dysplasia (PTCD, Online Mendelian Inheritance in Man [OMIM] No. 614688) and anterior mesencephalic cap dysplasia (AMCD).2⇓-4 In all 3, there is an abnormal “cap” protruding from the brainstem, located anteriorly in AMCD and posteriorly in PTCD and MTCD.3,5 A mass protruding from the dorsal medulla has also been described in Joubert-Boltshauser syndrome (JBTS) and in fibrodysplasia ossificans progressiva (FOP) syndromes, but never defined as MTCD.
In a teaching neuroimage paper previously published, the MR images showed an anomalous mass of gray matter signal intensity protruding from 1 side of the medulla, a hypoplastic pons and thickened medulla oblongata, a dysplastic cerebellum, and partial agenesis of the corpus callosum (CC).6
Following the presentation of a prenatal diagnosis of MTCD in 2 fetuses at the meetings of the International Research Consortium for the Corpus Callosum and Cerebral Connectivity and Neuro-MIG Cost Action project, we collected a total of 13 patients (3 fetuses and 10 children).
We describe the neuroimaging, clinical, postmortem, and genetic findings defining this unique brainstem malformation.
MATERIALS AND METHODS
This is a multicenter international retrospective study (Israel, France, Switzerland, Spain, the Netherlands, Germany, United States). Patients with a dorsally protruding mass from the medulla were extracted from personal teaching files of neuroradiologic colleagues across the globe. We assessed the medical records, prenatal ultrasounds, MR images, genetic findings, and postmortem results of the patients. We reviewed the medical literature for all studies describing medullary malformations and evaluated the cases in which a dorsal medullary protuberance was described.
The study was approved by the Wolfson Medical Center’s institutional review board [WOMC-0188–18].
Imaging Techniques
Fetal neurosonograms were obtained according to the International Society of Sonography in Obstetrics and Gynecology guidelines.7,8 The examinations were performed on Voluson E8 and E10 ultrasound machines (GE Healthcare, Kretz Sonography) using transabdominal and transvaginal probes or an Aplior i800 U (Canon Medical Systems).
MR imaging brain scans, fetal or postnatal, were obtained in all cases. Fetal MR imaging (Sigma Horizon LX and EchoSpeed MR imaging scanners, 1.5T; GE Healthcare) scans were obtained using an ultrafast, T2-weighted single-shot fast spin-echo MR imaging in the axial, coronal, and transversal planes (acquisition time = 40–45 seconds). During fetal scans, patients received oral diazepam and zopiclone, 7.5 mg, before the MR imaging to reduce fetal and maternal movements for imaging. In postnatal scans, the same sequences were used in addition to FLAIR and STIR.
MTCD Characterization.
The cap was characterized on the midsagittal plane by the authors Prof. Tally Lerman-Sagie and Prof. Eugen Boltshauser. The cap was described according to its shape (Fig 1), size in relation to the medulla (anterior-posterior diameter in the midsagittal plane), craniocaudal extension (pontomedullary, medullary, low medullary), axial projection (unilateral, bilateral), relation to the cerebellar peduncles (connected, separated, or unknown), and signal intensity (Online Supplemental Data).

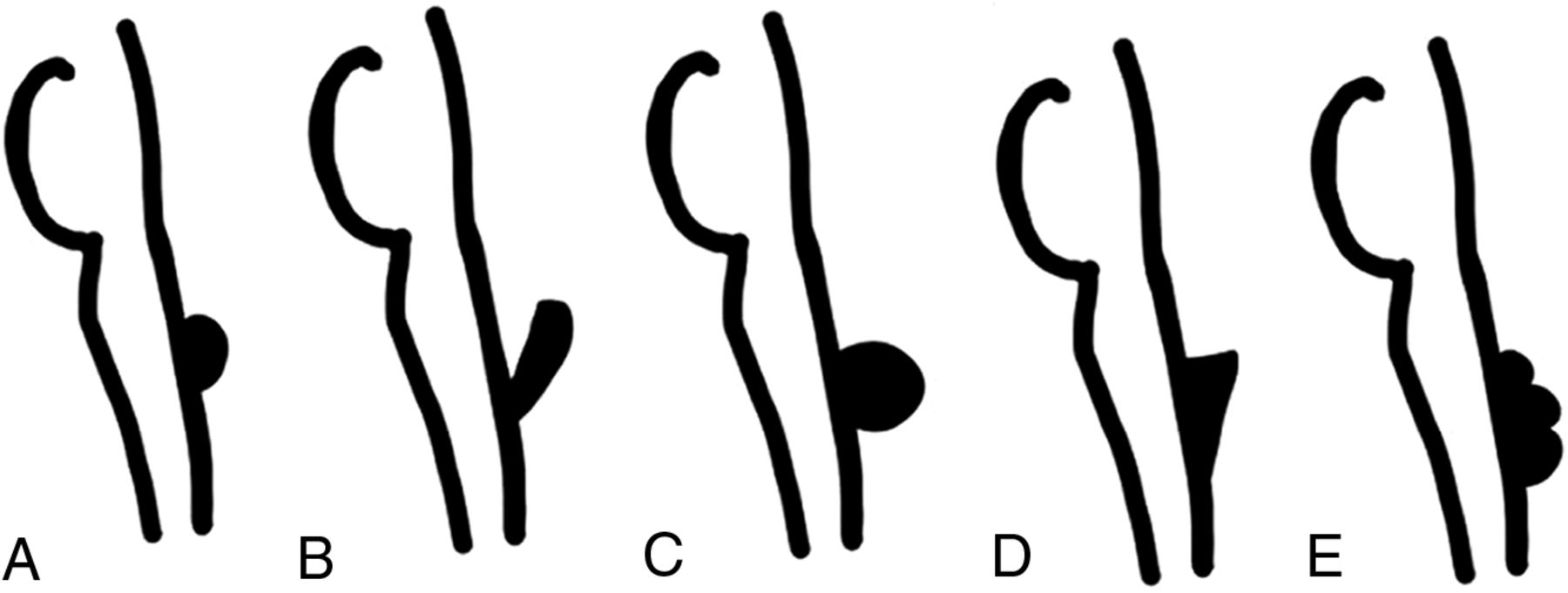
Illustration of the medullary cap morphologic characteristics: A, Smooth; B, Stick sign; C, Globular; D, Step sign; E, Caterpillar sign.
We defined 5 distinct shapes (Fig 1):
Smooth: the cap borders blend into the medulla, and the contour is smooth (Fig 2E).
Stick sign: the cap is thin and elongated (Fig 2F).
Globular: the cap is round (Fig 2A).
Straight-angled, “step sign”: there is a straight angle between the cap and the medulla (Fig 2D).
Tuberal, “caterpillar sign”: the cap consists of multiple tuber-like protuberances (Fig 2K).
Postmortem Examinations
Postmortem examinations were performed according to protocols previously described and included a detailed examination of the fetus and placenta.9 For gross examination of the brain, the brainstem was separated from the cerebral hemispheres by a section at the level of the midbrain. The cerebral hemispheres were bisected along the midsagittal plane. The separate hemispheres were placed back together, followed by coronal sectioning of the cerebral hemispheres. The brainstem and cerebellum were sectioned along the axial plane. Histologic sections 4-μm-thick were prepared and stained with H&E. The histologic sections were examined along with the corresponding gross photographs. Immunohistochemical stains for calretinin and synaptophysin were performed as indicated.9
Data Availability
Anonymized imaging data not published within this article will be made available by request from any qualified investigator.
RESULTS
The study included 13 unrelated patients: 3 fetuses (diagnosed at 17, 21, and 32 weeks of gestation), and 10 children and adolescents (9 months to 18 years of age at the latest clinical follow-up). All pregnant couples opted for termination of pregnancy (TOP) according to the national laws, allowing TOP in cases with imaging findings implying a high risk of severely impaired neurodevelopmental outcome. Two children died in infancy following an infection. Eight patients are alive.
We found 8 publications describing a dorsal medullary protuberance in 27 patients. The syndromic diagnosis was JBTS in 11 and FOP in 14 patients.1,6,10⇓⇓⇓⇓-15
Clinical Features
A clinical evaluation extracted from the medical charts was available in only 9 of our 10 patients (all 3 pregnant couples opted for TOP), as detailed in the Online Supplemental Data. Patients’ ages ranged between 6 months and 18 years at diagnosis, with 3 females and 5 males (in 5 patients the sex was unknown). Cognitive function was normal in 4 patients, 2 patients had severe global developmental delay, 1 patient was in the low-average range, and 3 patients had no information. Delayed motor milestones were observed 5 patients, of whom 3 had severe and 1 had mild developmental delay, and 1 had left hemiparesis.
Two patients presented with central apneic episodes. Neurologic examination findings were normal in 3 patients and abnormal in 5 patients, including axial hypotonia and normal reflexes in patient 1; hypotonia, dysarthria, strabismus, nystagmus in patient 7; left hemiparesis in patient 8; patient 9, had no eye contact/tracking, abnormal movement, self-mutilation, and exclusive gastrostomy, and in patient 10, with no eye contact, hyperkinetic limb movements, and hypotonia. Neurologic examination was unavailable in 5 patients. Two patients had cutaneous skull lesions. Three patients were diagnosed with JBTS. Bilateral hallux valgus (diagnosed with FOP), vocal cord paresis, and hematologic disorders with hepatic cholestasis were observed in 1 patient each. Two patients died, one from cardiac arrest following a respiratory infection at 9 months and the other from coronavirus disease 2019 (COVID-19) infection, at 11 months.
Neuroimaging Findings
The imaging findings of our 13 patients and all those previously described in the literature (27 patients) are detailed in the Online Supplemental Data.
Main Features According to the Anatomic Structure
Medulla Oblongata.
Cap morphology (illustrated in Fig 1) was smooth in 1/13 and 16/27, globular in 5/13 and 0/27, step sign in 6/13 and 9/27, stick sign in 3/13 and 0/27, and caterpillar sign in 3/13 and 5/27 patients.
Cap size in relation to the medulla was smaller 1/13 and 15/27 patients, equal in 7/13 and 9/27, and larger in 5/13 patients (in 1 patient, the cap was extremely enlarged and resembled a tumor, Fig 2L).
Craniocaudal extension was midmedullary in 5/13 and 2/27 patients, lower medullary in 8/13 and 9/25 patients (no information was available in 2 patients), and pontomedullary in 0/13 and 14/27 patients.
Axial projection was unilateral in 4/13 (unknown in 5) and 9/27 and bilateral in 11/27 patients (in the 13 patients described by Severino et al,14 axial projection varied).
The relation to the cerebellar peduncles was connected to the cerebellar peduncles in 1/13 and 1/27, and separated from the cerebellar peduncles in 10/13 and 22/27.
Signal intensity was equal to the medulla in 11 patients and different in 2. In the literature, signal intensity was equal in 22 patients, 2 had gray matter intensity, and FLAIR signal intensity was increased in 13 patients (Online Supplemental Data).
The midbrain was abnormal in 1/40; the pons, in 9/40; and the cerebellum, in 20/40 patients. Details of the abnormal CNS findings are found in the Online Supplemental Data.
Regarding posterior fossa anomalies, there was a hypoplastic vermis in 11 patients from the literature10⇓⇓-13 and in 6 of our patients (patients 1, 3, 5, 9, 11, and 12) and an oversized vermis in 2 patients from the literature.1,6 Cerebellar malformations including hemisphere hypoplasia and dislocated fastigium were observed in our cohort in 1 patient each. A total of 3 patients from our cohort (patients 9, 11, and 12) and 11 patients from the literature had a diagnosis of Joubert syndrome.10⇓⇓-13
An anomaly of the CC was found the original description by Barkovich,1 the neuroimage by Jurkiewicz and Nowak,6 and in 4 patients from our cohort (patients 1, 2, 4, and 10).
Sulcation was abnormal in 2 of our 13 patients.
Other anomalies included ventriculomegaly, frontoparietal interhemispheric cyst, and peritrigonal focal white matter abnormalities in 1 patient each from our cohort.
Genetic Findings
The genetic investigation included the following: karyotype (1/13), chromosomal microarray (5/13), exome sequencing (5/13), genome sequencing (3/13), and targeted gene analysis (1/13) (Online Supplemental Data). Chromosomal microarray in patient 5 revealed a paternally inherited 15q21.2 deletion, which included part of the GLDN gene. Targeted analysis of the ACVR1 gene was performed in patient 1 due to hallux valgus and revealed the classic p.Arg206His mutation. Patient 9 had an anomaly of the entire short arm of chromosome 11 in mosaicism, consistent with Beckwith-Wiedemann syndrome. Patient 11 had a CSPP1 gene mutation and was diagnosed with JBTS.
Postmortem Analysis
A postmortem examination was available in 2 of the 3 fetuses that underwent TOP (Fig 3) and in 1 of the postnatal cases.

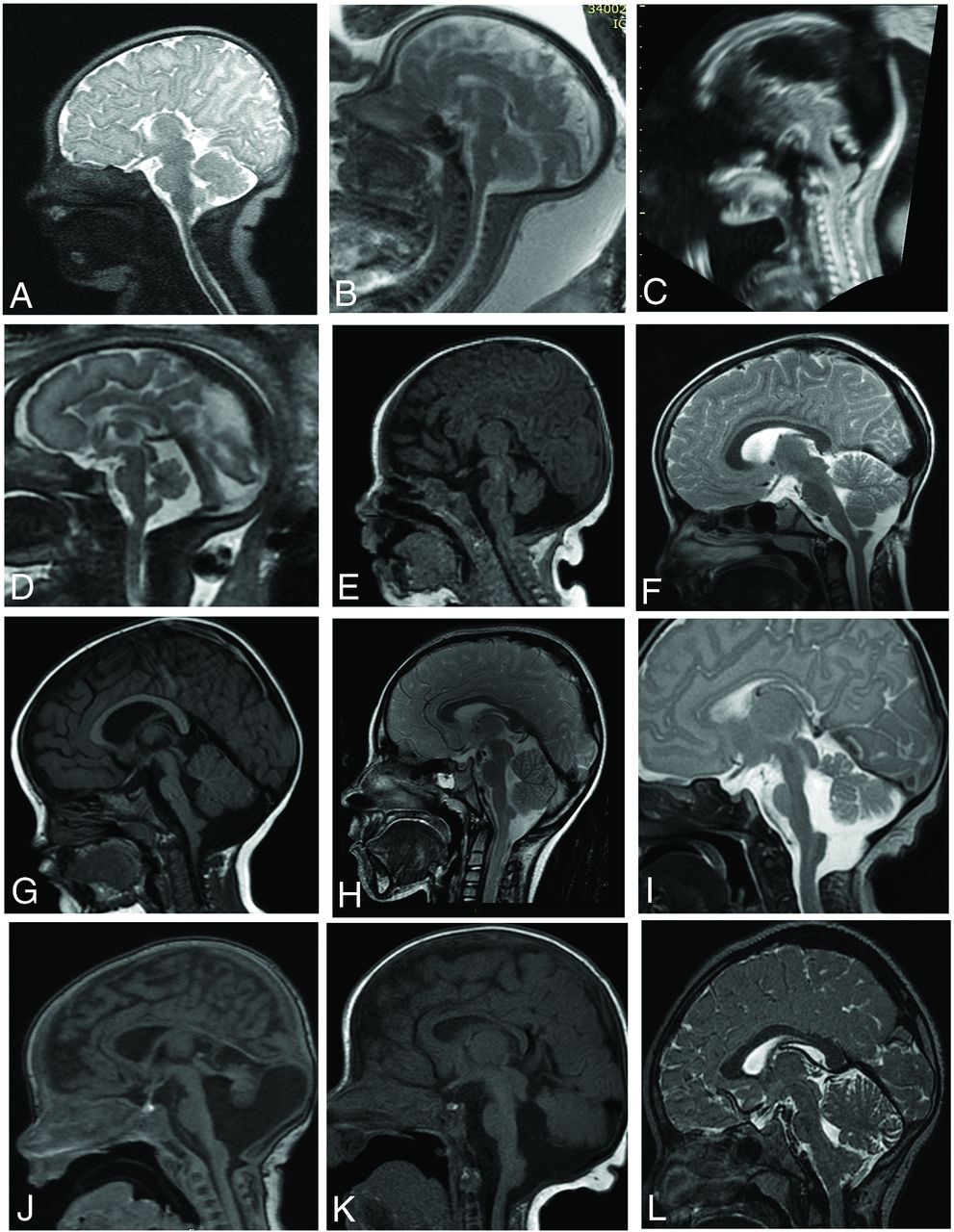
MR imaging and ultrasound showing the medullary cap in 12 patients, midsagittal view. A, Patient 1; B, Patient 2; C, Patient 3; D, Patient 4; E, Patient 5; F, Patient 6; G, Patient 7; H, Patient 8; I, Patient 9; J, Patient 11; K, Patient 12; L, Patient 13. Of note, patient 10’s MR imaging is separately shown in the Online Supplemental Data.

A, Axial microscopy photograph of the medulla oblongata of patient 2 at 35 gestational weeks. The right-posterior bulge of the medulla oblongata (RMO) contains many mature neurons, consistent with a hamartoma, connected to the cerebellum. The inferior olivary nuclei (ON) are well-developed, and the pyramidal tracts (PT) are intact. B, Postmortem photograph of patient 3 depicts the fetal posterior fossa after removal of the occipital bone, performed at 17 gestational weeks. Note the thickening and internal rotation of the RMO, producing the medullary cap shape. Cbl indicates cerebellum; FM, opening of the foramen of Magendi.
In patient 2, the macroscopic evaluation revealed a mass protruding from the dorsolateral right side of the medulla. The ventral pons was hypoplastic on the right. The right inferior peduncle was thickened relative to the other side. Microscopically, the mass contained many mature neurons that could be consistent with a hamartoma. The inferior olivary nuclei were well-developed, and the pyramidal tracts were intact. Few neurons were seen in the pons; the transverse and pyramidal tracts were observed. The cerebellar cortex was normal (Fig 3A), as well as the rest of the brain and organs.
In patient 3, the macroscopic evaluation showed a wide interhemispheric space; an asymmetrically rotated medulla oblongata with a posterior mass protruding on the right from the dorsolateral aspect; agenesis of the CC; and ventricular asymmetry. The medial part of the cortex in the left hemisphere was thicker than on the right, with an irregular structure with multiple sulcations (Fig 3B). Microscopic evaluation disclosed asymmetry of the medulla due to the occupying white matter. In the occipital lobe of the left hemisphere, an area of polymicrogyria with cortical disorganization was noted.
In patient 10, postmortem examination revealed that the hypersignal on the dorsal surface of the brainstem corresponded to spheroids in the posterior tracts of the medulla, in favor of a neuroaxonal dystrophy.
DISCUSSION
James Barkovich1 was the first to describe this unique brainstem malformation, MTCD, in 2005, and included it in the classification of midbrain-hindbrain malformations in 2009.16 It was described as a dorsal medullary protuberance identified on MR imaging in infants being imaged for multiple anomalies of the musculoskeletal, genitourinary, or gastrointestinal systems. On sagittal images, a dorsal (tegmental) cap was seen at the level of the medulla, associated with absence or severe hypogenesis of the corpus callosum.
No additional patients with MTCD were described in the literature until 2015, when Jurkiewicz and Nowak6 supplied MR images of this brainstem anomaly in Neurology. They described a 3-year-old boy who presented with respiratory distress and apnea. MR imaging showed a hypoplastic pons and thickened medulla oblongata with an anomalous mass of gray matter signal intensity around it.
To the best of our knowledge, MTCD has not been defined in any other cases in the literature, however, when searching the literature for medullary anomalies, we found 27 cases fulfilling the definition of an anomalous mass protruding from the posterior medullary surface.
We analyzed our 13 cases and the additional 27 cases from the literature for the characteristics of the cap, additional findings, clinical presentation, postmortem results, and genetic evaluation. We discovered that the dorsal medullary cap is not a single entity but has different characteristics: shape, size, signal intensity, craniocaudal location, laterality, and relation to the cerebellar peduncles (Online Supplemental Data). Furthermore, the etiology was diverse, there were specific additional CNS or systemic findings, and there was a range of clinical presentations, from no symptoms to profound developmental delay.
The clinical presentation of the patients with MTCD was considerably variable. Some patients did not have neurologic involvement at all. Patients with FOP (ACVR1 mutations) had only skeletal anomalies. Patient 1 from our cohort with an ACVR1 mutation had normal development and hallux valgus typical of FOP.17 In patients 6 and 13, the MTCD was an incidental finding during a cutaneous skull lesion evaluation. It seems that the underlying symptoms are related to the syndromic diagnosis (as in patients with JBTS) or associated findings. Three patients presented with profound developmental delay (patients 5, 9, and 10), and 2 had early death (patients 5 and 10). Brainstem dysfunction is described in 3/13 patients (patient 5, vocal cord paresis; patients 9 and 11, apnea). Eight patients had other brainstem anomalies (Online Supplemental Data).
The child described by Jurkiewicz and Nowak6 also had absence of the middle and distal phalanges of the hands and feet, gastroesophageal reflux, hiatal hernia, abnormal findings on auditory brainstem response testing, and dysmorphic features including facial asymmetry, large dysplastic earlobes, and deep-set eyes.6 He presented with apnea at 3 years of age. Whether these presentations are related to the medullary tegmental cap dysplasia or the underlying genetic syndrome remains unknown. In the 2 other brainstem malformations that share a cap (protruding from the dorsal pons in PTCD and the anterior mesencephalon in AMCD), the cap always has a distinct shape: in PTCD an abnormal curved structure covering the middle third of the pontine tegmentum and projecting into the fourth ventricle,4,5 and in AMCD, a rounded bulging obliterating the interpeduncular fossa.3 In contrast, in MTCD, the cap has multiple shapes as depicted in Figs 1 and 2.
AMCD has been described in only 3 patients with JBTS.3 Clinically, the patients manifested typical features of this syndrome: hypotonia, developmental delay, ataxia, intellectual disability, and neuro-ophthalmologic signs.3 Two patients were compound heterozygous for TMEM67 missense variants.18
PTCD is not considered inherent in JBTS, but rather a distinct category, part of the “molar tooth” family of brainstem anomalies, due to its particular posterior fossa characteristics and associated CNS findings (subtotal absence of the middle cerebellar peduncles, flattened ventral pons, vaulted pontine tegmentum, a molar tooth aspect of the pontomesencephalic junction, an absent inferior olivary prominence, vermal hypoplasia, and corpus callosum hypoplasia or agenesis5) that differentiate it from the Joubert spectrum of disorders.19 Prenatal diagnosis of patients with PTCD has been previously described in 4 fetuses. In the 3 living children, global developmental delay and multiple cranial nerve impairment were observed. A genetic etiology of PTCD has not been found, and it is considered a sporadic disorder because no familial cases have been described.2,4,5,20
MTCD is also a unique category within the classification of midbrain-hindbrain malformations,16 but it has multiple etiologies and different forms and clinical presentations. JBTS is one of the possible etiologies.
Poretti et al10⇓-12 described a posterior medullary protuberance in 7 patients with JBTS; images consistent with MTCD were supplied in 2 studies. In our cohort, there were 3 patients with this diagnosis (patients 9, 11, and 12). In most of these cases, the cap had distinct features: It was straight-angled, tubular, equal in size with the medulla, and located in the low-medullary region. We suggest that the step sign and the caterpillar sign adequately describe the typical appearance of the cap in JBTS because it is straight-angled and in some cases reminiscent of a caterpillar clinging to a stem (Fig 1 and Fig 2I, -K).
The step sign is reminiscent of clava hypertrophy, a relatively consistent imaging finding in infantile neuroaxonal dystrophy (INAD)/PLA2G6 (OMIM No. 256600).21,22
Recently (2022), clava prominence has also been mentioned in 6/27 scans of patients with β propeller protein-associated neurodegeneration (BPAN).23 Distinction between JBTS and INAD or BPAN is not problematic from the clinical and the imaging perspective. Imaging in INAD shows almost consistent cerebellar atrophy and inconsistent cerebellar cortex hyperintensity, and BPAN shows intense iron deposition in the substantia nigra, while JBTS presents (in addition to the molar tooth sign) with vermis hypodysplasia and cranial dislocation of the fastigium, while cerebellar atrophy is not a feature.21,24,25 Patient 10 from our cohort had a progressive course, both clinically (postnatal progressive microcephaly, development of hyperkinetic movements, and so forth, Online Supplemental Data) and radiologically. Prenatal MR imaging showed partial agenesis of the CC and a small pons, with no MTCD, which was only diagnosed later on MR imaging performed at 11 months (Online Supplemental Data), suggesting that MTCD could sometimes develop progressively, for example, in neurodegenerative disorders. This patient was suspected clinically of having atypical neuroaxonal dystrophy, further supported by the presence of spheroids in the posterior tracts of the medulla. However, findings of whole-genome sequencing including mitochondrial DNA were normal.
Patient 11 from our cohort was diagnosed with JBTS and has a CSPP1 gene mutation, also reported in a patient with JBTS and an occipital encephalocele published by Tuz et al.13 In both cases, the cap shared similar characteristics: It was in the lower medulla and separated from the cerebellar peduncles, and the step and caterpillar signs were noted.
PTCD and AMCD are considered the result of aberrant axonal guidance. AMCD is part of the JBTS spectrum and is associated with the molar tooth sign, which is a hallmark of this syndrome.26⇓-28 PTCD differs from JBTS, in the imaging, clinical, and genetic aspects. A displaced decussation of the superior cerebellar peduncles is noted anteriorly-posteriorly in both AMCD and PTCD.2,3,20,29
Further supporting evidence is supplied by fiber tractography, which showed an abnormal transverse bundle of fibers in the pons forming the cap in PTCD2,20,29 and an ectopic white matter bundle in AMCD. In the patient described by Jurkiewicz and Nowak,6 tractography revealed no decussating pontine fibers nor crossing of the corticospinal tracts, also implying abnormal axonal decussation in this entity. Postmortem analysis of patient 3 confirmed abnormal pathways because there was a continuation of fibers between the medullary mass and the white matter of the cerebellum (Fig 3).
The pathogenesis of JBTS, hypothesized to cause AMCD as well, is a ciliary dysfunction.2,3,30,31 Primary cilium has a key role in modulating neurogenesis, cell polarity, and axonal guidance, all essential for wiring the developing brain. Disrupted ciliary signaling contributes to axonal tract malformations in JBTS.30⇓-32 In our cohort, the additional findings in some patients such as midline distortion, a rotated position of the medulla on axial planes, and CC agenesis/partial agenesis as well as clinical features like polydactyly might support the hypothesis that MTCD can also be caused by impaired ciliary function in at least some patients. Callosal anomalies have also been mentioned by Barkovich,1 Jurkiewicz and Nowak,6, and Barkovich et al.16
A de novo mutation in the ACVR1 gene was found in one of our patients (patient 1, Fig 2A, p.Arg206His). This gene plays an essential role in ciliary formation.32 ACVR1 deletion in mouse embryonic fibroblasts compromised ciliary development and resulted in defects in leftward fluid flow and, thus, abnormalities in left-right patterning.32 Mutations in ACVR1 cause FOP, an autosomal dominant disorder causing progressive heterotopic endochondral ossifications.14 In 2016, Severino et al14 described a well-defined nonenhancing lesion at the level of the dorsal medulla with variable morphology, ranging from a thin band of tissue to an exophytic mass, in 13 patients with FOP. All also showed thin tissue bands at the ventral pons. We have re-classified this lesion as MTCD.
The cap in FOP seems to display a distinct form; it is “soft,” smooth, and rather flat, and its position is exceptionally higher in most cases, reaching the midpons. The mass has been suspected to represent a hamartoma;14,15 however, a postmortem examination of a 75-year-old patient revealed that the cap consisted of glial hyperplasia.33
In patient 2 from our cohort, the postmortem examination in the fetus revealed that the mass contained mature neurons consistent with a hamartoma. In contrast, in patient 10, the postmortem examination at the age of 11 months revealed that the cap consisted of spheroids, a feature of axonal degeneration.34 In this patient, the medullary cap was present prenatally (retrospectively) but was much less prominent and was noticeable postnatally, possibly due to progressive atrophy of the tegmentum as demonstrated by sequential MR images at 33 weeks’ gestation, 1 month, and 11 months (Online Supplemental Data). Also, the resolution of fetal MR imaging is inferior to that of postnatal MR imaging. The clinical picture and postmortem examination were reminiscent of neuroaxonal dystrophy; however, findings of genetic studies were negative.
Our study has several limitations. The main limitation is its retrospective nature, an evaluation of patients that have been collected by several groups across the globe. Therefore, a true incidence cannot be established. In addition, imaging protocols may have varied, the clinical data were limited in some of the cases, and no high-end functional imaging data were available (ie, DTI, which may allow studying of the internal architecture of the cap).
The inclusion of patients with JBTS might have led to a selection bias because their MTCD characteristics are distinctly different from those in the rest of the cohort. Future studies are warranted and may answer these open questions.
Differential diagnoses of abnormal dorsal medullary masses, causing a distortion of the brainstem, are brainstem tethering or proliferative disorders (tumor and metastasis). Brainstem tethering can be excluded because the mass is longer and, unlike MTCD, connects the dorsal medulla to the inner surface of the occipital skull,35,36 and a proliferative disorder can be excluded on the basis of lack of infiltrative features and imaging characteristics.3
CONCLUSIONS
This is the first study to delineate a series of patients with the rare malformation medullary tegmental cap dysplasia. The cap has different shapes, distinct in JBTS and FOP. Due to the variations in the clinical, imaging, and postmortem findings, we conclude that there are multiple etiologies and pathophysiology. We suggest that in some of the patients, the pathophysiology might be abnormal axonal guidance.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received October 14, 2022.
- Accepted after revision January 9, 2023.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}