
Abstract
BACKGROUND AND PURPOSE: Racial and socioeconomic disparities in the incidence, treatment, and outcomes of acute ischemic stroke exist and have been described. We aimed to characterize disparities in the use of endovascular thrombectomy in a nationally representative analysis.
MATERIALS AND METHODS: Discharge data from the Nationwide Inpatient Sample between 2006 and 2016 were queried using validated International Classification of Disease codes. Patients admitted to US hospitals with acute ischemic stroke were included and stratified on the basis of race, income, and primary payer. Trends in endovascular thrombectomy use, good outcome (discharge to home/acute rehabilitation), and poor outcome (discharge to skilled nursing facility, hospice, in-hospital mortality) were studied using univariate and multivariable analyses.
RESULTS: In this analysis of 1,322,162 patients, endovascular thrombectomy use increased from 53/111,829 (0.05%) to 3054/146,650 (2.08%) between 2006 and 2016, respectively. Less increase was observed in black patients from 4/12,733 (0.03%) to 401/23,836 (1.68%) and those in the lowest income quartile from 10/819 (0.03%) to 819/44,984 (1.49%). Greater increase was observed in the highest income quartile from 18/22,138 (0.08%) to 669/27,991 (2.39%). Black race predicted less endovascular thrombectomy use (OR = 0.79; 95% CI, 0.72–0.86). The highest income group predicted endovascular thrombectomy use (OR = 1.24; 95% CI, 1.13–1.36) as did private insurance (OR = 1.30; 95% CI, 1.23–1.38). High income predicted good outcome (OR = 1.10; 95% CI. 1.06–1.14), as did private insurance (OR = 1.36; 95% CI, 1.31–1.39). Black race predicted poor outcome (OR = 1.33; 95% CI, 1.30–1.36). All results were statistically significant (P < .01).
CONCLUSIONS: Despite a widespread increase in endovascular thrombectomy use, black and low-income patients may be less likely to receive endovascular thrombectomy. Future effort should attempt to better understand the causes of these disparities and develop strategies to ensure equitable access to potentially life-saving treatment.
ABBREVIATIONS:
- AIS
- acute ischemic stroke
- ECI
- Elixhauser Comorbidity Index
- EVT
- endovascular thrombectomy
- ICD
- International Classification of Disease
- NIS
- Nationwide Inpatient Sample
Ischemic stroke is one of the leading causes of death and disability.1 IV rtPA remains the criterion standard in acute treatment of acute ischemic stroke (AIS).2 After a number of randomized controlled trials demonstrated its effectiveness, endovascular thrombectomy (EVT) has emerged as standard of care for large-vessel occlusions of the anterior circulation within 6 hours of symptom onset and up to 24 hours for selected patients.2⇓⇓⇓-6
Socioeconomic and racial disparities in stroke prevalence and treatment have been studied extensively and documented in the literature. Black and Hispanic patients have a higher burden of stroke and are more likely to experience stroke earlier in life than white patients.1,7⇓-9 Black patients are less likely to receive IV rtPA than white patients,10 more commonly receive inferior in-hospital stroke care including longer wait times in the emergency department,11 have lower odds of receiving a door-to-CT time of <25 minutes, and have decreased likelihood of obtaining cardiac monitoring, dysphagia screening, and smoking-cessation counseling.10,12,13
Also, a few studies have studied disparities in EVT. Rinaldo et al14 demonstrated that in 2016–2018, black and Hispanic patients were less likely to receive EVT than white patients. A recently published study using the Nationwide Inpatient Sample (NIS) also demonstrated similar findings of a racial disparity in EVT use.15 However, this study period was limited to the time before the introduction of EVT as a standard of care for AIS in 2015; thus, we have little understanding of how disparities in EVT have changed from a longitudinal perspective that includes data collected after publication of the major EVT trials.
We aimed to study the trends in both socioeconomic and racial disparities in the use of EVT during a longitudinal period of time including the years following the mainstream acceptance of EVT as standard of care for AIS in a nationally representative administrative data base. As conversations surrounding implicit bias, health care infrastructure, and the funding of culture health care evolve, it is our hope that providing further data will guide interventions designed to achieve equality.
MATERIALS AND METHODS
Data Source
The NIS is the largest publicly available all-payer health care data base. It assesses 20% of all discharges from US hospitals, including approximately 7 million discharges annually and 35 million discharges annually when weighted. A broad range of patient information includes patient-level demographics, discharge diagnoses, procedures performed during admission, and hospital-level demographics. All data in the NIS, including the specific exposures and outcomes of interest, are provided by the included hospitals and are abstracted from discharge and other administrative documentation. Patients admitted between 2006 and 2016 with the diagnosis of AIS were selected. Inclusion criteria were the diagnosis of AIS; no strict exclusion criteria were applied. EVT and AIS and other diagnoses were identified using the International Classification of Disease, Ninth Revision (ICD-9) and the International Classification of Disease, Tenth Revision (ICD-10) codes. For AIS, ICD-9 codes 433–435 and ICD-10 codes I61, I63, and I64 were used. For EVT, ICD-9 procedure code 39.74 and ICD-10 procedure codes 03CG3Z7, 03CG3ZZ, 03CG4ZZ, 03CK3Z7, 03CK3ZZ, 03CL3Z7, 03CL3ZZ, 03CM3Z7, 03CM3ZZ, 03CN3Z7, and 03CN3ZZ, were used, as per prior studies.16,17 No institutional review board approval was necessary because the NIS is a de-identified data base.
Outcome
The primary outcome of the analysis was EVT use, which was determined by whether a patient who had an ICD-9 or ICD-10 code for AIS also had a procedural code for EVT. Secondary outcomes included having a good outcome, which was defined by discharge to home or an acute rehabilitation hospital. Poor outcome was defined as discharge to a skilled nursing facility, hospice, or in-hospital mortality. Although mortality was included within the poor outcome category, mortality was used as its own secondary outcome as well because it was thought to be an important outcome metric in and of itself. Prior studies have demonstrated that discharge disposition is correlated with functional status in patients with stroke.18
Covariables
Information regarding median household income, primary payer, age, sex, and race is included in the NIS data base. Age was approached as a continuous variable rather than using discrete age groups. The sex variable included male and female. The race variable provided by the NIS combines both race and ethnicity into 1 variable and includes white, black, Hispanic, Asian or Pacific Islander, Native American, or Other. Median household income was broken down into 4 categories based on national percentiles: Quartile 1 included patients whose income fell within the 0 to 25th percentiles. Quartile 2 included patients whose income fell within the 26th to 50th percentiles. Quartile 3 included patients whose income fell within the 51st to 75th percentiles. Last, quartile 4 included patients whose income fell within 76th to 100th percentiles. The NIS estimates this information on the basis of the participant’s ZIP code. Primary payer information was broken down into those patients with Medicare, Medicaid, private insurance, self-pay, no charge, or other. The “Other” payment category includes Workers’ Compensation, Civilian Health and Medical Program of the Uniformed Services, Civilian Health and Medical Program of the Department of Veterans Affairs, Title V, and other governmental programs. We additionally included hospital size (small, medium, large) as provided by the NIS. Last, we used ICD-9 and ICD-10 diagnosis codes to include covariates related to outcome such as tracheostomy and gastrostomy. Administration of IV rtPA was determined using ICD-9 procedural code 99.10 and ICD-10 procedural code 3E03317. The Elixhauser Comorbidity Index (ECI), a validated list of comorbidities that predict patient outcomes using ICD-9 and ICD-10 data,19 was compiled. The aggregate number of Elixhauser comorbidities for each patient was used as a surrogate for their comorbidity burden. ICD-9 codes were used for 2006 up through the third discharge quarter of 2015. ICD-10 codes were used for the fourth discharge quarter of 2015 through 2016.
Statistical Analysis
Descriptive analyses were performed by comparing the number and percentage of each variable in the group that underwent EVT with the corresponding patients who did not undergo EVT. These were presented as the total number and percentage. Univariate comparisons between these groups were performed using a χ2 test for categoric variables and the 1-sample t test for continuous variables. Trend analyses were performed by determining numbers and percentages of each variable for every year in the sample. Univariate logistic regression was used to determine whether the trend was statistically significant.
Four survey-weighted multivariate logistic regression analyses were performed. Variables were included in the multivariable analysis if they emerged as statistically significant in the univariate comparisons, were not missing significant amounts of data, were of clinical interest, and were biologically/clinically feasible. The dependent variable for the first analysis was EVT use; this analysis was performed to determine which variables were independently predictive of EVT use. This analysis included the year as a continuous variable; adjusting for this allowed us to determine whether the longitudinal trends in use were significant when stratifying by individual race/ethnicity. The dependent variable for the second 2 analyses was patients having a good outcome and poor outcome after EVT, respectively. Finally, a multivariable logistic regression analysis was performed with the outcome of in-hospital mortality.
RESULTS
Patient Demographics
In our sample of 1,322,162 patients who had AIS between 2006 and 2016, the average age of our population was 72 years. Fifty-two percent of the patients were women; most (62%) of the patients were white, with the primary payer as Medicare (66%) (Table). There was a fairly equal distribution of income levels among our patient population, with all 4 income groups containing between approximately 19% and 30% of our patient population each. The median ECI sum for our entire patient population was 3. The average age of White patients (72.45 years) was higher than that of black (64.29 years) and Hispanic (66.02 years) patients (Online Supplemental Data). Additionally, women, on average, were older (72.68 years) than men (67.91 years).
Demographic information stratified by EVT status
Comorbidities
When we stratified for race (Online Supplemental Data), white patients had a lower percentage of cardiovascular risk factors such as diabetes and hypertension (diabetes, 29.73%; hypertension, 74.57%) compared with black (diabetes, 42.50%; hypertension, 82.91%) and Hispanic (diabetes, 46.24%; hypertension, 77.73%) patients. Black patients had the highest proportion of smokers (20.27%) compared with the other races. Additionally, white patients had the highest rate of cardiac arrhythmias (35.41%) compared with black (22.83%) and Hispanic (25.79%) patients.
When we stratified on the basis of income (Online Supplemental Data), the percentage of patients with diabetes and hypertension and those who were smokers was inversely proportional to the increasing income quartiles. The percentage of patients with cardiac arrhythmias was directly proportional to the increasing income quartiles.
Income and Insurance Disparities
When we stratified by race (Online Supplemental Data), a greater proportion of black and Hispanic patients were in the lowest quartile (52.70% and 40.01%, respectively) compared with white patients (25.03%). The proportion of black and Hispanic patients was inversely proportional to increasing income quartile, with the lowest percentage of patients occupying the highest income quartile (10.39% and 13.89%, respectively). In white patients, there was no such trend in the distribution of income quartiles. A total of 22.58% of white patients were in the highest income quartile.
When we stratified by insurance, 41.80% of patients with Medicare were white, while 31.29% of patients were black and 16.35% were Hispanic. In patients with private insurance, 68.83% of patients were white, while 17.31% were black and 7.19% were Hispanic, suggesting that white patients were more likely to have private insurance than black or Hispanic patients.
When we stratified by sex, women were more likely to have Medicare (71.38%) than men (60.34%), whereas men were more likely to have private insurance (22.43%) than women (16.10%).
Trends in EVT Use
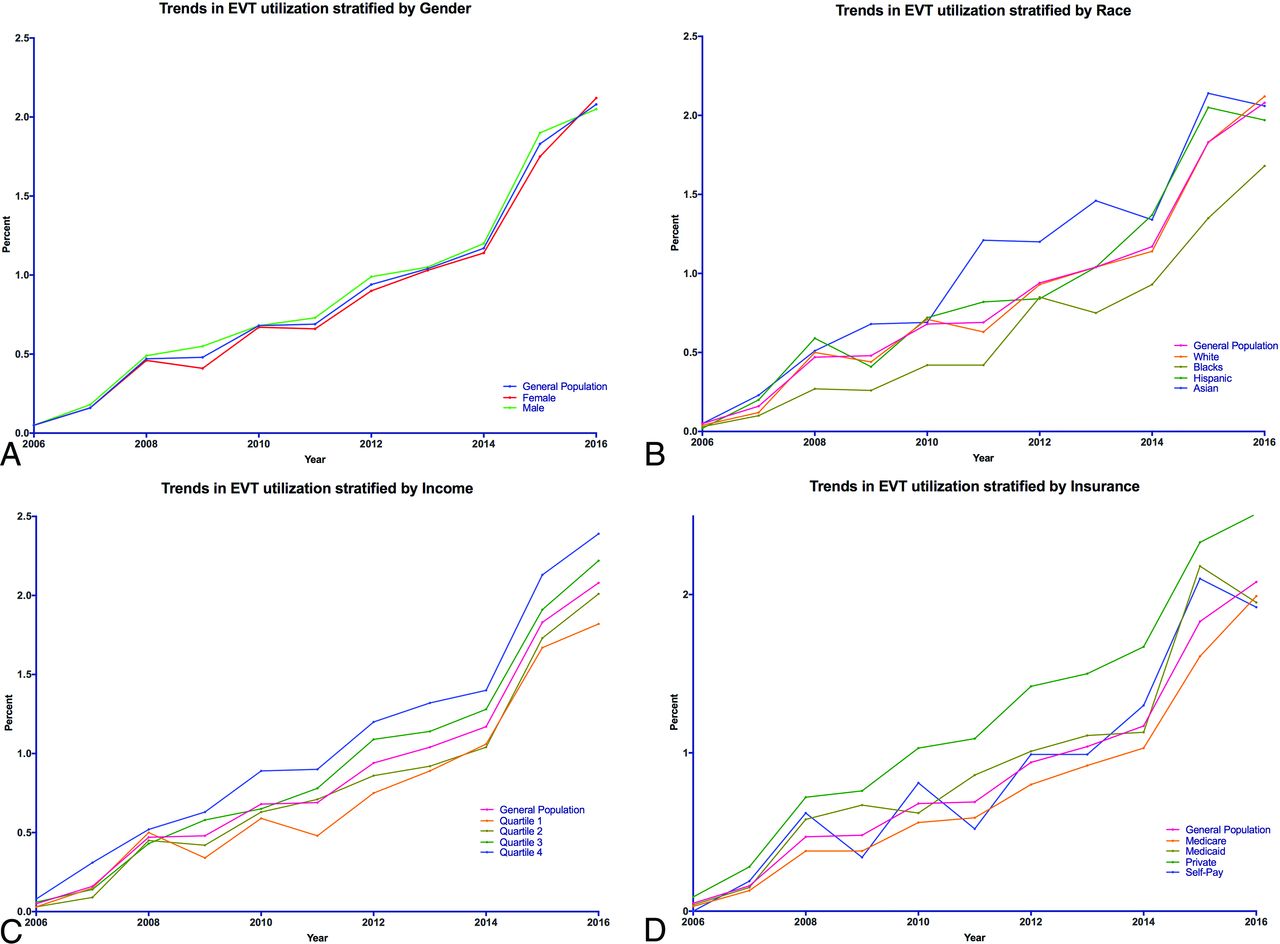
There was a notable increase in EVT use between 2006 and 2016, with 0.05% of all patients with AIS undergoing EVT in 2006, increasing linearly to 2.08% in 2016. (Fig 1). Similar trends were observed when stratifying for sex (Fig 1A) because both men and women had nearly identical rates of increase. When stratifying by race (Fig 1B), the rate of increase in EVT use in White patients nearly mirrored that of the general population, increasing from 0.04% in 2006 to 2.12% in 2016, while the rate of increase in black patients was notably lower (0.03% in 2006 to 1.68% in 2016). When we stratified by income (Fig 1C), those patients in the highest income quartile had a rate of increase that was markedly higher than that of the general population, increasing from 0.08% in 2006 to 2.39% in 2016, while the use of EVT in those patients in the lowest income quartile had a rate of increase that was notably lower (0.03% in 2006 to 1.49% in 2016). Last, we stratified trends in EVT use on the basis of primary payer (Fig 1D), and a markedly increased rate in the use of EVT in patients with private insurance was observed compared with that of the general population, from 0.09% in 2006 to 2.51% in 2016. The lowest increase was observed in the Medicaid group, which increased from 0.03% in 2006 to 1.95% in 2016.

Trend graphs demonstrating the use of EVT in patients stratified by sex, race, insurance, and income. Higher income and private insurance demonstrate a greater increase in the rates of use of EVT than lower income groups and other types of insurance including Medicare and Medicaid. Black race has a lower increase in the rate of use of EVT than the general population as well as other races.
Predictors of EVT Use
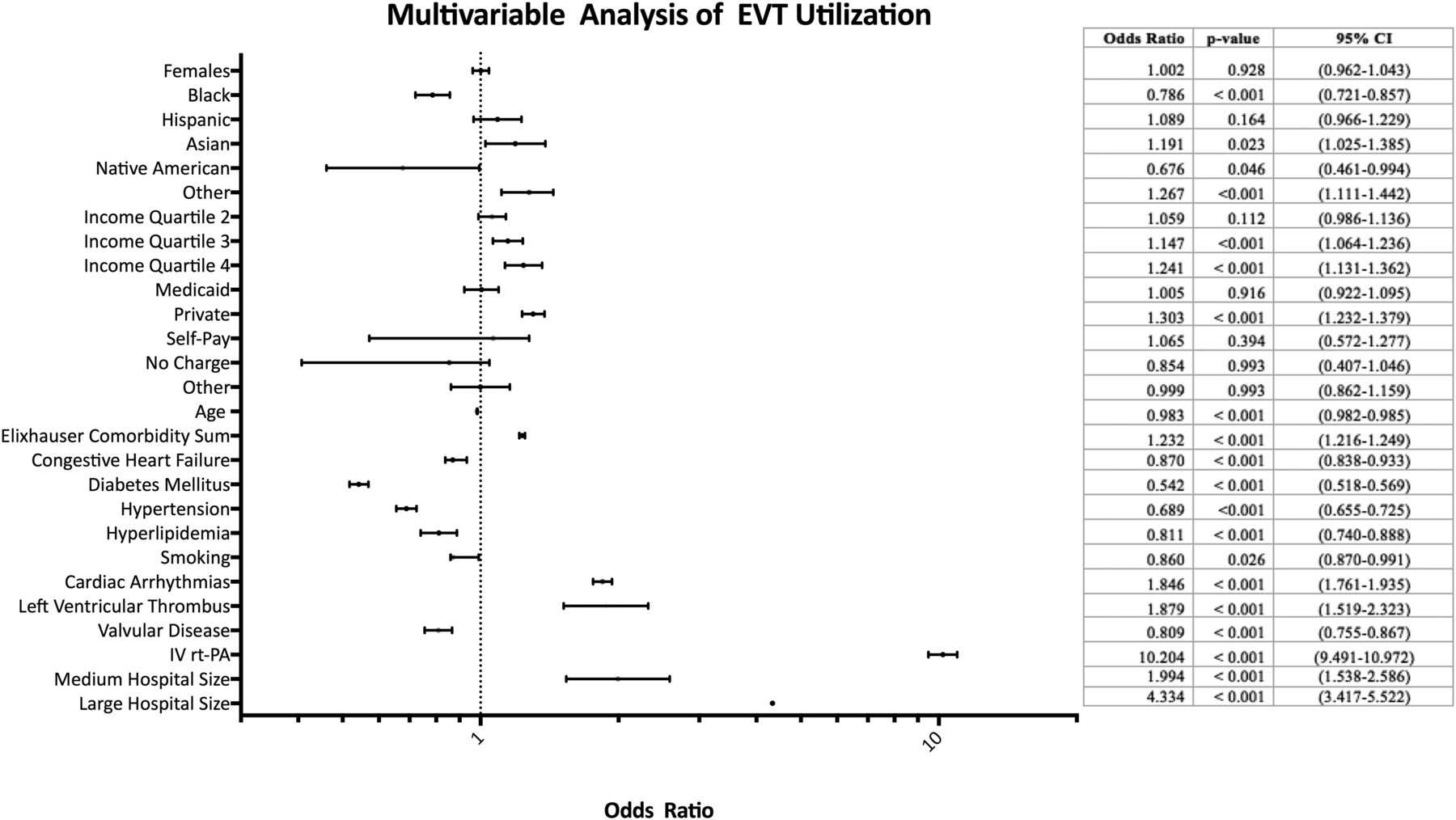
We performed multivariable logistic regression (Fig 2), adjusted for race, income, primary payer, demographic variables, and other potential confounders, including age, ECI sum, congestive heart failure, diabetes mellitus, hypertension, hyperlipidemia, smoking, cardiac arrhythmias, left ventricular thrombus, valvular disease, IV rtPA, and hospital size. In this model, black race was found to be an independent predictor of less frequent use of EVT (OR = 0.79; 95% CI, 0.72–0.86). Increasing income trended toward predicting EVT use, with the highest income quartile independently predicting EVT use (OR = 1.24; 95% CI, 1.13–1.36). Private insurance additionally independently predicted EVT use (OR 1.30; 95% CI, 1.23–1.38). As might be expected, cardiac arrhythmias and left ventricular thrombus were independent predictors of EVT use (OR = 1.85; 95% CI, 1.76–1.94; OR = 1.88; 95% CI, 1.52–2.32, respectively). Additionally, increasing hospital size independently predicted EVT use, with the large hospital size demonstrating the greatest effect (OR = 4.33; 95% CI, 3.42–5.52). All reported findings are statistically significant, with P value <.01, accounting for the large sample size used.

Multivariable regression analysis of predictors of EVT. Notably, black race has a statistically significantly lower odds ratio of EVT use. Private insurance is associated with higher odds of EVT use. Sequentially higher odds ratios of EVT are observed with each level of increasing income. Small-vessel disease risk factors such as hyperlipidemia, diabetes, and smoking are associated with decreased EVT use. Cardioembolic risk factors such as cardiac arrhythmias and left ventricular thrombus are associated with higher rates of EVT use. Increasing hospital size is also associated with increased use of EVT. For analysis of race/ethnicity, the reference category is white race. For income quartiles, the reference variable is income quartile 1. For hospital size, the reference category is small hospital size. For insurance type, the reference category is Medicare.
Predictors of Outcome
Multivariable logistic regression of good outcome (Fig 3), poor outcome, and in-hospital mortality was performed. Models were adjusted for race, income, primary payer, demographic variables, and other potential confounders, including age, ECI sum, congestive heart failure, diabetes mellitus, hypertension, hyperlipidemia, smoking, cardiac arrhythmias, left ventricular thrombus, valvular disease, IV rtPA, and hospital size. Predictors of good outcome included increasing income, with the median household income quartile 4 most strongly predicting good outcome (OR = 1.101; 95% CI, 1.06–1.14). Private insurance additionally independently predicted good outcome (OR = 1.36; 95% CI, 1.31–1.39).

Multivariable regression analysis of predictors of good outcome following EVT. Female sex is associated with decreased odds of good outcome, as was black race. Increasing income quartile is associated with increased odds of good outcome. Private insurance is associated with increased odds of good outcome. An increasing Elixhauser Comorbidity sum is associated with decreased odds of good outcome. For analysis of race/ethnicity, the reference category is white race. For income quartiles, the reference variable is income quartile 1. For hospital size, the reference category is small hospital size. For insurance type, the reference category is Medicare.
Black race was an independent predictor of poor outcome (OR = 1.328; 95% CI, 1.298–1.358). Increasing age (OR = 1.039; 95% CI, 1.038–1.039) and increasing ECI sum (OR = 1.438; 95% CI, 1.431–1.445) additionally were independent predictors of poor outcome. Additionally, female sex appeared to be predictive of worse outcome following EVT (OR = 1.214; 95% CI, 1.203–1.225).
Hispanic ethnicity predicted in-hospital mortality with small-but-detectable odds (OR = 1.055; 95% CI, 1.021–1.090). Paradoxically, while congestive heart failure predicted in-hospital mortality (OR = 1.289; 95% CI, 1.265–1.314), diabetes mellitus (OR = 0.619; 95% CI, 0.607–0.630), hypertension (OR = 0.374; 95% CI, 0.368–0.381), and hyperlipidemia (OR = 0.511; 95% CI, 0.493–0.530) were associated with lower odds of in-hospital mortality. Similar findings were seen in the multivariable regression model for poor outcome because diabetes, hypertension, hyperlipidemia, and smoking appeared to decrease the odds of poor outcome. All reported findings are statistically significant, with P value < .01, accounting for the large sample size used.
DISCUSSION
Our study demonstrates that there may have been persistent racial and socioeconomic disparities in use of EVT in the past decade despite an overall increase of EVT in the general population. In our large population of >1 million patients with acute ischemic stroke, we found that black and low-income patients were less likely to receive EVT compared with white patients with higher income and private insurance. These findings are consistent with prior studies. Esenwa et al15 also demonstrated, in a study of the NIS, that black patients were less likely to receive EVT compared with patients of other races. Rinaldo et al14 also demonstrated, in a large data base, that patients with commercial insurance were more likely to receive EVT and were more likely to be white rather than black or Hispanic. Multiple theories for this disparity have been postulated. One theory is that the underlying mechanism of stroke in blacks and Hispanic individuals, as well as patients in lower income populations, is more frequently from small-vessel atherosclerosis, whereas the mechanism in white and higher income patients is often cardioembolic.20⇓-22 Our study does, in fact, demonstrate a greater prevalence of cardiovascular risk factors such as diabetes, hypertension, and smoking in the black, Hispanic, and low-income patients. Additionally, while the specific code for atrial fibrillation was not used, cardiac arrhythmias were present in a much higher percentage of white and higher income patients in our study than in black, Hispanic, and lower income patients. Prior studies have demonstrated that black patients are less likely to receive IV rtPA as well,10 and this disparity has been thought to be from delays in hospital arrival (distance, transportation challenges) as well delays in symptom recognition in lower income and minority populations.23 There is additional literature that demonstrates that black patients receive inferior hospital care, including delays in receiving treatment in the emergency department and longer door-to-CT scan times.11,12 Other studies suggest that other contributors include caregiver racial biases, patient mistrust, educational and cultural barriers, and the relatively small number of minority physicians,24 as well as deeply rooted legacies of social and financial disenfranchisement.25 Socioeconomic and racial disparity has been long recognized in stroke care. Our current 11-year analysis re-emphasizes the presence of disparity in stroke care and demonstrates that despite the widespread nationwide spike in the use of EVT as a standard of care in patients with stroke with large-vessel occlusions, the wide socioeconomic and racial disparity in provision of this service remains grossly unchanged.
Additionally, our analysis demonstrates that patients with private insurance may be more likely to have a good outcome following EVT for AIS, while black patients may be less likely to have a good outcome and are more likely to have a poor outcome. Black and Hispanic patients had approximately double the percentage of tracheostomies as well as a higher percentage of gastrostomies compared with white patients. Prior studies have also demonstrated worse poststroke outcomes in minority patients;26⇓-28 however, there is a paucity of data regarding racial disparities in stroke outcomes following thrombectomy. Black patients in our population were slightly less likely to experience in-hospital mortality according to our multivariable analysis. This finding is consistent with similar findings from prior studies of the NIS.15 One possible reason offered in this observation is that black patients with stroke are, on average, younger than white patients. This was the case in our study because black patients were, on average, 8 years younger than white patients. The finding that black patients with AIS are younger than white patients additionally is validated in numerous studies that demonstrate that black patients have a higher stroke burden earlier in their lives than white patients and the general population.10 It is our hope that the data presented in this study will serve as further impetus to increase resources directed toward disparity research, with the hope of ultimately understanding the causes of these disparities and developing actionable interventions to achieve equity. Specifically, defining these disparities, in addition to awareness, is an important initial step in addressing and improving the current environment.
While the rate in EVT use appeared to be similar in women and men, female sex was predictive of poor outcome following EVT. This finding is consistent with findings in prior studies demonstrating worse outcomes in women with AIS following treatment with IV rtPA and EVT.29⇓-31 The reason for worse outcome after stroke in women compared with men is not fully understood; however, higher prestroke disability, a higher admission NIHSS score, and even smaller intracranial artery diameters have been previously postulated as possible causes for this discrepancy. 31,32
This study has many limitations. First, the NIS does not provide many important specifics about EVT that would be relevant to outcome such as the NIHSS score, ASPECTS, last known well, TICI score following thrombectomy, or baseline functional status. Additionally, the NIS does not provide information on whether the patient had a large-vessel occlusion, which would be relevant in the discussion of EVT use. Similarly, there is no information provided in the NIS on time metrics to EVT such as the time of symptom onset to recanalization, which may directly affect the clinical outcome. Also, as with all administrative datasets, the NIS may be prone to coding errors. Finally, the NIS does not offer any readmission data; therefore, we were unable to assess long-term outcome for these patients.
CONCLUSIONS
Our nationally representative study demonstrates that despite widespread increase in use of EVT in patients with stroke, notable socioeconomic and racial disparities still exist in access to this immensely effective and life-changing treatment technique. Further studies are warranted to address this ongoing shortcoming in providing stroke treatment.
Footnotes
Disclosures: Johanna T. Fifi—UNRELATED: Consultancy: Stryker, Penumbra, Cerenovus; Grants/Grants Pending: Stryker, Penumbra, Viz.ai; Stock/Stock Options: Imperative Care. Christopher P. Kellner—UNRELATED: Grants/Grants Pending: Cerebrotech, Minnetronix, Siemens, Penumbra, Viz.ai, Integra LifeSciences Corporation.* J. Mocco—UNRELATED: Consultancy: Cerebrotech, Viseon, EndoStream Medical, Vastrax, RIST Neurovascular, Synchron, Viz.ai, Perflow Medical, and CVAid; Stock/Stock Options: investor in Cerebrotech, Imperative Care, EndoStream Medical, Viseon, blinktbi, Myra Medical, Serenity, Vastrax, NTI, RIST, Viz.ai, Synchron, Radical, and Truvic Medical; Other: Principal Investigator on research trials funded by Stryker Neurovascular, MicroVention, and Penumbra. Shahram Majidi—UNRELATED: Employment: The Mount Sinai Hospital. *Money paid to the institution.
References
- Received March 25, 2021.
- Accepted after revision April 26, 2021.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Time to endovascular thrombectomy for acute ischaemic stroke in language other than English (LOTE) communities in South-Western Sydney
- Impact of Race, Gender, and Insurance Status on Outcomes Following Endovascular Treatment for Acute Ischemic Stroke
- Multicenter study of association between socioeconomic status and treatment of ruptured cerebral aneurysms compared to unruptured cerebral aneurysms: insights from 4,517 patients using the area deprivation index
- Racial disparities in access to, and outcomes of, acute ischaemic stroke treatments in the USA
- Neighbourhood deprivation, distance to nearest comprehensive stroke centre and access to endovascular thrombectomy for ischemic stroke: a population-based study
- Association of Neighborhood Deprivation With Thrombolysis and Thrombectomy for Acute Stroke in a Health System With Universal Access