
Article Figures & Data
Figures
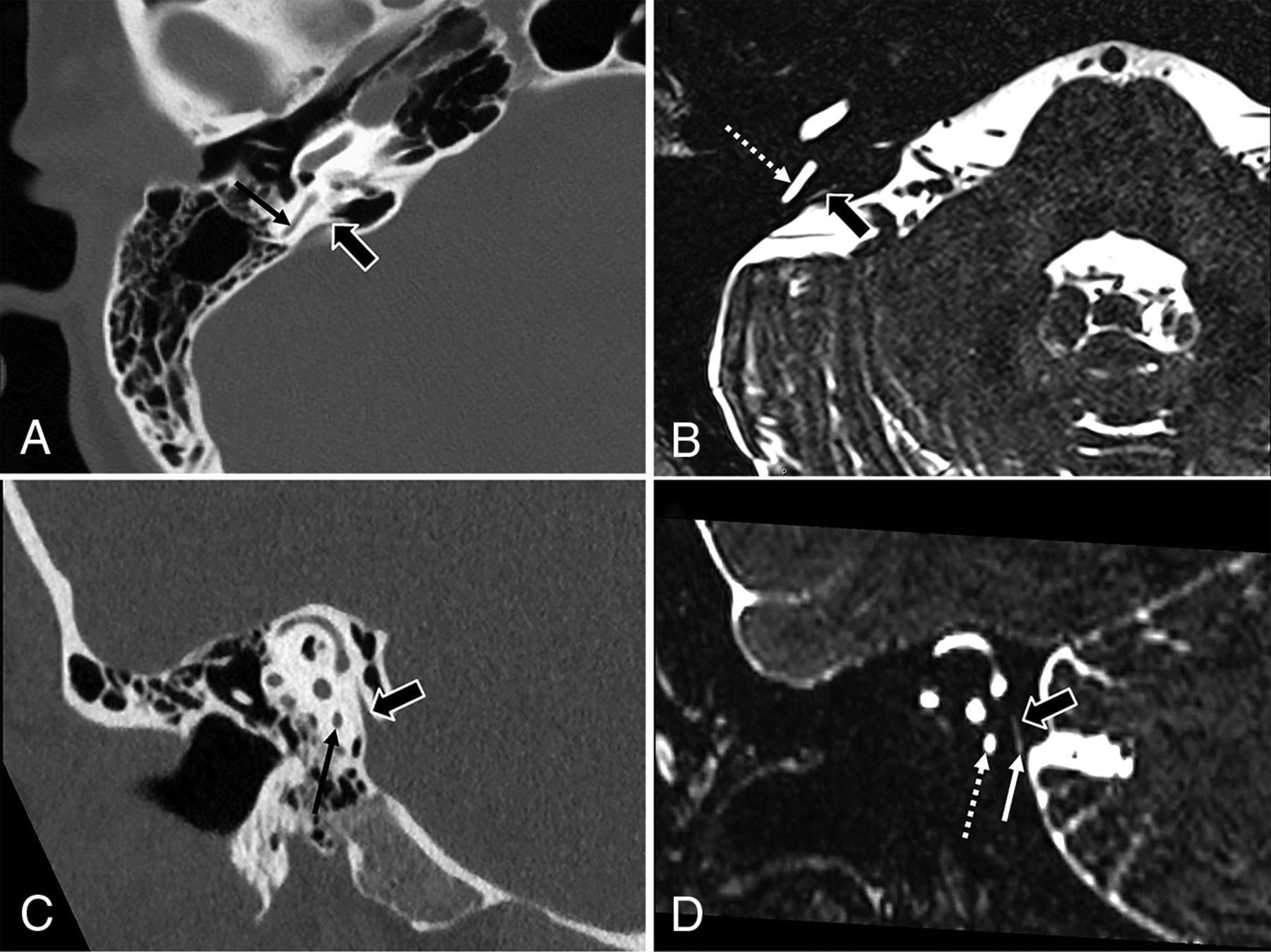
- FIG 1.
Anatomy of the endolymphatic duct and sac on axial (A and B) and Pöschl view (C and D) CT and 3D fast spin-echo T2-weighted MR images. The endolymphatic duct connects with the endolymphatic sac. Both structures are not directly seen on CT, but CT shows the osseous vestibular aqueduct that houses the endolymphatic duct (block arrows, A and C). Note the location of vestibular aqueduct extending to the cortex of the posterior temporal bone (block arrow, A). On MR imaging, the endolymphatic duct can be seen directly as a T2WI hyperintense tubular structure (block arrows, B and D), extending inferiorly beneath the dura of the posterior cranial fossa at the expected location of endolymphatic sac (white arrow, D). Note the close proximity of the posterior semicircular canal (black arrows on CT and dotted white arrow on MR imaging), an important anatomic landmark to identify the endolymphatic sac intraoperatively.
- FIG 2.
Endolymphatic sac decompression (A) versus mastoidectomy (B). A, Transmastoid endolymphatic sac shunt surgery: Postoperative changes of right canal wall-up mastoidectomy (asterisk). The posterior margins of the mastoidectomy defect extend up to the presigmoid osseous plate at the expected location of the endolymphatic sac (solid white arrow shows the location of transmastoid endolymphatic sac shunting). Removal of the bone overlying the posterior semicircular canal (black arrow) and vestibular aqueduct (dotted white arrow) indicates good surgical exposure of the endolymphatic sac. The silastic shunt is not directly visualized on CT. B, For comparison, an image from another patient with a simple canal wall-up mastoidectomy and ossiculoplasty for chronic otitis media. Note the mastoidectomy defect (asterisk) and the intact posterior cortex (solid white arrow) overlying the posterior semicircular canal (black arrow) and vestibular aqueduct (dotted white arrow).
- FIG 3.
Sacculotomy (A) versus stapes prosthesis migration (B). A, Sacculotomy with insertion of a Cody tack prosthesis. Oblique CT image reformatted along the long axis of the stapes (A) shows a linear metallic device in the saccule (dotted white arrow). This was a Cody tack device for a sacculotomy. Note the intact stapes (solid white arrow). B, Vestibular migration of stapes prosthesis. Oblique CT image reformatted along the long axis of the stapes (D) shows that the stapes suprastructure is replaced by a prosthesis (solid white arrow), with intrusion of the prosthesis into the vestibule.
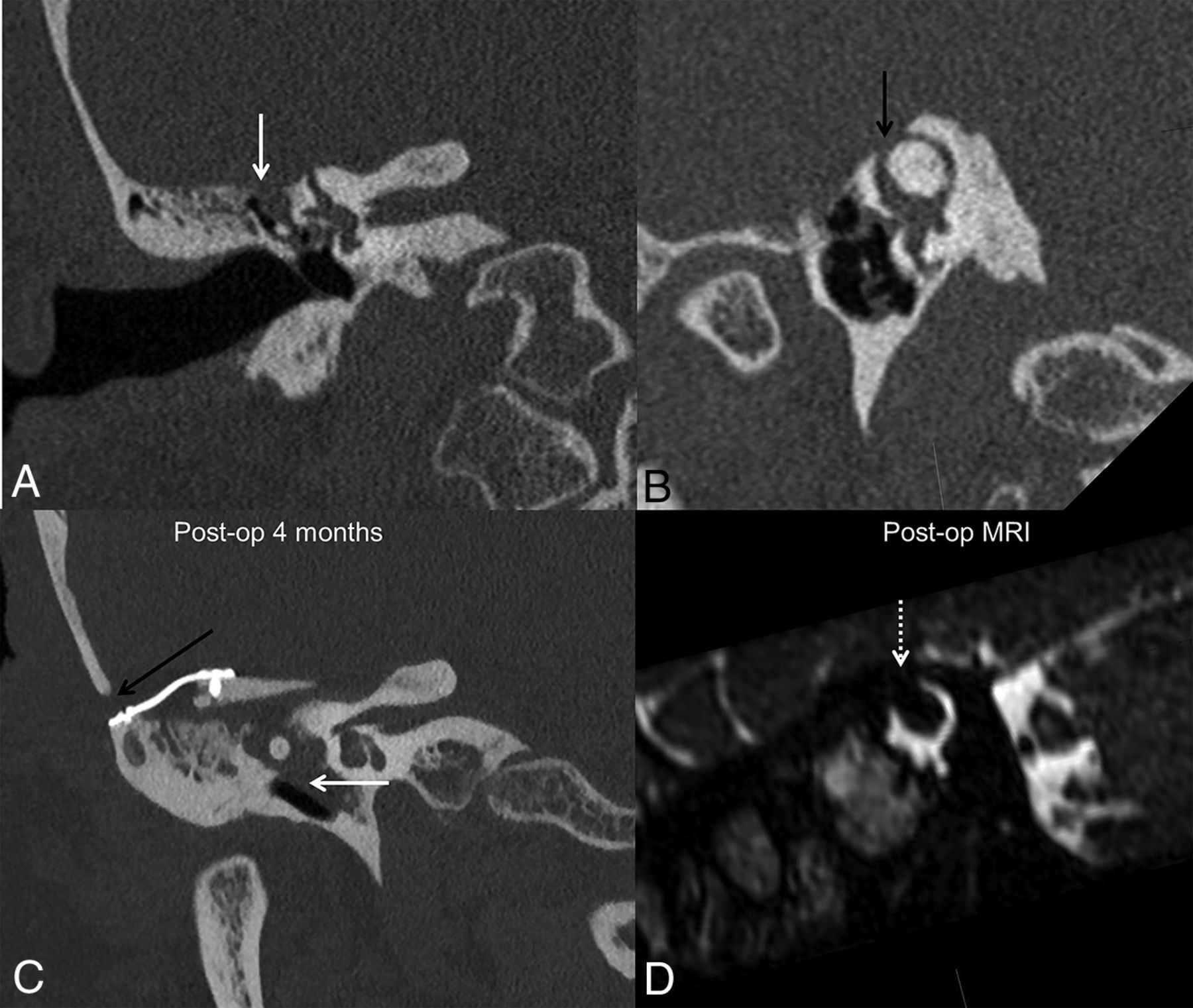
- FIG 4.
Surgical labyrinthectomy with cochlear labyrinthitis ossificans. Axial CT image (A) of the left temporal bone shows changes of prior transmastoid endolymphatic sac surgery (dotted white arrow), with a mastoidectomy defect extending posteriorly to the expected location of the endolymphatic sac. Postoperative changes of the subsequently performed hearing-ablative surgical labyrinthectomy are seen as surgical removal of bone overlying the lateral semicircular canal with a fistulous connection between the lateral semicircular canal and the mastoid defect (solid white arrow, A). Air also extends to the superior semicircular canal (solid white arrow, B). A more caudal image (C) shows mineralization within the basal turn of the cochlea (black arrow, C), consistent with labyrinthitis ossificans, an expected postoperative finding following labyrinthectomy.
- FIG 5.
Superior semicircular canal dehiscence repair through a middle cranial fossa approach (A and B) and transmastoid approach (C and D). Preoperative Pöschl view (A) shows dehiscence of the mid-third of the left superior semicircular canal (solid white arrow). A middle cranial fossa approach (dotted white arrow, B) was used to plug the superior semicircular canal with bone wax and temporalis fascia. Postoperative CT (B) shows further loss of bone overlying the superior semicircular canal due to drilling of bone overlying the superior semicircular canal to plug it (solid white arrow). Bone wax and temporalis fascia are radiolucent and not directly seen on CT. Postoperative changes of middle cranial fossa repair can be missed on temporal bone CT if not specifically sought and in the absence of clinical details. Preoperative CT (C) shows a large left superior semicircular canal dehiscence (solid white arrow). A transmastoid approach (dotted white arrows, D) was used to access the roof of the superior semicircular canal and plug it with bone wax and temporalis fascia. There is expected soft tissue in the mastoidectomy defect without evidence of otitis media (not shown). Pre-op indicates preoperative; Post-op, postoperative.
- FIG 6.
Transcanal occlusion of the round window for superior semicircular canal dehiscence. A patient with bilateral superior semicircular canal dehiscence underwent bilateral transcanal occlusion of the round windows with cartilage graft and fascia. Postoperative axial CT image of the right temporal bone (A) shows nodular soft tissue in the round window niche (white arrow). A normal round window niche is air-filled compared with that of a healthy patient (black arrow, B). Intraoperative image (C) shows a round window after occlusion with fascia/cartilage graft (white arrow), compared with that of a healthy patient (black arrow, D).
- FIG 7.
Postoperative changes of lateral semicircular canal fenestration performed for otosclerosis. Axial CT image shows lucency around the cochlea (the “double ring” sign) (dotted white arrow, A) consistent with retrofenestral otosclerosis. Postoperative axial (B) and coronal (C) CT images show an osseous defect over the lateral margin of lateral semicircular canal (solid white arrows) due to surgical fenestration of the lateral semicircular canal. This should not be mistaken for a lateral semicircular canal fistula. Note the associated mastoidectomy defect (asterisk).
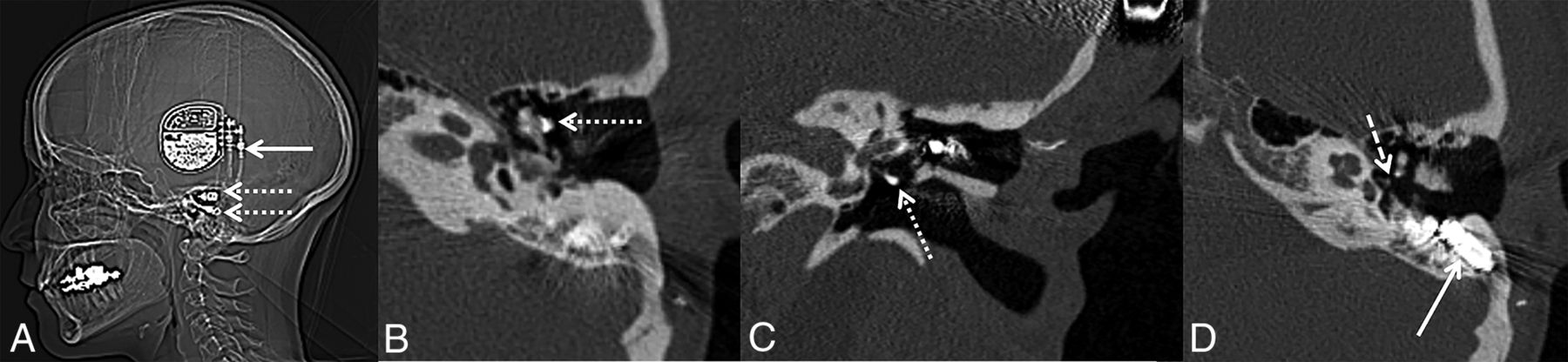
- FIG 8.
Temporal meningoencephalocele repair and superior semicircular canal dehiscence plugging complicated by CSF leak in a patient with idiopathic intracranial hypertension. Preoperative coronal CT of right temporal bone (A) shows a defect in the tegmen tympani. Soft tissue extends through the defect into the right middle ear (solid white arrow, A). Pöschl view (B) shows dehiscence of the mid-portion of the right superior semicircular canal (black arrow, B). Postoperative images show changes of right middle canal fossa repair with the bone and fascia graft held down with plate screws (black arrow, C). The right SSC was plugged with bone wax in the same setting, and the roof was resurfaced with fascia graft, better appreciated on the heavily T2-weighted MR imaging (D), which shows the expected focal loss of fluid signal in the right SSC at the site of plugging (dotted white arrow, D). Postoperatively, the patient developed a CSF leak requiring additional surgical repair (solid white arrow, C). The patient also had a small encephalocele on the left side (not shown) consistent with intracranial hypertension. Post-op indicates postoperative.
- FIG 9.
Internal auditory canal decompression for Camurati-Engelmann disease. Upper row: Preoperative CT images (A–C) in a patient with Camurati-Engelmann disease show extensive osseous skull base thickening and near-complete obliteration of both internal auditory canals (left > right) (solid white arrows, A). Coronal images (B and C) show marked narrowing of both internal auditory canals (dotted white arrows), more so medially where the porus acousticus is nearly obliterated due to hypertrophic osseous overgrowth of the walls of internal auditory canals (solid white arrows). Lower row: Postoperative CT images (D–F) show widely patent internal auditory canals bilaterally (solid white arrows, D). Coronal images (E and F) show decompression of the internal auditory canals by removal of the superior and anterior portions of the petrous bones (solid white arrows). The black polygon in C depicts the portion of the bone removed through the middle cranial fossa approach to decompress the internal auditory canal. Care is taken to preserve the arcuate eminence over the superior semicircular canal (black arrows, C and F).
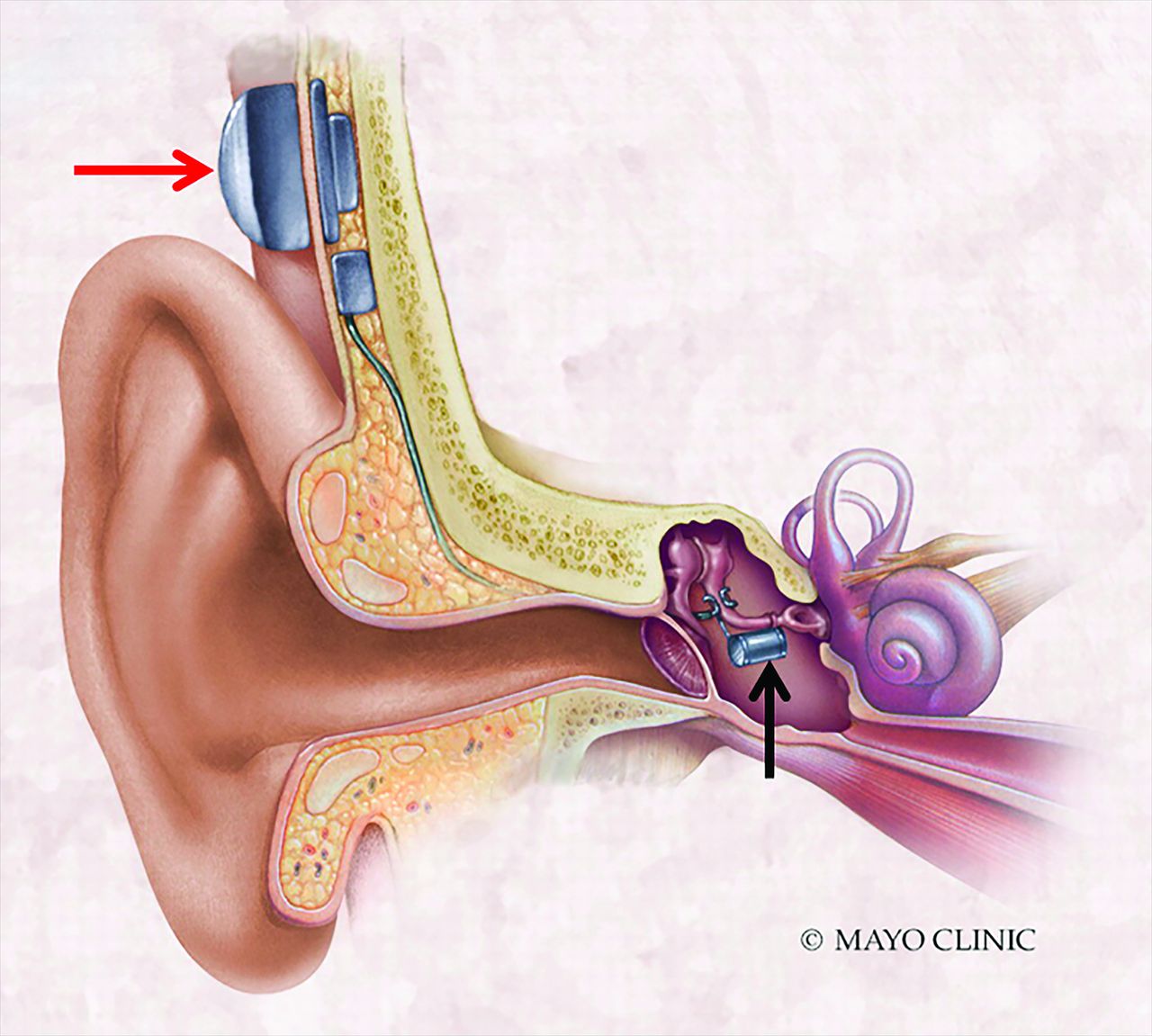
- FIG 10.
Normal active middle ear implant. Illustration of a partially implantable external audioprocessor (red arrow) attached to the mastoid bone that transmits vibrations to an internal floating mass transducer (black arrow) coupled with the intact ossicular chain. Images used with permission of the Mayo Foundation for Medical Education and Research. All rights reserved.
- FIG 11.
Dislodged floating mass transducer in a partially implantable active middle ear implant. Axial (A) and coronal (C) CT images show a dislodged floating mass transducer lying in the hypotympanum (dotted white arrows) instead of being attached to the stapes in the mesotympanum (solid white arrows, B, C). Postoperative photograph (D) shows the surgically retrieved floating mass transducer.
- FIG 12.
Expected CT findings in totally implantable AMEIs. Images show the different components of the totally implantable Esteem AMEI. The CT scout image shows the processor (solid white arrow) and separate internal sensor and driver leads (dotted white arrows). Axial (B and D) and coronal (C) CT images show the sensor on the incudomalleolar articulation (dotted white arrow, B), driver on the stapes (dotted white arrow, C), and audioprocessor in the mastoid (solid white arrow, D). The incudostapedial joint is disarticulated as part of the surgery (dashed white arrow, D) and should not be misdiagnosed as fracture/failure.
- FIG 13.
Jugular bulb dehiscence repair. Preoperative (A) and postoperative (B) axial CT images in a patient with pulsatile tinnitus show osseous dehiscence at the lateral margin of the high-riding right jugular bulb, with a diverticulum extending anteriorly to the tympanic annulus (solid black arrow, A). Intraoperatively, a bone pate was harvested from the mastoid cortex and used to cover the high-riding jugular bulb and jugular diverticulum. This is seen as hyperattenuating material at the tympanic annulus and external auditory canal on the postoperative CT (dotted black arrow, B).
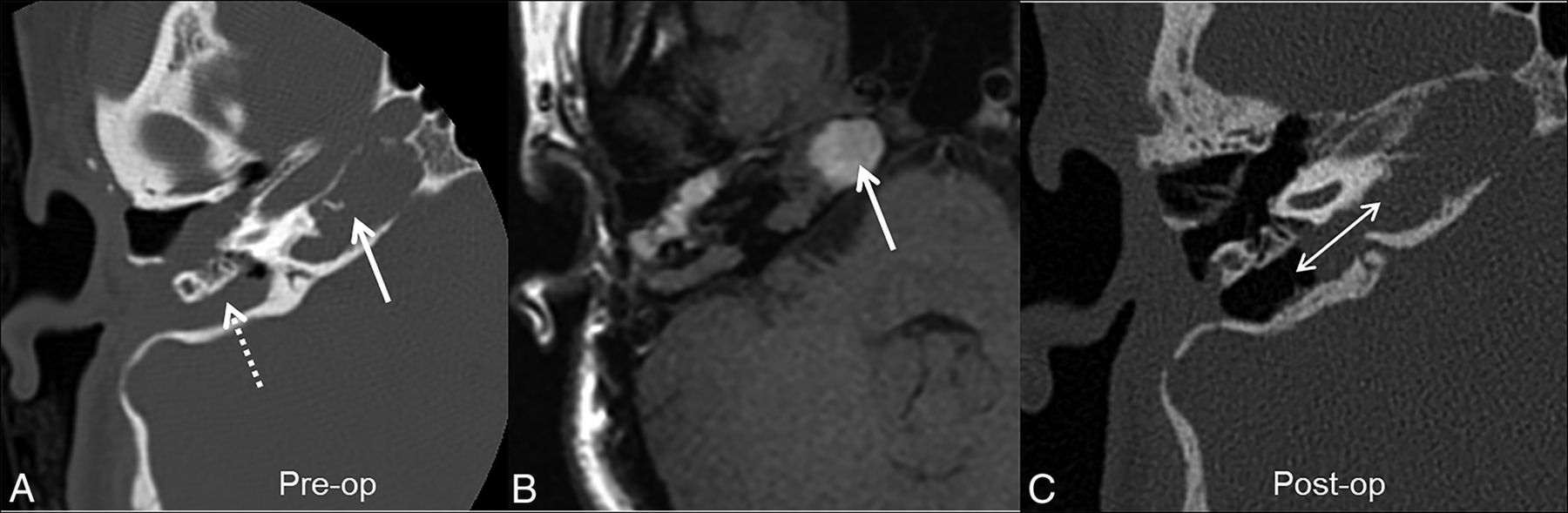
- FIG 14.
Petrous apex drainage surgery in a patient with recurrent right cholesterol granuloma. Predrainage CT image (A) shows a lesion expanding the petrous apex (solid white arrow) and extending to a prior postoperative mastoid defect (dotted white arrow). On T1-weighted MR imaging (B), the lesion is hyperintense (solid white arrow); it was also T2WI hyperintense and nonenhancing (not shown), consistent with a cholesterol granuloma. C, Postoperative CT image after drainage through a transmastoid infralabyrinthine approach shows the surgically created tract between the petrous and mastoid, allowing drainage of the petrous apex into the mastoid (double-headed white arrow). Pre-op indicates preoperative; Post-op, postoperative.














Tables
Surgical approaches for superior semicircular canal dehiscence repaira
Approaches Advantages Disadvantages Surgery Technique Approach Most Suitable for Middle Cranial Fossa Direct visualization of dehiscence More invasive requiring craniotomy and limited temporal lobe retraction All kinds of SSC repair: canal resurfacing, plugging, capping Transmastoid Less invasive, standard mastoidectomy approach No direct visualization of dehiscence Canal plugging and modified resurfacing (of SSC sidewalls and not directly over dehiscence) Transcanal Outpatient setting Less efficacious in long-term Reinforcement or occlusion of round window ↵a Modified with permission from Mau et al,16 Ward et al,17 and Succar et al.19





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.