
Abstract
BACKGROUND AND PURPOSE: Ischemic stroke can be mimicked by nonischemic conditions. Due to emphasis on the rapid treatment of acute ischemic stroke, it is crucial to identify these conditions to avoid unnecessary therapies and potential complications. We investigated the performance of the multimodal CT protocol (unenhanced brain CT, CTA, and CTP) to discriminate stroke mimics from acute ischemic stroke.
MATERIALS AND METHODS: We retrospectively selected multimodal CT studies performed for clinical suspicion of acute ischemic stroke in our center in a 24-month period, including patients with at least 1 follow-up imaging study (brain CT or MR imaging). Hemorrhagic strokes were excluded. We measured the performance of multimodal CT, comparing the original diagnostic results with the final clinical diagnosis at discharge.
RESULTS: Among 401 patients, a stroke mimic condition was diagnosed in 89 (22%), including seizures (34.8%), migraine with aura attack (12.4%), conversion disorder (12.4%), infection (7.9%), brain tumor (7.9%), acute metabolic condition (6.7%), peripheral vertigo (5.6%), syncope (5.6%), transient global amnesia (3.4%), subdural hematoma (1.1%), cervical epidural hematoma (1.1%), and dural AVF (1.1%). Multimodal CT sensitivity, specificity, and accuracy were 24.7%, 99.7%, and 83%. Multimodal CT revealed peri-ictal changes in 13/31 seizures and diagnosed 7/7 brain tumors, 1/1 dural AVF, and 1/1 subdural hematoma. CT perfusion played a pivotal diagnostic role.
CONCLUSIONS: Multimodal CT demonstrated low sensitivity but high specificity in the diagnosis of stroke mimics in the acute setting. The high specificity of multimodal CT allows ruling out stroke and thereby avoiding unnecessary revascularization treatment in patients with diagnosis of a stroke mimic.
ABBREVIATIONS:
- CECT
- contrast-enhanced CT
- EEG
- electroencephalogram
- iCVE
- ischemic cerebrovascular event
- SM
- stroke mimics
- Tmax
- time-to-maximum
The clinical management of ischemic stroke requires a fast diagnostic workflow to refer patients to early revascularization.1 One of the challenges in the diagnosis of ischemic stroke is related to the presence of stroke mimic conditions, which are nonischemic disorders with clinical presentations similar to those of stroke. These disorders include seizures, systemic infections, brain tumors, toxic-metabolic conditions, positional vertigo, syncope, migraine, transient global amnesia, dementia, demyelinating disease, conversion disorder, and others.2,3 The prevalence of stroke mimics (SM) has been reported in up to 31% of patients with suspected acute stroke referred to the emergency department.4 Although complications of IV rtPA treatment in SM are rare,5,6 an accurate diagnosis is desirable to avoid unnecessary treatment and possible complications. Timely brain imaging is critical in the management of patients in this setting. MR imaging with diffusion-weighted imaging is the most sensitive technique to diagnose ischemic stroke. However, MR imaging is not routinely available in the emergency setting in many facilities; therefore, CT remains the first imaging method of choice in most centers. NCCT reliably rules out brain hemorrhage, but its sensitivity to identify early signs of brain ischemia is low in the first 6 hours from the onset of symptoms.7,8 Complementary CT techniques add further information on the presence, extent, and pathogenesis of ischemic stroke. CTA allows evaluating the status of neck and brain vessels and identifying a proximal arterial occlusion. CTP readily identifies areas of hypoperfused brain and allows estimating the presence of an ischemic core and an ischemic penumbra.9
A multimodal CT approach, including NCCT, CTA, and CTP, is used in many centers for the diagnosis of acute stroke,8 though the use of perfusion is not required by actual guidelines in the first 6 hours from stroke onset.1 Although multimodal CT has been reported to be able to distinguish some SM such as seizures, migraine, space-occupying lesions, infections, toxic-metabolic conditions, and others,10 there are scarce systematic studies on the diagnostic performance of multimodal CT in the diagnosis of SM, with most studies focusing on the diagnostic performance of CTP in seizures as a subgroup of SM.11⇓-13
In this study, we aimed to evaluate the overall diagnostic performance of multimodal CT for the diagnosis of SM not limited to seizures in the setting of acute stroke care.
MATERIALS AND METHODS
This is a retrospective study based on a single medical center with a comprehensive stroke unit that offers 24/7 admission of patients with acute stroke, clinical and imaging diagnoses, and systemic and endovascular treatment.
The study was approved by the local institutional Ethics Committee, Comitato Etico Cantonale. The study cohort included all consecutive patients who underwent a multimodal CT examination in the acute setting for suspected acute stroke in a 24-month period. Exclusion criteria were as follows: hemorrhagic stroke; incomplete multimodal CT (ie, lack of ≥1 imaging protocol component); examinations judged to be of nondiagnostic quality by the original interpreting neuroradiologist due to artifacts, poor patient cooperation, or other technical issues; and lack of at least 1 imaging follow-up (CT or MR imaging) necessary to confirm or rule out an acute brain ischemic lesion.
Triage of Clinical Patients
At our center, patients with clinical suspicion of acute ischemic stroke are promptly referred to a multimodal CT stroke imaging protocol after clinical evaluation by a neurologist, including an NIHSS evaluation.
Multimodal CT at Admission
Multimodal CT stroke imaging was performed using a dual-source 128-section CT scanner (Somatom Definition Flash; Siemens) as follows: NCCT of the head was followed by CTP acquired with a toggling-table technique, encompassing a brain coverage of 100 mm along the z-axis for 45 seconds with a temporal resolution of 1.5 seconds. We then performed CTA in a dual-energy mode from the aortic arch to the vertex with a bolus-tracking technique, placing the density-monitoring ROI in the ascending aorta with a trigger threshold of 100 HU. Contrast-enhanced CT (CECT) was acquired 4 minutes after the first injection of contrast medium when required. The details of CT technical parameters are reported in the Online Supplemental Data.
Postprocessing was performed by a CT technologist. Parametric qualitative maps of CBF, CBV, MTT, time-to-drain, and time-to-maximum (Tmax) were obtained from CTP data using a commercial perfusion package (VPCT-Neuro; Siemens). Arterial input and venous output time-attenuation curves were generated with ROIs automatically drawn on the anterior cerebral artery and the superior sagittal sinus, respectively. The CT technologist checked the correct positioning of the ROIs, the quality of the curves, and the presence of movement artifacts. Postprocessing of CTA source images was performed with multiplanar overlapping MIP reformatting. Images were sent, saved, and visualized in the PACS.
Follow-up CT and MR Imaging Examinations
Follow-up CT and MR imaging examinations were performed at a mean of 1.7 (SD, 2.6) days from admission before patient discharge, with MR imaging in 64% and CT in 36% of cases. NCCT was performed as described above. MR imaging was performed on a 3T scanner (Magnetom Skyra; Siemens) with a protocol consisting of at least the following sequences: axial DWI, axial FSE T2WI, axial FLAIR T2WI, and axial gradient recalled-echo T2*WI. The details of technical MR imaging parameters are shown in the Online Supplementary Data. Additional sequences, MRA, or postcontrast administration imaging were performed in selected cases as necessary.
Imaging Diagnosis at Admission and Retrospective Imaging Diagnosis
Images were rapidly interpreted and reported by a staff neuroradiologist who had access to the patient’s clinical information. The group of 7 reporting neuroradiologists included physicians with a subspecialty in neuroradiology and experience ranging from 1 to 15 years. Radiology reports were archived in the radiology information system, integrated into the hospital informatics system.
For this study, 2 neuroradiologists (E.P. and L.D.) retrospectively reviewed, in consensus, the original reports of the multimodal CT study performed at admission and assigned the imaging diagnosis to 1 of 3 different categories: 1) evidence of acute ischemic vascular event (iCVE) on imaging; 2) evidence of an acute condition other that iCVE on imaging, likely the cause of the clinical presentation (SM); and 3) no evidence of acute iCVE or SM on imaging. The imaging diagnosis based on the report of the multimodal CT at admission was considered the index text to be evaluated for performance.
Discharge Diagnosis and Retrospective Discharge Diagnosis
The discharge diagnosis documented and archived in the hospital informatics system was considered the final diagnosis. The discharge report with the final diagnosis was signed in consensus by 2 staff stroke neurologists and 1 neurology fellow on the basis of relevant clinical, imaging, electroencephalogram (EEG), and laboratory data. For this study, the diagnosis at discharge was retrospectively reviewed in consensus by 1 neurology fellow (C.M.) and 1 neuroradiologist (E.P.) and dichotomized into 2 final diagnoses: iCVE and SM. iCVE included stroke and TIA.14,15 For TIA, the likelihood of an ischemic event was rated with a version of the Precise Diagnostic Score scale.16 SM were cases in which the clinical details did not suggest an ischemic vascular etiology and another convincing explanation for the symptoms was found throughout supportive investigations. A few cases remained without a conclusive final diagnosis, even after evaluation of all available follow-up data. These included cases with less convincing clinical features, in which an alternative explanation for the clinical syndrome may have been present, but there was no definite proof of a nonstroke. These cases were excluded from the analysis. The final diagnosis at discharge for each patient was considered the reference diagnostic standard to establish true-positive, true-negative, false-positive, and false-negative and, therefore, to determine the accuracy of multimodal CT at admission.
Data Analysis
Descriptive statistics were presented as arithmetic mean with an SD or as median with interquartile range for quantitative data. Qualitative data were presented as absolute numbers with percentages. Comparisons of quantitative data among the 3 multimodal CT groups were performed with the Kruskal-Wallis test. With a statistically significant P value, we performed post hoc tests (Mann-Whitney), taking into account the multiple comparisons. Qualitative data among groups of patients were compared using the χ2 test. With statistically significant results, we made post hoc comparisons with the appropriate critical level adjustment.
Comparisons between the diagnostic test and the reference standard permitted calculating sensitivity, specificity, positive and negative predictive values, positive and negative likelihood ratios, and accuracy with the corresponding 95% confidence intervals. Contemplating an option of uncertainty in the multimodal CT results, we built 3 × 2 contingency tables. In 3 × 2 tables, we considered nonevaluable results as negative results, assuming a higher prevalence of a final diagnosis of iCVE.17
All tests were conducted 2-sided, and P values < .05 were considered statistically significant. STATA, Version 15 (StatCorp) and MedCalc (MedCalc Software) were used for all statistical analyses.
RESULTS
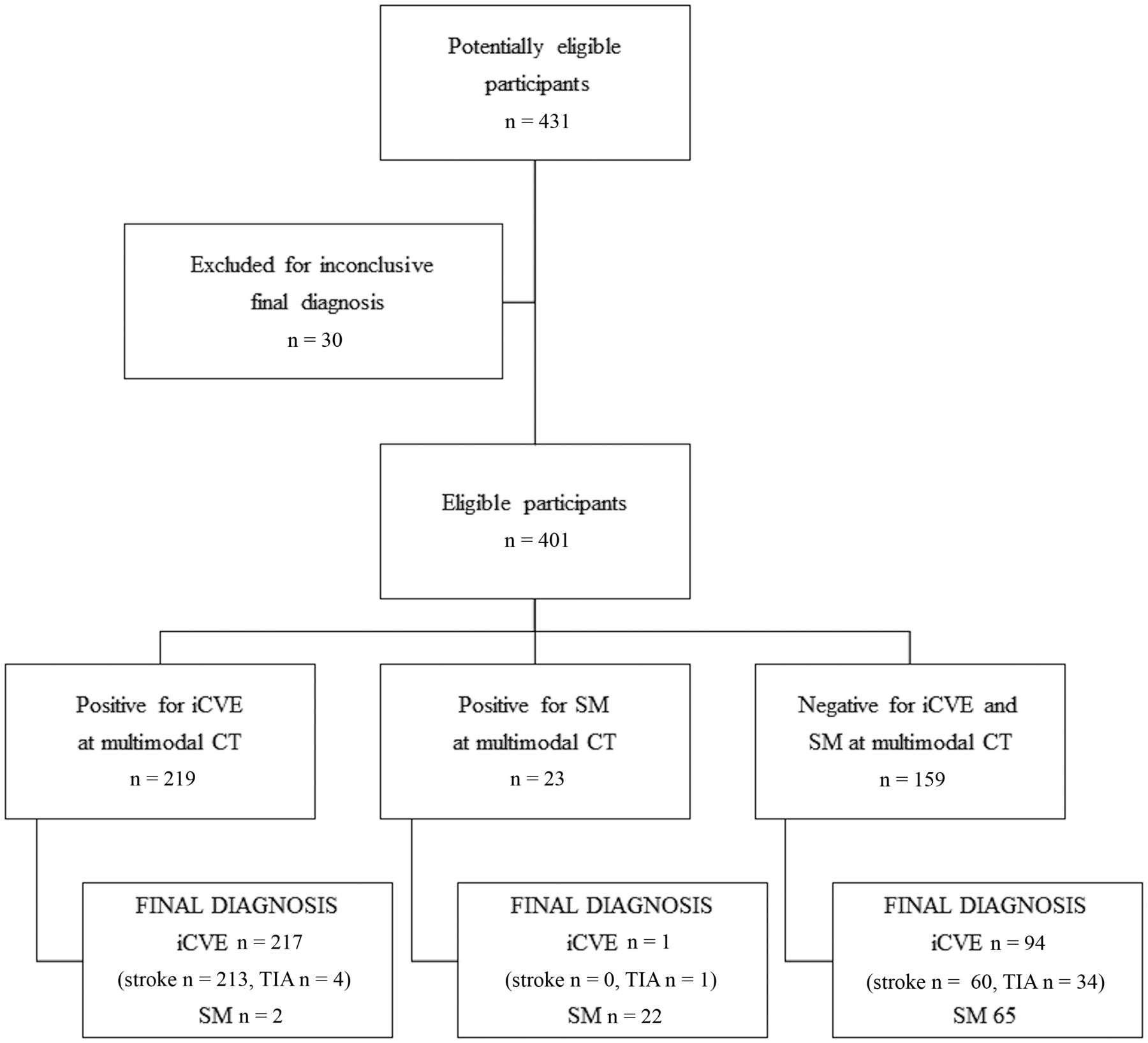
Four hundred thirty-one patients fulfilled the inclusion criteria; 30 patients were excluded from the analysis due to an uncertain final diagnosis. Therefore 401 patients were included in our study population: 219 men and 182 women (mean age, 71 [SD 14] years; range, 25–97 years).
The results of multimodal CT at admission (index test) were categorized as diagnostic of iCVE (n = 219), diagnostic of SM (n = 23), and negative for both iCVE and SM (n = 159).
The clinical final diagnosis (reference standard) was dichotomized into diagnoses of iCVE (n = 312) and SM (n = 89). The iCVEs were further subdivided into diagnoses of stroke (n = 273) and TIA (n = 39) (Fig 1).

Study design diagram.
The sex distribution was similar among different categories of multimodal CT diagnoses (male/female ratios, respectively, 122:97, 15:8, 82:77 for the categories of multimodal CT diagnoses of iCVE and SM, and negative for both iCVE and SM, P = .298) and final diagnoses (male/female ratios, respectively, 180:132 and 39:50 for the final diagnoses of iCVE and SM, P = .087).
Age distribution significantly differed between the categories of final diagnosis, respectively, 73 (SD, 13) years in the final diagnosis of iCVE and 66 (SD, 11) years in the final diagnosis of SM (P = .002).
The prevalence of SM in our population was 22%, including seizures (n = 31, 34.8%), migraine with aura attack (n = 11, 12.4%), conversion disorder (n = 11, 12.4%), infection (n = 7, 7.9%), brain tumor (n = 7, 7.9%), acute metabolic condition (n = 6, 6.7%), peripheral vertigo (n = 5, 5.6%), syncope (n = 5, 5.6%), transient global amnesia (n = 3, 3.4%), subdural hematoma (n = 1, 1.1%), cervical epidural hematoma (n = 1, 1.1%) and dural AVF (n = 1, 1.1%) (Table 1). More specifically, infections included 1 viral undetermined encephalitis and 6 systemic infections; brain tumors were all primitive glial tumors; and metabolic causes included 2 cases of hepatic encephalopathy, 2 cases of drug-related encephalopathy, 1 case of hyponatremia, and 1 case of hypoglycemia.
SM and stroke mimics with diagnostic findings at multimodal CT
Statistical analysis results are shown in Table 2. Multimodal CT sensitivity, specificity, and accuracy for the diagnosis of SM were 24.7% (95% CI, 16.2%–35%), 99.7% (95% CI, 98.2%–100%), and 83% (95% CI, 79%–86.6%), respectively. Multimodal CT revealed peri-ictal changes in 13/31 seizures, 7/7 brain tumors, 1/1 dural AVF, and 1/1 subdural hematoma, while it revealed no relevant abnormal findings in 18/31 seizures, 11/11 migraines with aura attack, 11/11 conversion disorders, 7/7 infections, 5/5 cases of peripheral vertigo, 6/6 metabolic conditions, 5/5 cases of syncope, 3/3 cases of transient global amnesia, and 1/1 cervical epidural hematoma. When we excluded a priori undetectable SM conditions on multimodal CT (conversion disorders, peripheral vertigo, syncope, transient global amnesia), multimodal CT sensitivity, specificity, and accuracy were 33.9% (95% CI, 22.6%–46.7%), 99.7% (95% CI, 98.4%–100%), and 89% (95% CI, 85.6%–91.9%), respectively.
Statistical analysis results
The specificity of multimodal CT for the diagnosis of SM in our study was high: Only 2/85 SM were diagnosed as stroke, and only 1/327 iCVEs was misdiagnosed as a stroke mimic on multimodal CT. More specifically, in 1 case, a subtle cortico-subcortical density was interpreted as a stroke, despite normal findings on perfusion maps, and the final diagnosis was aseptic meningoencephalitis, while 1 other false-positive diagnosis of stroke was derived from an erroneous interpretation of hypoperfusion, non-matching vascular territories such as a watershed hemodynamic hypoperfusion, which was, instead, a postseizure abnormality. The false-positive stroke mimic occurred, instead, in a patient with a vague perfusion asymmetry, which was interpreted as a possible postseizure abnormality, but the final diagnosis was a TIA. No imaging diagnosis of the cervical epidural hematoma was obtained on admission multimodal CT due to subtle and overlooked findings at CTA of the neck.
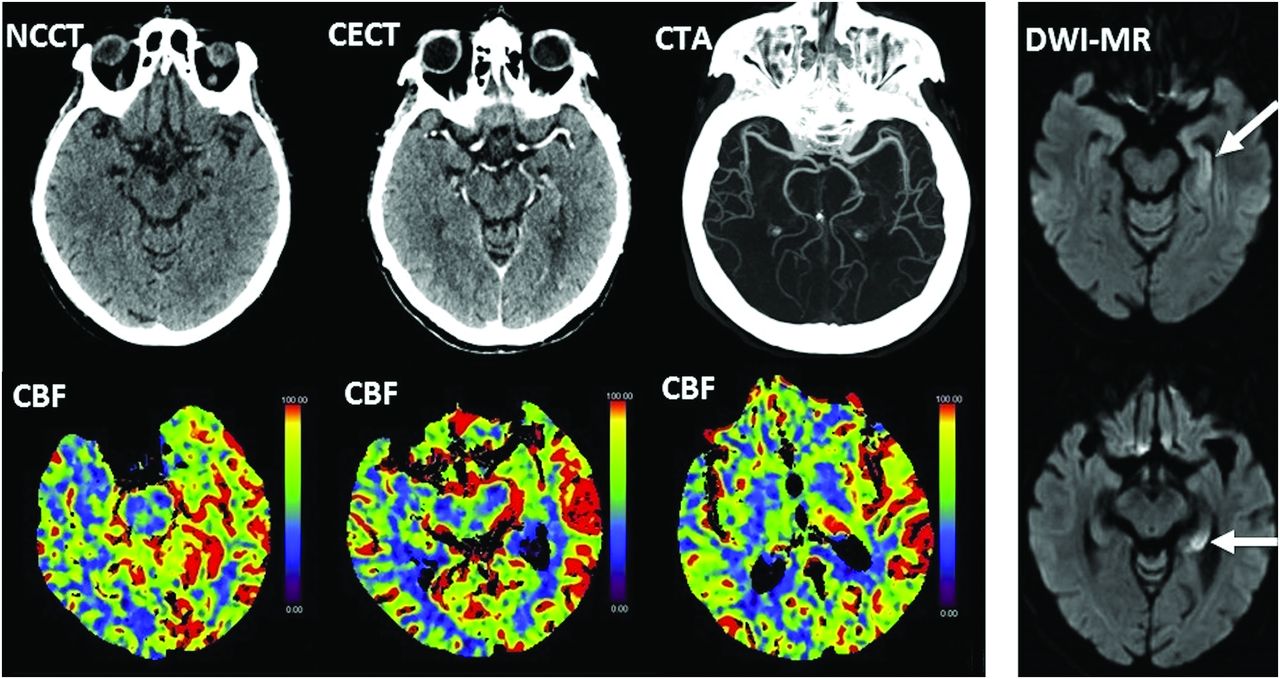
The role of each of the multimodal CT techniques in the diagnosis of a stroke mimic is shown in Table 3. A hyperperfusion pattern (increased CBV and CBF ± reduced MTT/Tmax) was observed in 7/13 seizures and 6/7 tumors (Fig 2 and Online Supplemental Data), while 6/13 seizures and 1/7 tumors showed a hypoperfusion pattern (increased MTT/Tmax ± reduced CBV and CBF) (Online Supplemental Data). While CT + CTA showed positive findings in 41% of detected SM, perfusion CT alone showed positive findings in 95.5% of them.
Table 3: Role of each multimodal CT technique (NCCT, CTA, CTP, CECT) in the diagnosis of SM

Left panel: elevated CBF consistent with hyperperfusion involving the left temporo-occipito-parietal cortex and left pulvinar in a 77-year-old woman with acute right-sided motor impairment, right hemineglect, aphasia, and conjugate eye deviation to the right. Note normal findings on NCCT, CECT, and CTA. Right panel: Diffusion MR imaging excludes ischemia and demonstrates seizure changes (arrows) in the left hippocampus.
We also evaluated the sensitivity, specificity, and accuracy of multimodal CT for the diagnosis of stroke, which were, respectively, 78% (95% CI, 72.6%–82.8%), 97.8% (95% CI, 92.1%–99.7%), and 82.9% (95% CI, 78.6%–86.6%), in line with previous reports.18⇓–20 The sensitivity, specificity, and accuracy of multimodal CT in the diagnosis of total iCVE (stroke and TIA) were, respectively, 69.6% (95% CI, 64.1%–74.6%), 97.8% (95% CI, 92.1%–99.7%), and 75.8% (95% CI, 71.3%–79.9%) (Table 2).
Among 89 patients with SM in our cohort, 82% underwent MR imaging at follow-up. MR imaging determined the diagnosis of SM in only 5 patients, with no relevant findings on multimodal CT (7% of patients with SM examined by MR imaging). Among these, there were patients with transient global amnesia (n = 3) and postictal hippocampal (n = 1) and cortical (n = 1) diffusion restriction. The remainder of the diagnoses of SM were established on the basis of other anamnestic, serologic, CSF, or EEG findings.
DISCUSSION
In this study, we aimed to examine the overall performance of multimodal CT for the diagnosis of SM in the context of clinical suspicion of acute ischemic stroke, demonstrating low sensitivity but high specificity with high positive predictive values and fairly high negative predictive values (respectively, 25.6%, 99.7%, 95.6%, and 83.8%). So far in the literature, the performance of CTP has been assessed mostly with regard to seizure-related SM, with a recent case-control study on a large seizure-related stroke mimic population demonstrating sensitivity, specificity, and positive and negative predictive values, respectively, of 38%, 86%, 42%, and 83% for CTP hyperperfusion in patients with ongoing seizure (ictal state).11
In our population, as in previous studies,6,21 seizure was the most common stroke mimic. We were able to recognize 13/31 (42%) seizures on the basis of perfusion abnormalities on multimodal CT, with a hyperperfusion pattern in 7/13 (54%) and a hypoperfusion pattern in 6/13 (46%). Because in many of our patients, EEG was not obtained at the time of multimodal CT acquisition, it is not possible to correlate these perfusion abnormality patterns with an ictal or postictal state.
Van Cauwenberge et al11 reported that CTP can reliably differentiate acute ischemic stroke from ictal seizure, respectively, characterized by cortico-subcortical hypoperfusion and cortical hyperperfusion. Conversely, they showed that CTP findings may overlap in acute ischemic stroke and postictal seizure, both characterized by cortico-subcortical hypoperfusion, though seizure-related hypoperfusion typically follows a nonvascular distribution. In our study, the specificity of multimodal CT for the diagnosis of SM was high: Only 2/85 SM were diagnosed as stroke, and only 1/327 iCVEs was misdiagnosed as a stroke mimic; 2 of 3 of these misdiagnoses were related to a misinterpretation of hypoperfusion findings, with a postictal seizure erroneously interpreted as a stroke and vice versa. Therefore, our results confirm the potential overlap of CTP findings between postictal hypoperfusion and acute ischemic stroke.
We detected all brain tumors present in our cohort by multimodal CT. Abnormal findings were visible on NCCT and CECT due to the presence of mass effect, vasogenic edema, and/or contrast enhancement. CTP showed hyperperfusion in 6/7 (86%) and hypoperfusion in 1/7 (14%) brain tumors. Perfusion abnormalities in brain tumors may be related to the nature of the lesion, with typical hyperperfusion in high-grade gliomas, or to induced seizure.22
In our cohort, none of the patients with an attack of migraine with aura had recognizable multimodal CT findings, though perfusion abnormalities have been described in migraine, mostly on MR imaging studies demonstrating abnormalities ranging from hypoperfusion to hyperperfusion, with a typical nonvascular distribution,23⇓-25 which can be associated to an increase of distal cortical vessel representation.26
None of the toxic-metabolic conditions or infections in our cohort were detected by multimodal CT, though in these cases, NCCT may variably show areas of hypoattenuation or swelling, with possible contrast enhancement. Perfusion findings have also been anecdotally described in case reports such as in Wernicke encephalopathy,27 Hashimoto encephalopathy,28 and viral infections.29,30
In addition, we did not encounter, in our cohort, luxury perfusion conditions, which may pose a challenge in a differential diagnosis between a postreperfusion iCVE and a stroke mimic. Luxury perfusion represents, in fact, the recovery of CBF to normal or increased levels in regions of infarcted brain when re-vascularization is established after a stroke, sometimes spontaneously. Luxury perfusion commonly occurs in subacute strokes but has also been reported in <24-hour strokes.31
In our study, the sensitivity of multimodal CT for the diagnosis of SM was low (25.6%) and remained low (34.4%; 95% CI, 22.9–47.3), even excluding SM, which are a priori considered to be undetectable by multimodal CT (such as conversion disorder, positional vertigo, syncope, and transient global amnesia). Due to its low sensitivity, multimodal CT cannot, therefore, be considered an efficient diagnostic tool for SM. In our cohort, 82% of SM underwent MR imaging at follow-up, and MR imaging has determined the diagnosis of SM in only 5 patients, with no relevant findings on multimodal CT (7% of SM examined by MR imaging). Although MR imaging allows ruling out stroke and may give a further hint of the diagnosis of SM, the diagnosis of these conditions relies on other complementary tests, such as serum and CSF analysis or EEG findings.
Conversely, our study outlines the high specificity of multimodal CT for the diagnosis of SM. This may support the clinician in the choice of avoiding revascularization treatment in SM with positive findings on multimodal CT. Among the different multimodal CT techniques, CTP was the most useful in the detection of SM, demonstrating abnormal findings in 95.5% of the overall diagnoses of SM performed by multimodal CT. Despite the current debate about the usefulness of CTP in patients with stroke in the first 6 hours from symptom onset,1 CTP has the potential to detect perfusion abnormalities related to stroke mimic conditions and in cases in which brain CT is typically silent, such as in seizures.
Limitations in this study are related to the retrospective type of the analysis and to the relatively small number of subjects, which might have precluded some uncommon SM from being part of our population. There are, indeed, other vascular dysregulation conditions that might have a clinical presentation similar to that of stroke and may show CTP abnormalities, that we did not encounter in this study, such as posterior reversible encephalopathy syndrome32 and reversible cerebral vasoconstriction syndrome.33
Another limitation is related to a selection bias in our study population, because we included only patients who underwent a full multimodal CT protocol at admission. We, therefore, excluded either patients with iCVE or those with SM without a multimodal CT protocol (ie, patients transferred from neighboring hospitals where CTP was not performed in the acute setting). Also, patients with a very high clinical suspicion of SM (such as those with hypoglycemia, positional vertigo, and migraine) might not have been referred to the multimodal CT protocol. Nonetheless, the prevalence of SM in our cohort was 21%, within the range of previous reports.4,34 Subjects with a final diagnosis of SM were younger than those with a final diagnosis of iCVE, and this difference was statistically significant. This finding is in line with the expected epidemiology of patients with SM. Indeed, clinical indicators of a mimic condition, though nonspecific, include young age and lack of a history of hypertension, hyperlipidemia, atrial fibrillation, diabetes, and coronary artery disease.21 Moreover, some patients with minor stroke who presented at admission as having a TIA, with complete symptom regression, did not undergo a full multimodal CT protocol and were, therefore, excluded from the study.
Finally, this was a monocentric study, and it may limit the generalizability of our findings. In particular, our series benefitted from consultant neurology review before imaging and a subspecialist neuroradiology review at time of imaging.
CONCLUSIONS
Multimodal CT has a low sensitivity for the diagnosis of SM. MR imaging and further investigation (serum and CSF analysis and EEG) are required to obtain a definite diagnosis of these conditions. On the contrary, the high specificity of multimodal CT for the diagnosis of stroke mimic can support the clinician in the choice of avoiding revascularization treatment in patients diagnosed with SM on multimodal CT.
Acknowledgments
We thank Matteo Merli, Istituto Imaging della Svizzera Italiana, Ente Ospedaliero Cantonale, Lugano, Switzerland, for CT technical support; and the Clinical Trial Unit, Ente Ospedaliero Cantonale, Bellinzona, Switzerland, for assistance in research project development.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Carlo W. Cereda and Alessandro Cianfoni contributed equally to this work.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received June 22, 2021.
- Accepted after revision October 6, 2021.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}