
Article Figures & Data
Figures
- FIG 1.
Common biopsy approaches to H&N lesions at different levels of the suprahyoid (A) and infrahyoid neck (B). Note that to avoid the parotid gland, one should use a retromandibular approach for more inferior retropharyngeal, parapharyngeal, pharyngeal mucosal, and masticator space lesions; more superior lesions are better accessed via paramaxillary and subzygomatic approaches. Reprinted with permission of Mayo Foundation for Medical Education and Research, all rights reserved. PG indicates parotid gland; T, tumor; LT, lingual tonsil.
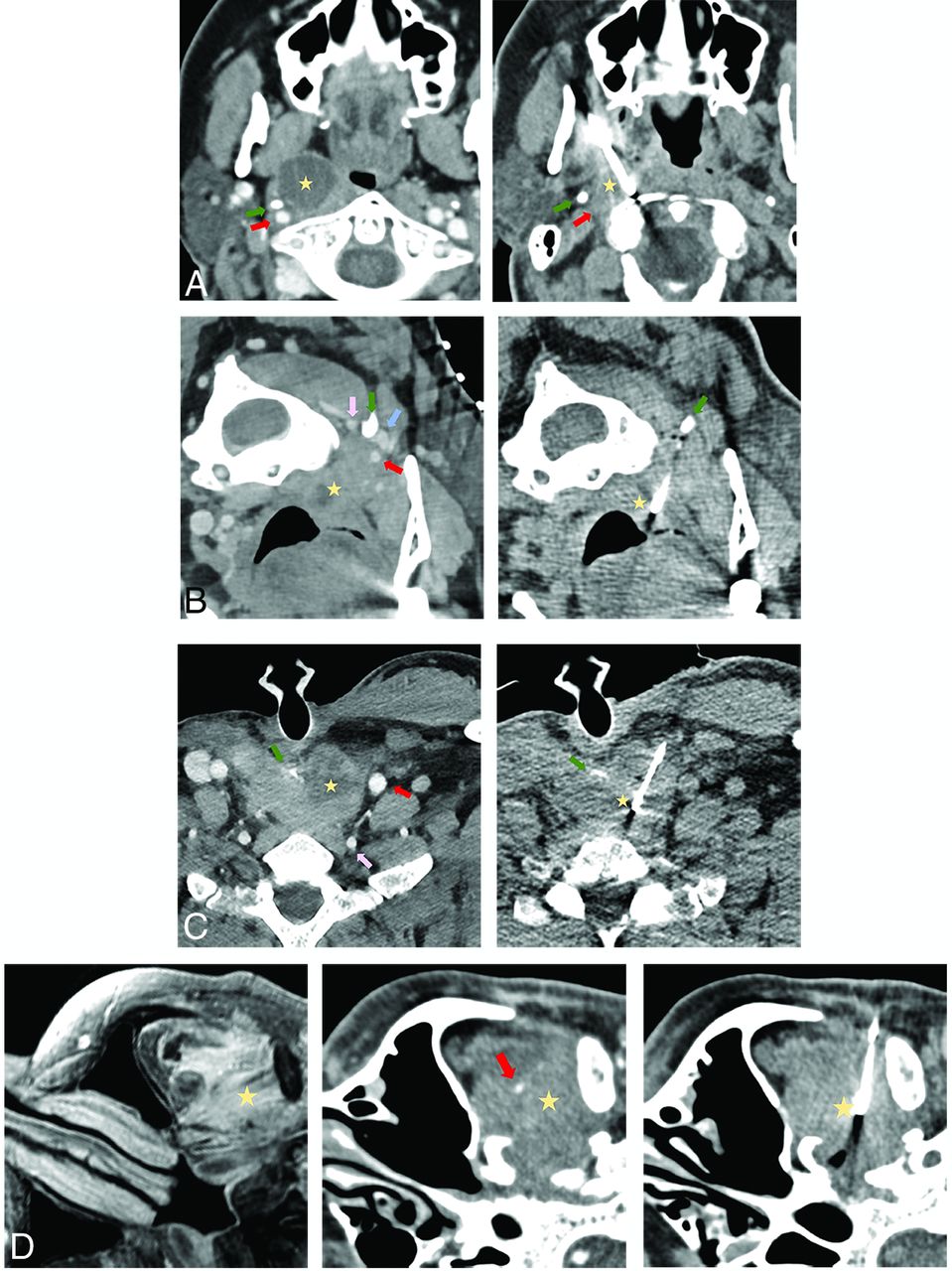
- FIG 2.
Common approaches used in the current series biopsy. A, A paramaxillary approach targeting a 1.9-cm partially cystic right retropharyngeal lymph node (yellow star). Left, Preprocedural contrast-enhanced CT (venous phase) to better visualize the right ICA (red arrow) and better assess lesion margins due to peripheral enhancement. Right, Intraprocedural CT with a 14-ga needle trough through the lesion (part of the cystic component was initially aspirated). The styloid process (green arrow) is a useful landmark because it is immediately anterior to the ICA. Recurrent human papillomavirus (HPV) + SCC. This approach is commonly used to access retropharyngeal, parapharyngeal, pharyngeal mucosal, masticator, and deep parotid space lesions. B, A retromandibular approach in a patient in a prone position targeting a 1.1-cm partially cystic left retropharyngeal lymph node (yellow star). Left, Contrast-enhanced CT (venous phase) to better visualize the left ICA (red arrow), vertebral artery (pink arrow), and internal jugular (IJ) vein (blue arrow) and highlight more solid lesion portions. Right, Intraprocedural CT with a 16-ga needle trough through the solid portion of the lesion. The C1 transverse process (green arrow) is a useful landmark because it “marks a safe pass” between the vertebral artery posterior to the needle and the ICA/IJ vein anteriorly. Recurrent HPV + SCC. This approach can be used for more inferior retropharyngeal, parapharyngeal, pharyngeal mucosal, masticator, and deep parotid lesions, as well as sublingual, submandibular, perivertebral, and carotid space lesions. C, Anterior approach targeting a 3.4-cm partially cystic nodule at the tracheoesophageal groove (yellow star). Left, Preprocedural contrast-enhanced CT (venous phase) to opacify the left common carotid artery (red arrow) and vertebral artery (pink arrow) and delineate the solid component of the target lesion. Right, Intraprocedural CT with an 18-ga needle trough through the solid component of the lesion. A partially visualized esophageal stent (green arrow) is a useful landmark showing the approximate location of the infiltrated esophagus, lateral to the stent. Recurrent SCC. This approach is used with a neutral supine position for more midline anterior neck lesions such as the visceral space, level VI, and the supraclavicular lymph nodes. D, A subzygomatic approach targeting an infiltrating left masticator space mass seen on MR imaging (left image, yellow star). Middle, Preprocedural contrast-enhanced CT (venous phase) to opacify the left internal maxillary artery (red arrow). Right, Intraprocedural CT with an 18-ga needle trough through the infiltrating lesion with the biopsy device clearly posterior to the expected location of the internal maxillary artery in correlation with the middle image. Recurrent SCC with perineural spread. By far, masticator space lesions are the most common targets for this approach.
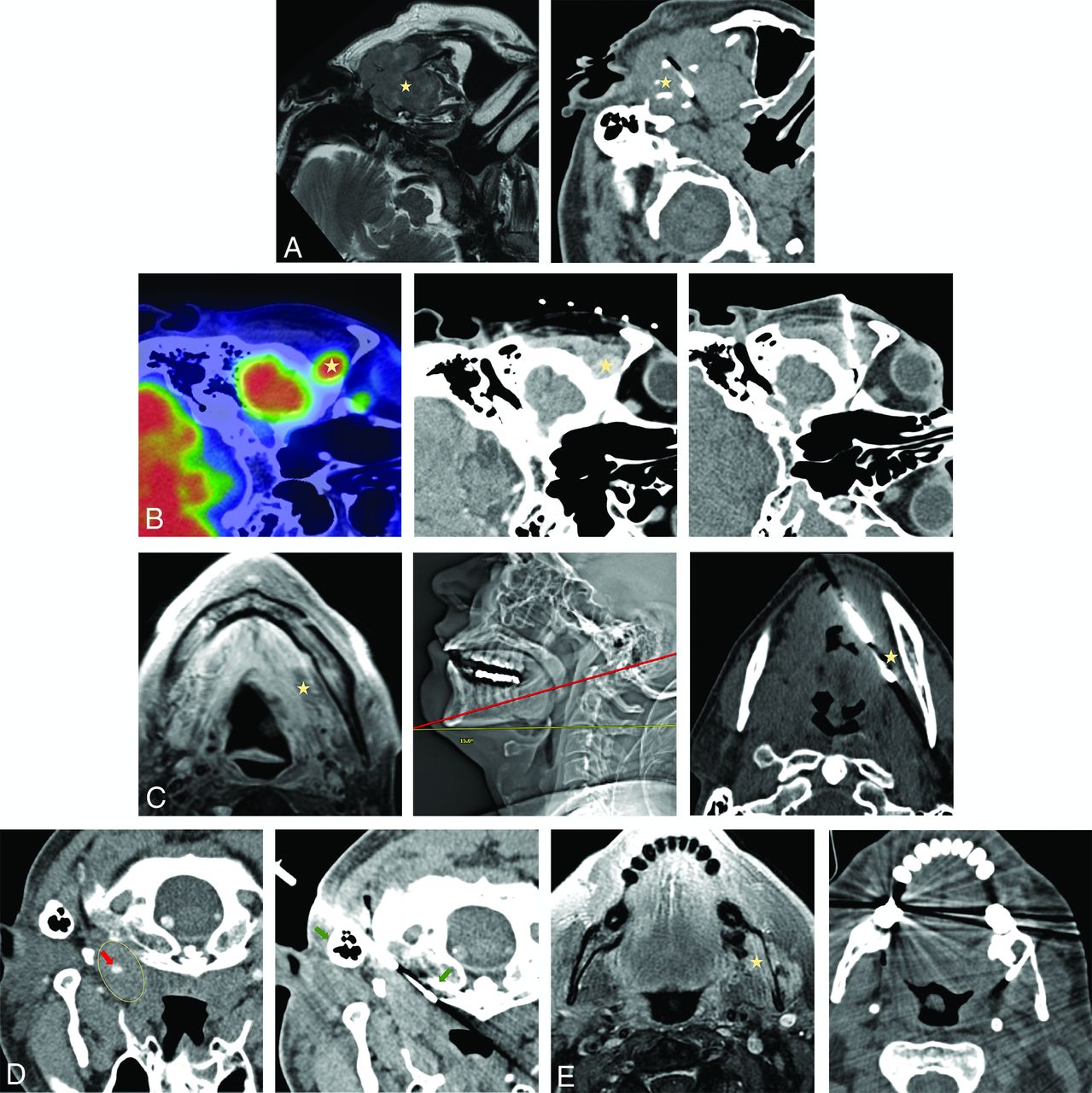
- FIG 3.
Less commonly used biopsy approaches. A, Preauricular approach targeting a 4.2-cm expansile left mandibular lesion with an extraosseous soft-tissue component on MR imaging (left image, yellow star). No preprocedural contrast was administered given the size of the lesion and the lack of proximity of the crucial neurovascular structures. Right, Intraprocedural CT with a 16-ga needle trough through the lesion. Plasmacytoma. This approach is used for superficial lesions in the masticator or superficial parotid space, particularly when a zygoma is partially destructed. B, A suprazygomatic approach targeting hypermetabolic on PET/CT 1.5 -cm right suprazygomatic masticator mass (left image, yellow star). Middle, Preprocedural contrast-enhanced CT (venous phase) to delineate the lesion (yellow star) that enhances more than background tissues. Right, Intraprocedural CT with a 16-ga needle trough through the expected location of the lesion in correlation with bony landmarks and previous contrast enhancement on the middle image. Recurrent adenoid cystic carcinoma. This approach is essentially exclusively used for superficial suprazygomatic masticator space (temporal fossa) lesions. C, Submental approach targeting diffusely heterogeneously enhancing on MR imaging left sublingual/floor of the mouth soft-tissue (left image, yellow star). Middle, Intraprocedural scout CT image showing patient positioning and a cranial gantry tilt of 15° (red line, biopsy plane after 15° gantry tilt) to bypass a mental protuberance. Right, Intraprocedural axial CT with a 14-ga needle trough through the expected location of the target (yellow star). Preprocedural contrast was not administered due to regional vasculature paucity in correlation with prior imaging. Recurrent adenoid cystic carcinoma. Sublingual space and floor of the mouth lesions can be accessed via this approach; to avoid the mental protuberance, cranial gantry tilt and/or substantial neck extension might be needed. D, A retromastoid approach with the patient in the prone position targeting a 2.6-cm left retropharyngeal mass (left image, yellow ellipse), encasing the ICA on preprocedural limited CTA (red arrow). Right, intraprocedural CT with a 16-ga needle advanced between mastoid tip and the C1 anterior arch (right image, green arrows); these osseous landmarks align a safe trajectory into the lesion portion posterior to the ICA in correlation with preprocedural CTA. Recurrent human papillomavirus + SCC. This approach can be used for more lateral retropharyngeal and anterior perivertebral lesions. E, A transosseous approach targeting an enhancing 2.5-cm left masticator mass expanding the mandibular canal on MR imaging (left image, yellow star). Right, Intraprocedural CT scan with a 16-ga needle traversing the buccal cortex of the mandibular ramus. Preprocedural contrast was not administered given lack of critical regional vasculature in correlation with MR imaging. Recurrent adenoid cystic carcinoma with inferior alveolar perineural spread. This approach can be used to access lesions along the inner cortex of the mandible and zygoma.
- FIG 4.
A, PET/CT with hypermetabolic left retropharyngeal 6-mm lymph node (yellow arrow). B, This lesion is centrally cystic/necrotic on follow-up contrast-enhanced CT (yellow arrow) and immediately medial to the ICA (red arrow). C, Intraprocedural CT without contrast with an 18-ga needle advanced via a paramaxillary approach anterior to the target retropharyngeal lymph node (yellow arrow) and medial to the expected location of the unopacified ICA (red arrow). Before further needle advancement, 60 mL of Omnipaque-300 was slowly infused at a rate of 0.6 mL/s to continuously opacify the ICA (red arrows) for adequate visualization before (D) and during (E) lesion sampling (yellow arrows). Pathology reported poorly differentiated metastatic carcinoma in a patient with a history of oropharyngeal human papillomavirus + SCC.





Tables
Patients’ Characteristics and Lesion Management No. % Initially “negative for malignancy” biopsies 43/184 23% Patients with a known malignancy 29/43 68% Rebiopsied/excised 7/29 20% Ultimately +malignancy 4/7 57% Stable/resolved (mean f/u time: 32 mo, 2–120 mo) 17/29 59% No f/u 5/29 17% Patients without known malignancy 14/43 32% Rebiopsied/excised 5/14 36% Ultimately + malignancy 0/5 0% Stable/resolved (mean f/u time: 25.6 mo, 1–72 mo) 7/14 50% No f/u 2/14 14% Total false-negative rate 4/184 2% Total diagnostic yield 167/184 91% Note:—f/u indicates follow-up.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}