
Abstract
BACKGROUND AND PURPOSE: CSF-to-venous fistulas contribute to spontaneous intracranial hypotension. CT-guided fibrin occlusion has been described as a minimally invasive treatment strategy; however, its reproducibility across different institutions remains unclear. This multi-institution study evaluated the clinical and radiologic outcomes of CT-guided fibrin occlusion, hypothesizing a correlation among cure rates, fibrin injectate spread, and drainage patterns.
MATERIALS AND METHODS: A retrospective evaluation was conducted on CT-guided fibrin glue treatment in patients with CSF-to-venous fistulas from 6 US and UK institutions from 2020 to 2023. Patient information, procedural characteristics, and injectate spread and drainage patterns were examined. Clinical improvement assessed through medical records served as the primary outcome.
RESULTS: Of 119 patients at a mean follow-up of 5.0 months, fibrin occlusion resulted in complete clinical improvement in 59.7%, partial improvement in 34.5%, and no improvement in 5.9% of patients. Complications were reported in 4% of cases. Significant associations were observed between clinical improvement and concordant injectate spread with the fistula drainage pattern (P = .0089) and pretreatment symptom duration (P < .001). No associations were found between clinical improvement and cyst puncture, intravascular extension, rebound headache, body mass index, age, or number of treatment attempts.
CONCLUSIONS: Fibrin occlusion performed across various institutions shows cure when associated with injectate spread matching the CVF drainage pattern and shorter pretreatment symptom duration, emphasizing the importance of accurate injectate placement and early intervention.
ABBREVIATIONS:
- BMI
- body mass index
- CTM
- CT myelography
- CVF
- CSF-to-venous fistula
- SIH
- spontaneous intracranial hypotension
CSF-to-venous fistulas (CVFs) have been increasingly recognized as a cause of spontaneous intracranial hypotension (SIH) since their first description in 2014.1 Initially, surgical ligation of the associated nerve root or adjacent draining veins was the primary treatment strategy for CVF.2 More recently, less invasive treatment strategies have been described with high degrees of efficacy, including fibrin occlusion and transvenous embolization.3,4 Fibrin occlusion is performed percutaneously using either fluoroscopic or CT guidance, whereas transvenous embolization is performed via an endovascular approach using a liquid embolic agent under live fluoroscopy. Both procedures have been described by a few quaternary SIH referral centers as safe, having low adverse effect profiles and relatively high rates of radiologic and clinical improvement.5,6 However, the replicability of these techniques and outcomes across other institutions and patient populations is unknown.
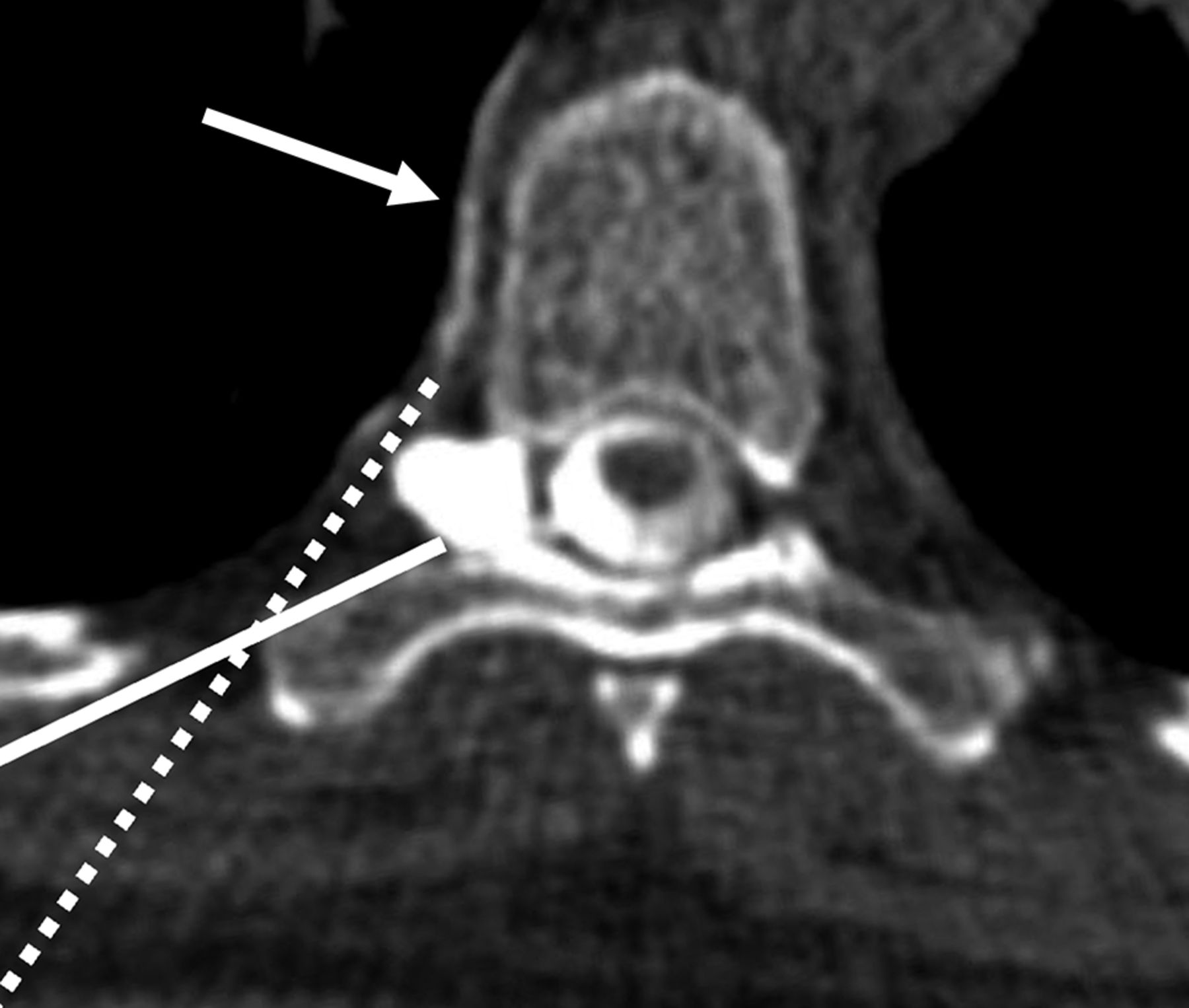
The use of fibrin sealant as a neurosurgical adjunct for postoperative CSF leaks is well-known, and its use under image guidance for treatment of SIH has been documented since at least 2004.7 The relatively high cure rates described in the 2021 reports of CVF fibrin occlusion were somewhat surprising, given that prior reports stated minimal response to epidural patching.3,8 However, unlike traditional epidural patching, the fibrin occlusion technique described needle positioning at the junction of the meningeal diverticulum and/or downstream draining vein, sometimes with >1 needle (Fig 1). The resultant spread of fibrin injectate was often predominantly foraminal, paraspinal, and sometimes even within a meningeal diverticulum and/or intravascular, rather than within the dorsal or ventral spinal epidural space as would be achieved in a traditional dorsal interlaminar or transforaminal epidural injection (Fig 2).

Expected needle trajectories for a typical transforaminal epidural steroid injection (solid line) compared with that for a fibrin CVF occlusion (dotted line), targeting a CVF with paraspinal drainage (arrow).

Direct cyst puncture of a CVF in a 64-year-old woman. A, Axial left decubitus CTM shows an intraosseous left T12 CVF embedded within the pedicle (arrow) with intraosseous and segmental venous drainage (arrowheads). B, Axial prone CT shows a needle intentionally directly puncturing the intraosseous meningeal diverticulum (arrow). C, Axial image slightly cranial to B shows contrast-enhanced glue within the osseous and paraspinal veins (arrows). D, Posttreatment left decubitus CTM 1 month later shows resolution of the CVF.
The aim of this study was to characterize clinical and radiologic treatment outcomes of CT-guided fibrin occlusion across multiple institutions, hypothesizing that fibrin injectate spread patterns that more closely approximated the drainage pattern of the targeted CVF would be associated with a relatively higher cure rate and that injectate spread patterns that did not match the CVF drainage pattern would be associated with treatment failure. A secondary aim of this study was to characterize the safety profile and success rate of fibrin occlusion when performed by various proceduralists across multiple institutions.
MATERIALS AND METHODS
Patients
This was a retrospective cross-sectional cohort study involving 6 institutions across the United States and the United Kingdom from March 1, 2020, through March 31, 2023. Approval from each respective institution's ethics board was obtained or considered exempt as appropriate, and written informed consent was waived. Inclusion criteria included the following: 1) SIH diagnosis according to the “International Classification of Headache Disorders, 3rd ed”; 2) a CVF diagnosed by decubitus CT myelography (CTM); 3) CT-guided fibrin occlusion as a first-line therapy; and 4) a documented clinical response in the patient's electronic medical record.9 Patient information including age, sex, body mass index (BMI), CVF level and side, pretreatment brain MR imaging, Bern score, and duration of symptoms was recorded.10
CT-Guided Fibrin Glue Technique
The fibrin glue technique for CVF has been described previously, but briefly, the patient is positioned prone on the CT table and scanning is performed at the CVF level.3,6 Spinal needles are placed along the CVF course using anatomic landmarks. A test dose of 0.2–0.5 mL of air and/or iodinated contrast is injected, depending on the preference of the proceduralist to outline the eventual glue location, and the needle position is modified if needed. Occasionally, if 2 needles were not placed initially, an additional needle may be placed after a test injection to optimize injectate spread. After adding 0.2 mL of preservative-free contrast into both hubs of the fibrin glue syringe (Tisseel or Artiss fibrin sealant, 4 mL; Baxter), the contrast-enhanced fibrin glue is injected into the spinal needle along the CVF course.
CVF Characteristics
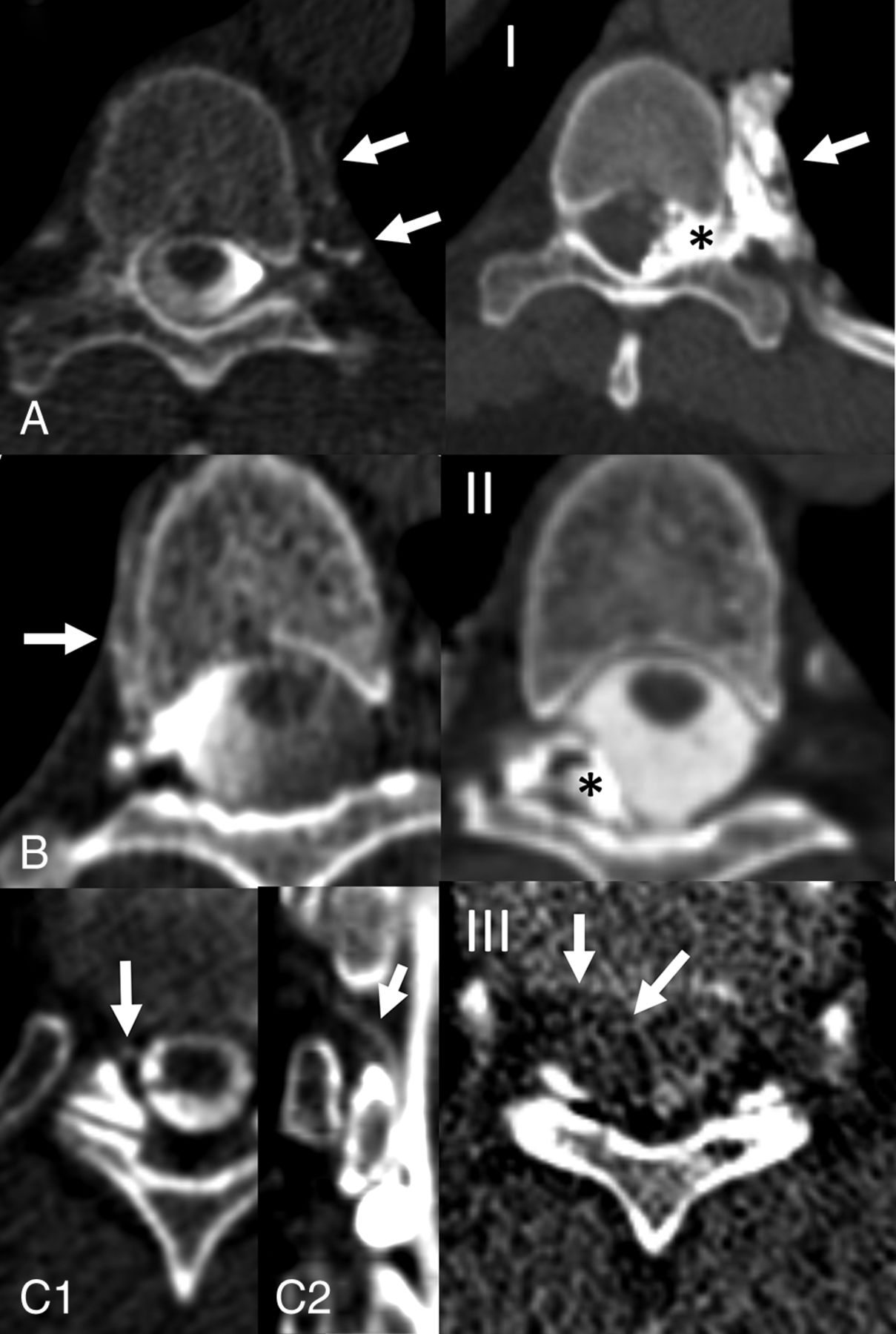
Each initial dynamic myelogram of a CVF was assessed for the primary venous drainage pattern and classified by the proceduralist as either paraspinal, internal epidural, or both. Postpatch images were then assessed, and the distribution of fibrin injectate was classified as either paraspinal, epidural, or both. Fibrin glue injection spread patterns were then compared with CVF drainage patterns and assessed for concordance of the injectate spread and CVF drainage. For example, a CVF that had paraspinal drainage but epidural injectate spread would be considered discordant, whereas a CVF that had paraspinal drainage and paraspinal injectate spread would be considered concordant (Fig 3).

Examples of fibrin spread in 3 patients with a CVF. A, Left decubitus dynamic CTM demonstrates a CVF with paraspinal drainage (A, arrows), which was adequately covered by fibrin injectate in the paraspinal space (I, arrow), with additional extension into the lateral epidural space (I, asterisk). This injectate coverage was considered concordant with the CVF drainage. B, Right decubitus dynamic CTM demonstrating a CVF with paraspinal drainage (B, arrow), with fibrin injectate confined only to the dorsolateral epidural space (II, asterisk). This injectate coverage was considered discordant from the CVF drainage. C, Axial (C1) and coronal (C2) images from a right decubitus dynamic CTM demonstrating a CVF draining into the right epidural venous plexus (arrows), and axial (III) post injection image demonstrating fibrin injectate spreading along the right epidural space (arrows). This injectate coverage was considered concordant with the CVF drainage.
Procedural Characteristics
Additional treatment characteristics were recorded, including needle gauge and number of needles within a single procedure, as well as the type and volume of fibrin sealant used. The total number of fibrin occlusion attempts was also recorded, and if >1 procedure was performed, variables from the final procedure were used. Whether any postprocedural adverse event occurred was recorded.
Clinical and Radiologic Evaluation
The primary outcome was the patient's clinical response, which was assessed by retrospective review of the patient's medical record by the proceduralist team for written documentation of either complete, partial, or no clinical improvement, along with the clinical follow-up time. This documentation consisted of either clinic or telephone encounter notes written by either the patient's primary care physician, referring neurologist, a radiology nurse/nurse practitioner, or the proceduralist. Whether there was a documented clinical record, either in the immediate postprocedural period or in the days to weeks following the procedure, of a patient developing symptoms suspicious for rebound intracranial hypertension was recorded. If the patient underwent postprocedural MR imaging of the brain, the posttreatment Bern score and brain MR imaging follow-up time were also recorded. Procedural covariates such as the number of total attempts, needles, needle gauge, and whether there was intravascular extension of fibrin or a direct cyst puncture were recorded.
Statistical Analysis
The primary outcome of the study was clinical improvement, which was treated as a 3-category variable (no improvement, partial improvement, complete improvement). All exposures were tested univariately for association with clinical improvement. Dichotomous exposures (concordant spread, cyst puncture, intravascular extension, rebound headache) were tested via logistic regression, with the exposure as the outcome and clinical improvement as a covariate. BMI, age, and the number of attempts were tested via linear regression with the exposure as the outcome. Symptom duration was tested via robust linear regression with Huber weights; robust regression was used to ensure valid inference in the presence of outliers. For logistic regression models, association of categoric clinical improvement with the exposure was tested via a likelihood ratio test. For linear regression models, an F-test was used, and for robust linear models, a robust F-test was used. In the case of a significant association for the 3-category outcome, pair-wise comparisons were tested using the Tukey post hoc correction. A 6-fold Bonferroni multiple testing correction was applied to secondary exposures. All data analyses were performed using R statistical and computing software, Version 4.1.2 (http://www.r-project.org/).
RESULTS
Patients
Patients' descriptive statistics are summarized in Tables 1 and 2. One hundred nineteen total patients with 120 total CVFs were included in the analysis. Three patients did not have documentation of their clinical response in the medical record and thus were not included in the analysis. One hundred eighteen patients had 1 CVF, and 1 patient had 2 CVFs. The 2 CVFs in the single patient were on opposite sides but at adjacent levels at T7 and T8. The mean patient age was 59.3 (SD, 11.7) years. The mean patient BMI was 27.1 (SD, 5.2). Sixty-three of 119 (52.9%) patients were women, and 56/119 (47.1%) patients were men. Mean patient symptom duration was 34.6 (SD, 73.4) months. One hundred eighteen of 119 (99.2%) patients had a pretreatment MR imaging, and the mean pretreatment Bern score was 6.4 (SD, 2.3).
Descriptive statistics of patients
Descriptive statistics of fistulas
CVF Characteristics
Seventy-six of 120 (63.3%) fistulas were on the right. One hundred fourteen of 120 (95.0%) originated in the thoracic spine, 3/120 (2.5%) originated in the lumbar spine, and 3/120 (2.5%) originated in the cervical spine. Eighty-seven of 120 (72.5%) CVFs had only paraspinal drainage, 11/120 (9.2%) CVFs had only epidural drainage, and 22/120 (18.3%) had paraspinal and epidural drainage.
Procedural Characteristics
Tables 3 and 4 summarize the procedural characteristics. Seventy-five of 120 (62.5%) CVFs were treated with 20-ga needles, 44/120 (36.7%) were treated with 22-ga needles, and 1/120 (0.8%) was treated with an 18-ga needle. One needle was used in 88/120 (73.3%) cases, 2 needles were used in 28/120 (23.3%) cases, and 3 needles were used in 4/120 (3.3%) cases. Tisseel fibrin sealant was used in all except 1 case, in which Artiss fibrin sealant was used. In 9 cases, 2–9 mL of autologous blood was injected with fibrin, and in the remaining cases, fibrin sealant was injected in isolation. The mean and median (Q1, Q3) of fibrin sealant used were 4.15 (SD, 1.63) mL, and 4.00 (3.5–4.00) mL, respectively. Intravascular extension of fibrin was noted in 37/120 (30.8%) cases. A direct cyst puncture was performed in 20/120 (16.7%) cases. The mean number of procedural attempts per patient was 1.5 (SD, 0.9).
Descriptive statistics of procedures (subject level)
Descriptive statistics of procedures (fistula level)
Clinical Outcome
One hundred nineteen patients all had documentation of the degree of clinical improvement or lack thereof following the procedure in their electronic medical record. The mean clinical follow-up time was 5.0 (SD, 5.8) months (range, 0.25–20 months). Complete clinical improvement was documented in 71/119 (59.7%) patients, partial clinical improvement was documented in 41/119 (34.5%) patients, and no clinical improvement was documented in 7/119 (5.9%) patients. Mean injectate volume stratified by clinical improvement was 4.0 (SD, 1.5) mL in complete, 4.4 (SD, 2.0) mL in partial, and 3.7 (SD, 0.5) mL in no improvement. More than 1 needle was used in 18/71 (25.3%) patients with complete improvement, 12/41 (29.2%) patients with partial improvement, and 2/7 (28.6%) patients with no improvement. Postprocedural complications occurred in 5/119 (4%) cases. These included asymptomatic pulmonary embolism in 2 patients (noted on routine postprocedural imaging performed to assess injectate spread, not prompted by any change in clinical status) and self-limiting radicular pain in 3 patients. Thirty-three of 119 (27.7%) patients experienced a new nonorthostatic headache postprocedure, which was clinically suspected to reflect rebound intracranial hypertension.
Within the complete response group, injectate spread was concordant with the fistula drainage pattern in 60/72 (83.3%) fistulas, compared with 30/41 (73.1%) in the partial response group and 2/7 (28.6%) in the no response group. There was a statistically significant association between concordant spread and clinical improvement (P = .0089). Pair-wise group tests further revealed that subjects with complete clinical improvement had significantly higher odds of concordant spread compared with those with no clinical improvement (OR = 12.5; 95% CI, 1.53–101.7; P = .013).
The mean pretreatment symptom duration was 1.3 years in the complete response group, 4.7 years in the partial response group, and 8.2 years in the no response group. There was a highly significant association between pretreatment symptom duration and clinical improvement (P < .001). Pair-wise group tests indicated that subjects with no clinical improvement had significantly longer symptom duration compared with those with complete clinical improvement (estimate = 3.0; 95% CI, 1.5–4.4; P < .001). Likewise, subjects with partial clinical improvement had significantly longer symptom duration compared with those with complete improvement (estimate = 1.1; 95% CI, 0.4–1.9; P <.001), whereas subjects with partial improvement had significantly shorter symptom duration than those with no improvement (estimate = 1.8; 95% CI, 0.3–3.3; P = .01).
After Bonferonni correction for multiple comparisons, no statistically significant associations were found between clinical improvement and cyst puncture (P = .22), intravascular extension (P = .85), rebound headache (P = .42), BMI (P = .95), age (P = .06), or the number of attempts (P = .31).
Radiologic Outcome
Of the 119 subjects, 92 underwent follow-up MR imaging, while 27 had not at the time of data analysis. Postprocedural MR imaging was performed at a mean duration of 3.5 months. Logistic regression analysis indicated no significant association between missing follow-up MR imaging and clinical improvement. The mean change in the Bern score (calculated as posttreatment Bern score minus pretreatment Bern score) in those with a complete response was −5.4, compared with −2.9 in the partial response group and 0.6 in the no response group. Figure 3 shows pre- and posttreatment Bern scores stratified by clinical improvement. No inferential analysis was performed due to the incomplete data.
DISCUSSION
This study aimed to assess the clinical and radiologic treatment outcomes achieved through CT-guided fibrin occlusion of CVFs across multiple institutions. Our results suggest that treatment success may be in part driven by whether the spread of fibrin injectate matches the target drainage pathway of the CVF and thus provides a potential explanation to account for the failure of a fibrin patch to treat a CVF. Specifically, when a technique mirroring a traditional transforaminal epidural steroid injection is used, achieving a robust epidural spread of injectate is often desirable. However, these data suggest that such a spread pattern is only desirable if there is concurrent drainage of the CVF into the internal epidural venous plexus; otherwise, the needle tip should be positioned more laterally, anterior or posterior to the foramen to target the CVF anatomy (Fig 1). Therefore, rather than using a standard transforaminal technique for all CVFs, we suggest mapping each CVF drainage pattern preprocedurally to plan needle positions accordingly. Before the termination of a procedure, postinjection imaging should be performed and studied for such adequate coverage, and if it is not achieved, additional injections should be considered. Historically, reports of patching for CVF described minimal treatment success; however, exact details such as the image-guidance technique and injectate location and amount were not reported.8,11 Our experience suggests that CT-guided fibrin glue injections that cover the CVF drainage are one of the main keys to successful treatment.
We found that this procedure demonstrates a favorable safety profile while achieving a relatively high clinical and radiologic cure rate. At a mean follow-up of 5.0 months, 59.7% of patients reported complete symptom improvement. This rate is lower than that of the initial reports describing fibrin occlusion, which may more closely approximate the effectiveness of this procedure in the hands of multiple proceduralists across various institutions.3,6 As centers build continued experience with this procedure, particularly with the unique needle placement required for successful fibrin occlusion, we speculate that there will be a stepwise improvement in clinical outcomes. Further research should continue to evaluate the success rate of this procedure as techniques are refined and more experience is gained.
Secondary analysis did not suggest that direct cyst puncture, intravascular spread of injectate, or the development of rebound intracranial hypertension independently predicted treatment success. There were no cases of confirmed or suspected arachnoiditis in our cohort despite a direct cyst puncture performed in 20 cases, and despite 37 cases of intravascular fibrin extension, there were only 2 instances of an incidentally imaged pulmonary embolism, neither of which were symptomatic. Despite the lack of clinically meaningful thromboembolic complications related to the procedure in our cohort, fibrin sealant does carry a black box warning in the United States advising against intravascular injection.
In our cohort, most (63.3%) CVFs were found on the right side, which is in keeping with several prior reports of CVF stratified by laterality.12⇓-14 Given this repeat evidence suggesting a right-sided predilection for CVF, we suggest starting digital subtraction myelography or decubitus CT myelography with the patient in the right decubitus position in the absence of other guiding factors. Also, in keeping with prior literature, most patients in our cohort were overweight, with a mean BMI of 27.1.12,15 Others have postulated that CSF hypertension secondary to obesity could lead to damage to spinal arachnoid granulations in the de novo or postsurgical setting.8,16 Further research should continue to investigate the associations between these factors and CVF pathophysiology.
Longer clinical duration of symptoms preceding treatment was inversely related to treatment success. This finding is in keeping with a recent report by Häni et al,17 which concluded that a shorter duration of preoperative symptoms was the strongest predictor of favorable response to the surgical treatment of type 1 and 2 CSF leaks. The enduring significance of this discovery in an alternative type of leak and treatment approach reinforces the understanding that SIH is intricately influenced by symptom duration in not only its clinical and imaging manifestations but also its susceptibility to treatment.18⇓⇓-21 While we believe that there is likely some pathophysiologic underpinning to this phenomenon, this relationship may also in part reflect regression to the mean independent of treatment as a result of selection bias in patients with longer symptoms. Nonetheless, we believe that prompt and decisive treatment strategies should be used for patients with spinal CSF leaks or CVF, without any unnecessary delays.
This study has important limitations, including its modest sample size (particularly in the no clinical response group) and retrospective nature. Specifically, due to the lack of universal prospective implementation of standardized or validated clinical response scoring criteria at the participating institutions, assessment of clinical response was obtained through a retrospective review and secondary classification of notes in each patient's medical record. This approach is potentially prone to interpretation bias, which may limit the generalizability of these findings. While the post hoc use of such measurement tools (such as the Headache Impact Test [HIT-6] headache questionnaire) could have been retrospectively administered to patients, this would have also introduced bias and therefore was not pursued. Institutions providing care for patients with SIH should consider routine, prospective, pre- and postprocedural use of such tools. Despite this potential limitation, we noted a concurrent stepwise improvement in the imaging response paralleling that in the patients with no, partial, or complete clinical improvement (Fig 4), which strengthens the overall validity of this classification schema and supports the potential reliability of the findings of this study. Additional limitations include the potential for missing cases of rebound intracranial hypertension because, in general, these symptoms are subjective and their documentation was subject to self-reporting by the patient.

Posttreatment Bern score (left) and change in Bern scores (right) stratified by clinical improvement.
CONCLUSIONS
CT-guided fibrin occlusion is a safe and effective treatment for CVF, achieving a relatively high clinical and radiologic cure rate with a small adverse effect profile across multiple institutions. The alignment between the spread pattern of fibrin injectate and the drainage pathway of CVFs appears to play a significant role in treatment success, emphasizing the importance of preprocedural mapping and tailored needle positions. Additionally, the shorter duration of symptoms preceding treatment was associated with a higher likelihood of treatment success, highlighting the significance of prompt intervention in patients with SIH.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received July 21, 2023.
- Accepted after revision August 27, 2023.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Advanced Imaging of Type 2 Spinal CSF Leaks with Ultra-High-Resolution Conebeam CT Myelography
- Additional Diagnostic Value of Conebeam CT Myelography Performed after Digital Subtraction Myelography for Detecting CSF-Venous Fistulas
- Assessing the Diagnostic Value of Brain White Matter Hyperintensities and Clinical Symptoms in Predicting the Detection of CSF-Venous Fistula in Patients with Suspected Spontaneous Intracranial Hypotension
- Hypersensitivity Reactions to Fibrin Glue during Epidural Blood Patching
- Technical Tips for CT-Guided Fibrin Glue Patching of CSF-Venous Fistulas
- CSF-Venous Fistulas Arising Intraosseously within Bone Remodeled by Meningeal Diverticula
- Spontaneous Intracranial Hypotension in Children: A Multi-Institutional Review of Spinal CSF Leaks Localized on Advanced Myelography
- Spinal CSF Leaks: The Neuroradiologist Transforming Care
- Myelographic Techniques for the Localization of CSF-Venous Fistulas: Updates in 2024
- The Spatial Relationship between Spinal Osteoarthritis and CSF Venous Fistulas in Patients with Spontaneous Intracranial Hypotension
- Perspectives from the Inaugural "Spinal CSF Leak: Bridging the Gap" Conference: A Convergence of Clinical and Patient Expertise