
Abstract
BACKGROUND AND PURPOSE: Long-range connections are more severely damaged and relevant for cognition in long-standing MS. However, the evolution of such coordinated network damage in patients with MS is unclear. We investigated whether short- and long-range structural connections sustained equal damage in early-stage MS.
MATERIALS AND METHODS: Sixteen patients with early-stage MS and 17 healthy controls were scanned by high-resolution, multishell diffusion imaging on 7T MR imaging and assessed cognitively. We investigated macrostructural properties in short- and long-range fibers and of microstructural metrics derived from 2 quantitative diffusion MR imaging models: DTI and neurite orientation dispersion and density imaging.
RESULTS: Patients had significant WM integrity damage—that is, higher radial diffusivity and a lower intracellular volume fraction in the focal WM lesions. Compared with the healthy controls, the patients had noticeable microstructure changes in both short- and long-range fibers, including increased radial diffusivity, mean diffusivity, and axial diffusivity. Z scores further indicated greater damage in the short-range fibers than in the long-range fibers.
CONCLUSIONS: Our findings demonstrate that more severe demyelination preceding axonal degeneration occurs in short-range connections but not in long-range connections in early-stage MS, suggesting the possibility that there are cortical lesions that are undetectable by current MR imaging.
ABBREVIATIONS:
- AD
- axial diffusivity
- EDSS
- Expanded Disability Status Scale
- FA
- fractional anisotropy
- ficvf
- intracellular volume fraction
- HC
- healthy control
- MD
- mean diffusivity
- NODDI
- neurite orientation dispersion and density imaging
- ODI
- Orientation Dispersion Index
- RD
- radial diffusivity
MS has been histologically characterized by the aggregation of inflammation, demyelination, gliosis, and axonal transection that ultimately leads to neurologic disability in young adults. MS can present with highly variable symptoms such as loss of vision, limb weakness, sensory loss, ataxia, and cognitive impairment.1,2 Neuroimaging studies have helped to define the pathologic substrates and microstructure (eg, demyelination) alternations of this disorder in focal lesions and diffusely abnormal tissue.3,4 While the specific WM fiber changes remain elusive, these local abnormalities in tissue microstructure are not enough to explain the clinically observed functional impairment.5,6 Nevertheless, there is growing evidence that neurologic impairment in MS is determined more by specific large-scale functional network alterations than by local tissue microstructural alterations.7,8
The subtle balance between short- and long-range connections contributes to the integration and segregation of the brain connectome. Connections of different lengths are found in different locations across the brain; short-range fibers are more abundant than their long-range counterparts, and the short-range fibers connect adjacent anatomic gyri that integrate multimodal information. Concurrently, long-range connections allow rapid and efficient interareal communication (eg, among cortical regions where tracts may cross the centrum semiovale) or diversification of information.9⇓⇓-12 Cognitive impairment is one of the primary symptoms of MS, occurring in up to 70% of patients.2 The specific damage to long-range connections in patients with long-standing MS would affect cognition by reducing the global efficiency of brain networks.13 However, it is still unclear when such distinct connectivity adjustments happen and whether this is a unique feature of patients with long-standing MS. In-depth knowledge of the evolution of the balance between short- and long-range connections during disease progression would significantly increase the understanding of the clinical symptoms of MS.
Previous studies have found that cortical demyelination occurs early, is common in patients with MS, and would affect the U-fibers more.4,14 Thus, we propose the following hypothesis: Short-range connections might be more severely damaged than long-range connections in early-stage MS, which is different from long-lasting MS. To make a definite determination, we explored the potential damage of long- and short-range structural connections in patients with early-stage MS who exhibited significant cognitive decline in this study. High-resolution DWI with multishell acquisition and structural MR imaging was performed on 16 patients with early-stage MS and 17 healthy controls (HCs), to quantify the damage to short- and long-range connections.
MATERIALS AND METHODS
Participants
For this prospective study, we recruited 16 patients with early-stage relapsing-remitting MS with a disease duration of <10 years.15,16 Patients had been diagnosed with MS according to the 2017 revisions of the McDonald criteria,17 had been free of clinical relapse, and had not required steroid treatment for at least 1 month before participation. Exclusion criteria were evidence of other structural brain diseases; a history of neuropsychiatric disorders, cognitive impairment, or other significant medical conditions; or contraindications to MR imaging. In addition, 17 age- and education level–matched HCs were recruited. Informed consent was obtained from each participant in this study, and the protocol was approved by the First Affiliated Hospital, School of Medicine, Zhejiang University. The cohorts have not been described in any previous publication.
Clinical Assessment
Neuropsychological tests were used to assess the most frequently impaired cognitive domains in MS. The tests included the Symbol Digit Modalities Test18 for information-processing speed, the Verbal Fluency Test19 for executive function, the Digit Span Test8 for attention, and the Auditory Verbal Learning Test20 for episodic memory. Also, the Mini-Mental State Examination and the Montreal Cognitive Assessment21 were performed to assess global cognitive function, and the Expanded Disability Status Score (EDSS)22 was performed for overall disability. The mean of the neuropsychological assessment of the patients was further analyzed by evaluating the deviation from the mean values based on the HC group. The results of each patient’s neuropsychological tests were regarded as normal if they declined <1.5 SDs from the mean values of the HC group;23 patients were diagnosed as cognitively impaired when the results of at least 2 tests had declined.24
Image Acquisition
All MR imaging data were acquired using a 7T MR imaging scanner (Magnetom; Siemens) with a 32-channel Nova Medical Head Coil (Siemens). For the structural MR imaging scans, T1-weighted images were acquired using a 3D MP2RAGE sequence with 0.8-mm isotropic resolution. The 3D sampling perfection with application-optimized contrasts by using different flip angle evolution (SPACE sequence; Siemens) T2 sequence was performed with a voxel size of 0.8 × 0.8 × 0.8 mm3. A multiband 2D EPI sequence was used for the multishell DWI protocol: 1.5-mm isotropic resolution, 3 shells (1000/2000/3000 s/mm2, 40 directions for each shell, single repetitions), and 8 repetitions without diffusion weighting; b=0 s/mm2. The gradient directions were optimized to maximize the minimal angle between directions and cross shells using the DMRITool25 (https://diffusionmritool.github.io).
DWI Data Preprocessing and Modeling
The image-processing pipeline is detailed below and summarized in Fig 1. All the preprocessing steps for raw DWIs, including eddy currents, motion, and EPI geometric distortion correction, were processed in the TORTOISE (Version 3.2; https://tortoise.nibib.nih.gov/) software package,26 and a T2-weighted image was used as the reference image. The output images with opposite phase-encoding were then used for EPI geometric distortion correction using the DR-BUDDI toolbox.27 The preprocessed diffusion data sets were then used for further diffusion metrics calculations.

Overview of the image acquisition and processing pipeline.
The DTI reconstruction was performed in TORTOISE using b = 0 and 1000 s/mm2, along with the calculation of fractional anisotropy (FA), axial diffusivity (AD), radial diffusivity (RD), and mean diffusivity (MD). The neurite orientation dispersion and density imaging (NODDI) reconstruction using the 3-shell data was performed in the NODDI toolbox in Matlab (Version 1.01; University College London, London, United Kingdom, http://mig.cs.ucl.ac.uk/index.php?n=Tutorial.NODDImatlab).28 Maps of NODDI metrics, including intracellular volume fraction (ficvf) and the Orientation Dispersion Index (ODI) were then generated.
WM Lesion ROI Identification and Analysis
The individual T1-weighted image was linearly registered to each patient’s B0 image. A whole-brain WM mask was segmented with coregistered T1-weighted images. The ROIs of patients with WM lesions were manually drawn on T1-weighted images with the complementing guidance of the T2-weighted images. The lesion load of each type of fiber was further defined as the fraction of fiber volume overlapped with the WM lesions (ie, volume of the fiber overlapped with WM lesions divided by the whole volume of this type of fiber).
B0 images of each HC were first linearly (FMRIB Linear Image Registration Tool [FLIRT]; http://www.fmrib.ox.ac.uk//fsl/fslwiki/FLIRT) and then nonlinearly registered to the same diffusion-weighted images in each patient with MS to obtain the location-matched ROIs in the HC group. Finally, the mean value of the diffusion MR imaging metrics for each ROI or whole WM was calculated.
Tractography
The probabilistic tractography procedure was performed on the MRtrix3 software package (http://www.mrtrix.org).29 Five tissue-type segmented images obtained from the T1-weighted images were used for the Anatomically-Constrained Tractography framework.30 We estimated the response functions and computed the fiber orientation distributions from the preprocessed DWI. Next, streamline tractography was performed by randomly seeding 20 million streamlines with default settings filtered to 2 million streamlines using spherical-deconvolution informed filtering of tractograms.31
We segmented structural fiber tracts into short- and long-range fibers as previously described.13 Then, we calculated the number and average length of the fibers in the whole WM. In addition, the mean of the microstructure metrics (eg, FA, ficvf) along the selected fiber tracts was calculated. We used the z score to compare the MR imaging metrics between short- and long-range fibers on a common scale. The formula for calculating the z score is z = (x − μ)/σ, where x is the mean value of the MR imaging metrics of short or long fibers in the MS group, μ is the mean value of corresponding MR imaging metrics in the MS group, and σ is the SD of the corresponding MR imaging metrics in the HC group.13
Statistical Analysis
Statistical analysis was performed using SPSS software (Version 24; IBM). Group differences in unpaired parametric data were assessed using the independent-samples t test for continuous variables and the χ2 test for categoric variables. The results of the z scores of short- and long-range fibers were analyzed using the 1-sample t test on a convergence of the average value to zero to compare with the HCs. The paired analysis of short- and long-range homologous fibers for each patient with MS was compared with the paired t tests. For patients with MS, intersubject bivariate correlation was performed between the MR imaging metrics and the clinical characteristics, while age and education level were treated as covariates of no interest. The level of statistical significance after false discovery rate correction was set at P < .05 for all statistical analyses.
RESULTS
Disability, Cognition, and Brain Volume
Demographic, clinical, and MR imaging characteristics for the patients with MS and the HCs are presented in Tables 1 and 2. In the MS cohort, patients had severe damage in several cognitive domains (Table 2). A total of 10 of 16 patients (62.5%) were classified as cognitively impaired. Among the remaining 6 patients, 3 (18.8%) showed isolated cognitive impairment in the form of reduced information-processing speed. Further brain volume comparison did not detect a significant difference in WM volume.
Demographic, clinical, and MR imaging volumetric characteristics of all participantsa
Summary of cognitive measuresa
Microstructure Metrics in Focal and Diffuse Lesions
The statistical analysis of the microstructure metrics assessed with the DWI of the WM lesion ROIs and whole WM is shown in Table 3. All quantitative metrics, except for ODI, of the focal lesion ROIs had a significant difference between the MS and HC groups. As for the whole WM, no significant differences were found between these 2 groups.
Microstructure metrics and fiber statistics of focal WM lesions and whole-brain WMa
Difference of the Whole-Brain Fibers between MS and HC Cohorts
There were no significant differences between the MS and HC cohorts in the overall number or average length of whole-brain fibers (Table 3). However, when short- and long-range fibers were observed independently, further analysis of the microstructure metrics of the short- and long-range fibers between the HC and MS cohorts revealed that the short-range fibers in patients with MS had a significant change in FA (P < .05), MD, AD, and RD (Fig 2). Long-range fibers in patients with MS showed a significant increase in MD, AD, and RD.

The fiber microstructure metrics of whole-brain short- (black) and long-range (gray) connections in patients with MS and HCs. log2 indicates the length of fibers was denoted in a logarithmic manner with base 2.
Direct Comparison of Damage (Z Scores) to Short- and Long-Range Connections
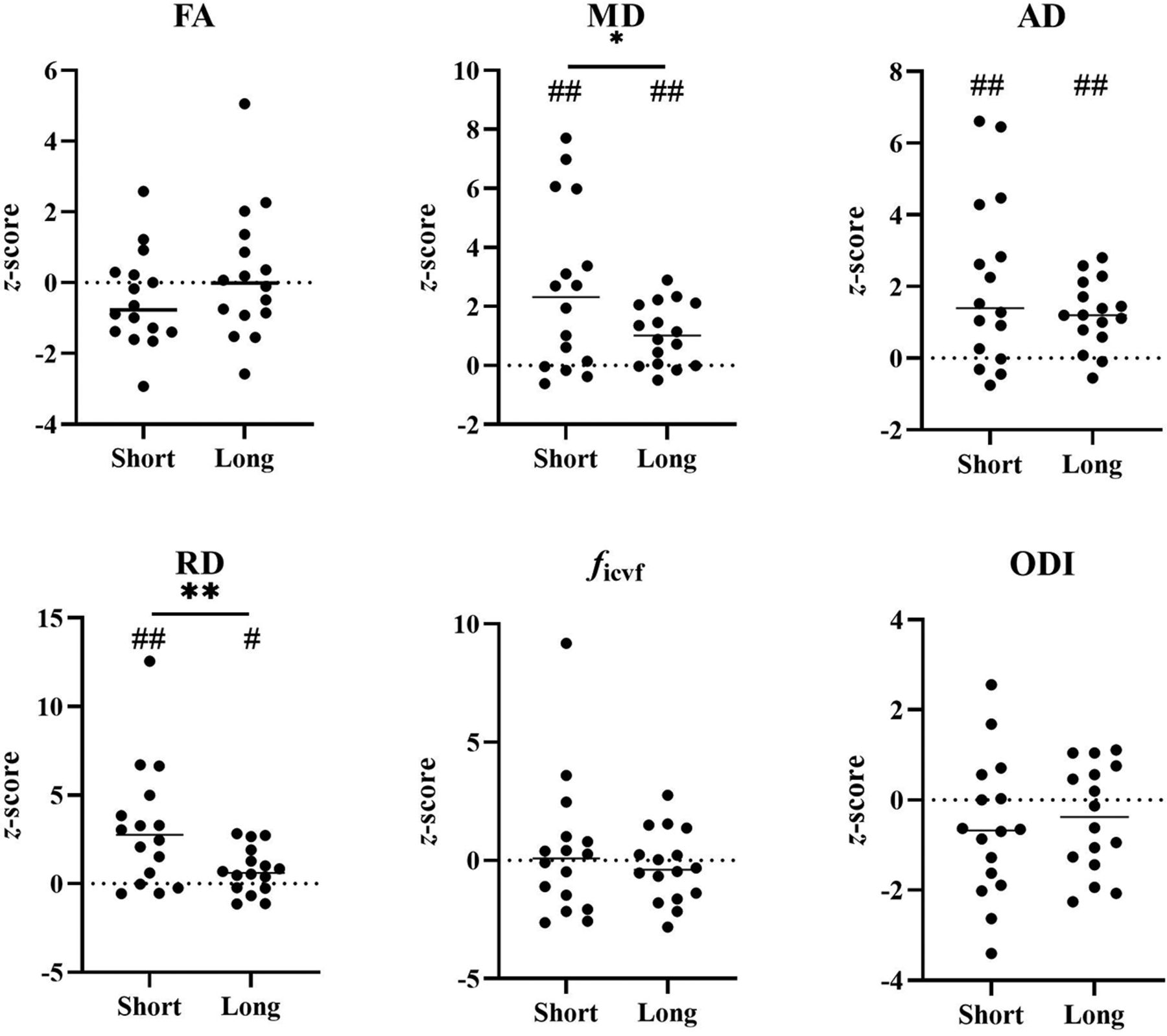
The WM lesion ROIs overlapped with 6.66% (range, 1.87%–9.55%) of the whole-brain fibers in patients with MS. The z score analysis of fiber properties is presented in Fig 3, in which both short- and long-range fibers show a significant increase in MD, AD, and RD in patients with MS compared with HCs. The increased MD, AD, and RD indicate the potential damage of WM integrity along short- and long-range fibers (Fig 3).

Severity of lesion damage (z score) compared between short- and long-range connections. The * represents a significant difference between short-and long-range fibers (P < 0.05); ** represents P < 0.01. # represents P < 0.05 using the one sample t test on a convergence of the average value to zero to compare with HCs. ## represents P < 0.01, FDR-corrected.
Further comparisons between the z scores of short- and long-range fibers show that the short-range connections have a larger increase than the long-range connections in both MD and RD. The MD z score was 2.57 (SD, 2.78) (short) versus 1.06 (SD, 1.05) (long), P < .05; and the RD z score was 3.10 (SD, 3.44) (short) versus 0.75 (SD, 1.29) (long), P < .01. The other microstructure metrics also showed the same tendency: The short-range fibers were more severely damaged than the long-range fibers.
Associations with Clinical Variables
No significant associations were found between MR imaging metrics and clinical variables after adjustment was made for the effect of age and years of education.
DISCUSSION
Long-range structural connections are more severely damaged in patients with long-standing MS.13 We have observed that the short-range connections are more severely damaged in early-stage MS, suggesting that the structural connections are altered differently during the progress of MS. In this study, the members of the MS cohort were in the early stages of disability, with a median EDSS score of 1.0, and had distinct cognitive impairment without obvious brain atrophy.
Microstructure Properties in MS WM Lesions and Whole WM
Our results show that in subjects with MS, WM lesion ROIs have higher MD, AD, and RD and lower FA and ficvf values compared with HCs. These results suggest there is damage to the WM integrity in these focal lesion areas, which is consistent with previous findings.32,33 However, there were no significant differences in the microstructure metrics of whole WM as found in previous studies,32,34 even though these changes have been observed in patients who have had MS for a longer time (>10 years).13,33 This finding is not surprising because the volume of the detectable WM lesions is relatively small (∼4 mL on average) and takes only a small portion of the whole WM in early-stage MS, while the WM lesions are much larger in long-lasting MS (eg, ∼670 mL13). In addition, previous studies have found that there was no significant difference in diffusion metrics in the normal-appearing WM of subjects with early-stage MS compared with controls.32,34 These 2 factors could make the changes of the whole-WM averaged diffusion MR imaging metrics relatively small, which means a large sample size is needed to make such changes significant in statistics.
Short-Range Connections Are More Severely Damaged in Early-Stage MS
In this study, the short-range fibers showed a more severe increase in the mean RD and MD values than the long-range fibers, a finding different from the results in patients with long-standing MS.13 Previous studies have shown that notable changes in RD are considered as noninvasive surrogate markers for myelin integrity, and myelin integrity may influence the diffusivity along the perpendicular direction of fibers; AD and ficvf correspond more to axonal loss.28,35
These results agree with MS being primarily a demyelinating disease that ultimately results in axonal degeneration, and they are in line with reported pathologic findings and current dogma.36,37 The early damage to the short-range fibers reflects the possibility that cortical lesions precede the degeneration of long-range fibers, as discussed below. Previous studies have demonstrated that short-range fibers have more myelin than long-range fibers.9,38 Injury to long axons in MS, which eventually causes the fragmentation of fibers, is secondary to myelin loss and may be the consequence of trophic disturbances after mixed outcomes of cumulative interactions among oligodendrocytes, microglia, and neurons.36 Most interesting, the ODIs of short fibers showed no significant difference between 2 groups because ODI reflects only neurite orientation, which is not sensitive to demyelination.39
Potential Invisible Leukocortical Lesions
We found that the lesion load is higher for long-range connections, suggesting that WM lesions visible in T1-/T2-weighted MR imaging are located in the long-range fibers (Online Supplemental Data). This result seems to contradict the finding of more severe microstructural damage to the short-range connections compared with the long-range connections. However, it could also be that we have failed to identify some tissue injuries within the current T1-/T2-weighted MR imaging, especially those leukocortical lesions located in the connections between anatomic neighboring areas of the cerebral cortex (short-range fibers).11,38,40 These leukocortical lesions running through the U-fibers in patients have been defined as cortical type I lesions.41 Cortical demyelination occurs early and is common in patients with MS, and it develops independent from WM lesions.4,14 With the help of ultra-high-field MR imaging, some cortical pathology can be detected in patients with MS.42,43 Fortunately, we further confirmed by MP2RAGE that the U-fiber lesions appear in almost all patients with MS (12/16); this use of MP2RAGE provides a more precise anatomic delineation of white and gray matter pathology (Online Supplemental Data).43 However, it is still challenging to detect most cortical lesions due to their relatively small size, sparse inflammatory cell infiltration, and limited damage to the blood-brain barrier. All of these factors could result in invisible cortical lesions under current MR imaging methods.42 The more severe demyelination to the short-range connections found in this study suggests that fiber tract–based microstructure analysis might be another efficient way to see the invisible cortical lesions.
Limitations and Future Work
This study has some limitations. First, our sample of patients with early-stage MS was small and recruited cross-sectionally, but large and longitudinal studies are still needed to further validate the current study and monitor how the disease progresses. Second, our understanding of the relationship between short- and long-range connections is relatively immature, and future studies combining structural data with more functional data are needed to verify the intrinsic functional architecture of brain networks. Most important, although we have carefully compared our results with the available and published pathology and radiology results and NODDI is a well-validated method, a direct comparison between MR imaging findings and the pathology of the same subject should be conducted to further confirm our interpretation.
CONCLUSIONS
We evaluated the damage to structural connections in patients with early-stage MS with cognitive impairment and found that short-range fibers are more vulnerable to damage in early-stage MS, indicating that cortical demyelination might precede the axonal loss of long-range fibers in patients with MS.
Footnotes
This work was supported by the National Natural Science Foundation of China (NSFC) (Grant No. 81873894) and the Natural Science Foundation of Zhejiang Province, China (Grant No. LR20H180001), China middle-young VG Clinical Research Fund (2017-CCA-VG-047), National key research and development plan of China(2019YFC0118203, 2016YFC1306402), Zhejiang key research and development plan (2017C03011).
H. Liang is senior author. H. Liang and R. Bai contributed equally to this work.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received August 20, 2021.
- Accepted after revision December 11, 2021.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}