
Abstract
BACKGROUND AND PURPOSE: Intracranial hemorrhage is a known complication following endovascular thrombectomy. The radiologic characteristics of a CT scan may assist with hemorrhage risk stratification. We assessed the radiologic predictors of intracranial hemorrhage following endovascular therapy using data from the INTERRSeCT (Identifying New Approaches to Optimize Thrombus Characterization for Predicting Early Recanalization and Reperfusion With IV Alteplase and Other Treatments Using Serial CT Angiography) study.
MATERIALS AND METHODS: Patients undergoing endovascular therapy underwent baseline imaging, postprocedural angiography, and 24-hour follow-up imaging. The primary outcome was any intracranial hemorrhage observed on follow-up imaging. The secondary outcome was symptomatic hemorrhage. We assessed the relationship between hemorrhage occurrence and baseline patient characteristics, clinical course, and imaging factors: baseline ASPECTS, thrombus location, residual flow grade, collateralization, and clot burden score. Multivariable logistic regression with backward selection was used to adjust for relevant covariates.
RESULTS: Of the 199 enrolled patients who met the inclusion criteria, 46 (23%) had an intracranial hemorrhage at 24 hours. On multivariable analysis, postprocedural hemorrhage was associated with pretreatment ASPECTS (OR, 1.56 per point lost; 95% CI, 1.12–2.15), clot burden score (OR, 1.19 per point lost; 95% CI, 1.03–1.38), and ICA thrombus location (OR, 3.10; 95% CI, 1.07–8.91). In post hoc analysis, clot burden scores of ≤3 (sensitivity, 41%; specificity, 82%; OR, 3.12; 95% CI, 1.36–7.15) and pretreatment ASPECTS ≤ 7 (sensitivity, 48%; specificity, 82%; OR, 3.17; 95% CI, 1.35–7.45) robustly predicted hemorrhage. Residual flow grade and collateralization were not associated with hemorrhage occurrence. Symptomatic hemorrhage was observed in 4 patients.
CONCLUSIONS: Radiologic factors, early ischemia on CT, and increased CTA clot burden are associated with an increased risk of intracranial hemorrhage in patients undergoing endovascular therapy.
ABBREVIATIONS:
- aOR
- adjusted OR
- CBS
- clot burden score
- EVT
- endovascular therapy
- ICH
- intracranial hemorrhage
With the results of the Clinical Mismatch in the Triage of Wake-up and Late Presenting Strokes Undergoing Neurointervention with Trevo (DAWN) and Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke 3 (DEFUSE-3) trials, the use of endovascular therapy (EVT) for large-vessel occlusion stroke will continue to increase as we transition from time-to tissue-based decision-making.1,2 While there is great potential to prevent disability and mortality, procedural risks still remain. Of note, post-EVT intracranial hemorrhage (ICH) continues to be observed consistently across studies.3 The incidence of intracranial hemorrhage varies from 9% to 25%.4 In recent randomized controlled trials, symptomatic hemorrhage was observed in 4%–8% of patients1,2,5; in nonrandomized studies, it was as high as 16%.4,6,7
Baseline imaging can help predict ICH following EVT.6,7 Low ASPECTS on presentation, low cerebral blood volume on perfusion, and thrombus length are associated with an increased risk of ICH following EVT.7⇓⇓–10 It remains to be seen whether emerging scores such as the clot burden score (CBS), residual flow grade, and collateral grade similarly predict post-EVT ICH because these scores may be more practical for clinicians in the acute setting.11 This knowledge may assist with pre-EVT prognostication and in the selection of borderline or “off-protocol”/higher risk individuals. The objective of our study was to investigate the predictors of ICH after EVT, with a focus on identifying imaging factors that may assist with risk stratification.
Materials and Methods
Local research ethics board approval was obtained at all enrolling sites as part of the Identifying New Approaches to Optimize Thrombus Characterization for Predicting Early Recanalization and Reperfusion with IV Alteplase and Other Treatments Using Serial CT Angiography (INTERRSeCT) study.12 Participants provided written consent. Data can be obtained from the senior author on reasonable request.
Patients
Patients were participants enrolled in the INTERRSeCT study.12 Briefly, INTERRSeCT was a prospective multicenter observational cohort study assessing recanalization rates with or without intravenous alteplase in patients with acute ischemic stroke. Patients enrolled in the study received treatment with intravenous tPA, EVT, both, or neither. Any patient presenting to the emergency department with symptoms consistent with ischemic stroke 12 hours from last known well and older than 40 years of age with a baseline CTA (before alteplase bolus if that drug was given) with evidence of a symptomatic intracranial thrombus was eligible. Patients with primary vertebrobasilar artery occlusions or a presenting ASPECTS of <6 were excluded from the study. Patients were also excluded if they had mRS > 2 at baseline, renal impairment (creatinine clearance level, <60 mL/min), contrast allergy, or hypoglycemia (serum glucose level, <2 mmol/L), or if they were unlikely to participate in follow-up. For this substudy, patients treated with IV tPA alone were excluded.
Imaging Evaluation and Treatment
Each patient was examined with noncontrast CT to exclude intracranial hemorrhage and to estimate signs of early ischemia via ASPECTS. Baseline CTA was used to identify acute occlusions in the anterior circulation and the following clot characteristics: thrombus location, CBS, residual flow grade, and collateralization grade. The CBS is a quantified assessment of the intracranial thrombus burden within the anterior circulation.13 Starting at 10, points are deducted on the basis of the loss of contrast opacification on CTA. Two points are deducted for contrast opacification within the supraclinoid ICA, proximal M1 MCA, or distal M1 MCA. One point is subtracted for opacification within the infraclinoid ICA, M2 branches of the MCA, or A1 segment of the anterior cerebral artery. A score of zero indicates occlusion of all major anterior circulation arteries. Residual flow was defined as the presence of attenuated contrast signal through the clot and was categorized as the following: Grade 0 is complete absence of contrast attenuation (no residual flow); grade 1, contrast attenuation denser than the surrounding brain parenchyma; and grade 2, a tiny lumen or streak of well-defined contrast is observed.14 Collaterals were graded as “good,” “intermediate,” or “poor” as per the Endovascular Treatment for Small Core and Proximal Occlusion Ischemic Stroke (ESCAPE) protocol.15 Clinical stroke severity was measured via the NIHSS at initial presentation, postprocedure, and at 24 hours. Follow-up at 24 hours was performed with MR imaging or CT. To maintain a pragmatic study design, participating sites were not required to use dual-energy CT. All imaging was sent to a core laboratory at the University of Calgary and reviewed by blinded study investigators.
Primary and Secondary Outcomes
The primary outcome of this study was any new intracranial hemorrhage diagnosed at 24-hour follow-up imaging. ICH was classified per the Heidelberg Bleeding system.16 Briefly, the Heidelberg system is based on the original European Cooperative Acute Stroke Study III definitions.17 To better reflect ICH in the context of intra-arterial therapy, hemorrhages are categorized into 5 major groups: 1a (hemorrhagic infarction [HI] 1), 1b (HI2), 1c (parenchymal hemorrhage [PH] 1), 2 (PH2), and 3 (other: remote ICH, intraventricular hemorrhage, subarachnoid, or subdural hemorrhage).18 Secondary outcome was symptomatic hemorrhage, defined as intracranial hemorrhage associated with an NIHSS ≥ 4 between the postprocedural assessment and 24-hour follow-up.
Statistical Analysis
Associations among patient characteristics (demographics, medical history, stroke severity, serum biomarkers), clinical course, imaging characteristics, and the occurrence of any intracranial hemorrhage were explored with the Fisher exact test, ANOVA, and Mann-Whitney U test, as appropriate. Factors with marginal significance (P < .1) were considered for inclusion in multivariable modeling. Continuous variables that did not meet the linearity assumption were categorized into quantiles, dichotomous variables or categoric variables. Collinearity was assessed using pair-wise correlations. Variables with a Spearman correlation of >0.25 were further assessed using 2-variable logistic regression models. Variables with confidence interval widening were assessed in separate multivariable models. Multivariable logistic regression with backward selection was performed to assess independent predictors of postprocedural intracranial hemorrhage. In post hoc analysis, radiologic score variables that were found to be statistically significant underwent further assessment via a receiver operating characteristic curve, and Youden's index was used to determine a clinically relevant threshold that predicts postprocedural hemorrhage. Statistical analysis was performed using SPSS, Version 25.0 (IBM, Armonk, New York) and SAS, Version 9.4 (SAS Institute, Cary, North Carolina).
Results
Of the 655 patients initially enrolled in the INTERRSeCT study, 199 were included in the primary analysis. Three hundred ninety-seven patients were not treated with mechanical thrombectomy. Forty-nine patients with vertebrobasilar occlusions, baseline modified Rankin Scale scores of > 2, and serum creatinine clearance levels of <60 mL/min were also excluded. Ten patients were excluded from analysis due to a presenting ASPECTS of 1–5, scores that would normally have excluded these patients from mechanical thrombectomy on the basis of selection criteria of the major treatment trials.2,15,19 The median age of the primary analysis population was 70 years (interquartile range, 59–78 years), and the median NIHSS score at initial presentation was 17 (interquartile range, 13–21). One hundred sixty of 199 (80%) patients received IV tPA along with mechanical thrombectomy. Forty-six patients (23%) had an ICH on 24-hour follow-up imaging. The breakdown of ICH subtypes is as follows: 1a (52.2%), 1b (17.4%), 1c (8.7%), 2 (19.6%), and 3 (2.2%). Only 4 of the 46 hemorrhage events were symptomatic (9%). Thirty patients with hemorrhage had a poor clinical outcome at 3 months (mRS 3–6). Patients with a postprocedural hemorrhage were associated with poor outcome (43% versus 12%, P < .001). The mean time to follow-up imaging was 24.4 ± 9.5 hours. There was no significant difference in mean follow-up time between patients positive for and negative for ICH (P = .86). MR imaging was used for follow-up imaging in 69 (35%) patients.
The associations between baseline patient characteristics and ICH occurrence are highlighted in Table 1. On univariate analysis, serum glucose and time to recanalization were higher in patients with ICH than in those without. Both ASPECTS and clot burden score were lower (indicating more early ischemia and increased clot burden, respectively) in patients with ICH. Occlusions located more proximally (eg, in the ICA) were associated with increased odds of post-EVT ICH. No significant relationship was observed among residual flow grade, collateralization, and hemorrhage incidence.
Exploratory analysis of patients stratified by hemorrhage occurrence at 24-hour follow-upa
Collinearity between CBS and clot location was suspected on the basis of significant pair-wise correlation (Spearman rank correlation, 0.87; P < .001) and confidence interval widening in 2-variable logistic models. The median CBSs for the ICA and proximal M1 locations were 1 and 6, respectively. The CBS for the remaining locations (distal M1, M2 horizontal, M2 Sylvian) ranged from 6 to 9. Clot location was included in an alternate multivariable regression model in which the clot burden score was not included (Table 2). No collinearity between CBS and time to recanalization was observed, and there was no relationship between CBS and a successful final recanalization state.
—Multivariable analysis—predictors of intracranial hemorrhage after endovascular therapy
If we adjusted for the relevant covariates, pretreatment ASPECTS (adjusted OR [aOR], 1.56 per point lost; 95% CI, 1.12–2.15) and clot burden score (aOR, 1.19 per point lost; 95% CI, 1.03–1.38) were associated with postprocedural hemorrhage. ICA occlusions were associated with a 3.10 times increased odds of postprocedure hemorrhage (95% CI, 1.07–8.91). Clinically, female sex (aOR, 2.34; 95% CI, 1.04–5.29), an elevated serum glucose level (aOR, 1.28 per 1 mmol/L increase; 95% CI, 1.09–1.51 mmol/L), and a prolonged time to recanalization (aOR, 1.33 per 60 minutes; 95% CI, 1.02–1.74 minutes) increased the risk of hemorrhage.
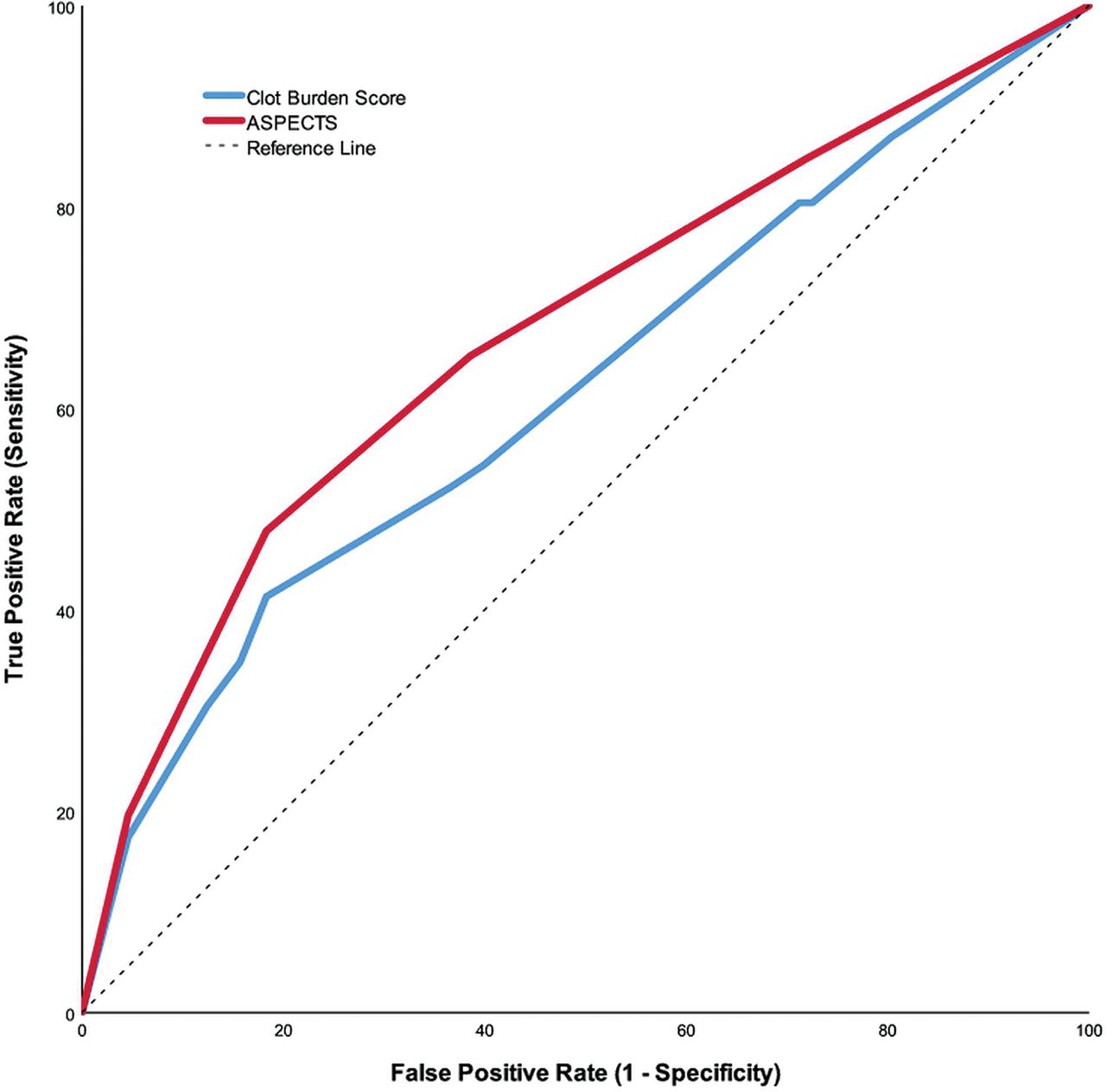
Baseline ASPECTS and CBS were selected for post hoc analysis. The receiver operating characteristic curves comparing these 2 radiologic scores with hemorrhage occurrence are shown in the Figure. According to Youden's index, the mathematically optimal cut-point for ASPECTS was ≤7 (sensitivity, 48%; specificity, 82%). Adjusted for relevant covariates, ASPECTS ≤7 was associated with a 3.17 times increased odds of ICH (95% CI, 1.35–7.45). Likewise, the ideal optimal cut-point for CBS was ≤3 (sensitivity, 41%; specificity, 82%; OR, 3.12; 95% CI, 1.36–7.15), indicative of extensive clot burden.

Receiver operating characteristic curves. Curves for baseline ASPECTS (area under the curve, 0.68; 95% confidence interval: 0.58–0.77) and CBS (area under the curve, 0.62; 95% confidence interval: 0.52–0.72).
Discussion
Our study assessed whether imaging features of large-vessel occlusion could help identify patients who are at high risk of post-EVT ICH. In a prospective cohort representative of the real-world application of EVT, we found that lower pretreatment ASPECTS, ICA clot location, and increased clot burden independently predicted ICH. Our study suggests that imaging features may be helpful for prognostication and risk stratification for EVT.
The findings of pretreatment ASPECTS affecting the risk of hemorrhage are in keeping with previous studies and provide further evidence that patients presenting with increasing amounts of early ischemia are at risk of developing postprocedural hemorrhage.7,20,21 States of relative hyperglycemia have been previously associated with postprocedural hemorrhage, and our findings are in line with previous work in this area.22,23 Prolonged symptom-to-recanalization times have also been previously associated with postprocedural hemorrhage and may aid in bedside prognostication.7 We hypothesize that a prolonged time to recanalization allows more time for the development of ischemia, ultimately increasing the risk of hemorrhage formation. Technical factors that could be associated with an increased time to recanalization, such as an increased number of stent-retriever passes, may play a contributing role as well.7,24
The CBS is a surrogate representation of both thrombus length and location.11 Accordingly, CBS was colinear with thrombus location. This idea is supported by the low clot burden scores observed in the ICA and proximal M1 locations and the increased risk of ICH associated with the ICA thrombus location in our alternate multivariable model. Our findings suggest that proximal occlusions in the ICA will often exhibit a high clot burden, thereby increasing the risk of hemorrhage in this particular patient subgroup. This finding, however, does not mean that clot burden equates to a difficult recanalization because we found no relationship among clot burden, time to recanalization, or successful recanalization.
Our findings complement safety data recently published from the Highly Effective Reperfusion evaluated in Multiple Endovascular Stroke Trials (HERMES) collaboration, a pooled patient-level analysis of the 7 major randomized controlled EVT trials.21 In this analysis, clot burden score, pooled into 3 groups (8–10, 5–7, 0–4), was not associated with symptomatic ICH. The symptomatic ICH event rate in INTERRSeCT was relatively low, and we therefore cannot comment on the associations between CBS and symptomatic ICH. However, asymptomatic hemorrhages are associated with poor outcome,25 and postprocedural ICH occurrence is still an important contributor to clinical outcome, symptomatic or not. While the risk of hemorrhage increases with certain locations and extensive clot burden (CBS ≤ 3), it is exactly these same patients who stand to benefit the most from EVT. Thus, our findings are important prognostic elements that can be discussed with patients and their families, even if they do not specifically influence the decision to offer EVT.
We expected to see an increased risk of hemorrhage in patients undergoing combined therapy; this was not observed. If IV tPA does not increase the risk of ICH, the size of the brain injury may ultimately have the largest influence on hemorrhagic transformation risk7,8,10; this notion is further supported by our results. Furthermore, our study supports the safety of combined therapy and provides additional context for the ongoing debate around whether EVT alone should be offered instead of combined therapy.26
Our study has several limitations. It can be difficult to differentiate contrast staining from reperfusion hemorrhage. Contrast staining is seen in approximately one-third of patients, and unlike reperfusion hemorrhage, it does not have a negative prognosis.27 For those 69 (35%) patients who underwent follow-up MR imaging, this concern is less because MR imaging can effectively differentiate blood from contrast staining.28 However, for the remaining scans, CT was the primary imaging technique of choice. Ideally, dual-energy CT would be used to effectively distinguish contrast from blood,29 but study sites were not required to do this. While the reported washout period of IV contrast is estimated to take place within 24–48 hours,29,30 studies seeking to differentiate contrast from hemorrhage have, in fact, used imaging at the 24-hour mark as a comparative end point.30 In addition, a recent study by Dekeyzer et al31 reported that follow-up CT scans performed at least 19 hours after the initial CT can differentiate contrast and hemorrhage with high specificity. The mean time to follow-up in our study was 24.4 ± 9.5 hours. Thus, while the risk of mistaking hemorrhage for contrast remains, we believe that we have reduced the risk of potential bias by strictly following our protocol timeline for follow-up imaging. Additional limitations include the use of an observational design, which may have introduced selection bias toward those patients offered EVT. Finally, given that EVT was not yet considered standard of care, technical data on the endovascular therapy procedure (number of passes, device used, aspiration used) were not collected.
Conclusions
Imaging characteristics, namely pretreatment ASPECTS, clot burden score, and clot location, are predictive of post-EVT ICH. These radiologic factors can be acquired with relative ease during an acute stroke and therefore can be practical tools to assist with EVT prognostication and can complement risk/benefit conversations with patients and their caregivers.
Footnotes
Disclosures: Robert Mikulik—RELATED: Grant: Project No. LQ1605 from the National Program of Sustainability II and the project of the International Clinical Research Center of St. Anne's University Hospital in Brno No. CZ.1.05/1.1.00/02.0123 (Operační program Výzkum a vývoj pro inovace).* Thalia S. Field—RELATED: Grant: Canadian Institutes of Health Research operating funds, Comments: The research program of the Vancouver Stroke Program received a per-patient payment to offset the cost of research nurse time and non-standard-of-care neuroimaging for the INTERRSeCT study*; UNRELATED: Consultancy: Bayer Canada, Pfizer-Bristol-Myers Squibb, Servier Laboratories, Comments: Advisory Board honoraria; Grants/Grants Pending: Canadian Institutes of Health Research, Heart and Stroke Foundation of Canada, Canadian Stroke Consortium, Bayer Canada, Boehringer-Ingelheim, Comments: Canadian Institutes of Health Research, Heart and Stroke Foundation of Canada, Canadian Stroke Consortium operating funds, Boehringer Canada operating funds, and Bayer Canada in-kind study medication*; Payment for Lectures Including Service on Speakers Bureaus: Bayer Canada, Pfizer-Bristol-Myers Squibb, Servier Laboratories, Boehringer-Ingelheim, Comments: Speakers Bureau honoraria from Bayer Canada, Pfizer-Bristol-Myers Squibb, Servier Laboratories, and Boehringer-Ingelheim Canada. Jean-Martin Boulanger—UNRELATED: Consultancy: Novartis, Bayer, Pfizer, Comments: conferences and Advisory Boards. Michael D. Hill—RELATED: Grant: Canadian Institutes of Health Research, Comments: grant to the University of Calgary. The principal Investigator was Dr A.M. Demchuk. I was a coinvestigator on the grant*; UNRELATED: Board Membership: Canadian Neuroscience Federation, Comments: not-for-profit entity; Consultancy: Boehringer-Ingelheim; Grants/Grants Pending: Medtronic, Stryker, Bayer Canada, Boehringer-Ingelheim, NoNO Inc, Canadian Institutes of Health Research, Alberta Innovates, British Heart Foundation, Comments: grants for ongoing studies; Stock/Stock Options: Calgary Scientific Inc, Comments: stock ownership. Andrew M. Demchuk—RELATED: Consulting Fee or Honorarium: Medtronic. Bijoy K. Menon—RELATED: Grant: Canadian Institutes of Health Research, Comments: operating grant.* Dar Dowlatshahi—UNRELATED: Consultancy: ApoPharma, Bayer; Payment for Lectures Including Service on Speakers Bureaus: Bristol-Myers Squibb. *Money paid to the institution.
INTERRSeCT was originally funded by an operating grant from the Canadian Institutes of Health Research. Dr Dowlatshahi was funded by a University of Ottawa Department of Medicine Clinician-Scientist Research Chair award and a Heart and Stroke Foundation of Canada New Investigator Award. Dr Yogendrakumar is supported by the Queen Elizabeth II Graduate Scholarship for Science and Technology and the Canadian Institutes of Health Research Banting and Best Graduate Scholarship. Dr Mikulik was supported by No. LQ1605 from the National Program of Sustainability II (MEYS CR) and by The International Clinical Research Center of St. Anne's University Hospital in Brno No. CZ.1.05/1.1.00/02.0123 (Operační program Výzkum a vývoj pro inovace).
Indicates open access to non-subscribers at www.ajnr.org
REFERENCES
- Received November 23, 2018.
- Accepted after revision February 11, 2019.
- © 2019 by American Journal of Neuroradiology





{kind=link}