
Abstract
BACKGROUND AND PURPOSE: It is well-established that a high prevalence of infants with congenital heart defects surviving to childhood have neurodevelopmental abnormalities. The etiology is not clear. In this study, we aimed to find prenatal neuroanatomic changes in fetuses with congenital heart disease to better understand the pathophysiology behind these sequelae.
MATERIALS AND METHODS: A retrospective study of 46 fetal brain MR imaging scans was performed at a tertiary medical center during a 4-year period. Clinical data were collected from electronic medical charts. Volumes of the supratentorial brain, right hemisphere, left hemisphere, and cerebellum were measured using a semiautomated method and were compared with the normal growth percentiles.
RESULTS: We found that cerebellar volume and the cerebellar-supratentorial volume ratio were significantly lower among fetuses with congenital heart disease. Supratentorial and hemisphere volumes showed no difference between groups. This difference was not observed in fetuses with septation defects.
CONCLUSIONS: Fetuses with congenital heart disease have smaller cerebellar volumes than healthy fetuses. Additional research is needed to assess this finding as a radiologic marker for long-term outcome.
ABBREVIATIONS:
- CHD
- congenital heart disease
- CV
- cerebellar volume
- HLHS
- hypoplastic left heart syndrome
- LHV
- left hemisphere volume
- ICC
- intraclass correlation coefficient
- RHV
- right hemisphere volume
- STV
- supratentorial brain volume
- TGA
- transposition of the great arteries
Congenital heart diseases (CHDs), which affect approximately 0.9% of all births, are abnormalities of the heart present at birth. Once a life-threatening condition, today most CHDs are corrected or palliated in infancy, enabling these children to reach adulthood. However, a considerable proportion of the surviving children show neurodevelopmental abnormalities.1
Studies were made to further understand these sequelae and found that neonates with CHD have a high prevalence of anatomic and functional neurologic abnormalities.2⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–19 The etiology of the abnormalities is unknown, and it is presumed to be multifactorial, both from a shared genetic background and as a secondary outcome. One of the leading hypotheses is damaged oxygen supply to the brain,3,5,6,15,18,20 either because of reduced cerebral oxygen saturation or from the disturbed circulation, both derived from the heart defect.
To investigate this hypothesis, a few biometric studies have been performed. Miller et al7 used preoperative MR imaging to evaluate and compare several parameters indicative of cerebral maturation and oxidative stress between fetuses with and without hypoplastic left heart syndrome (HLHS) and transposition of the great arteries (TGA). They found significant changes in both CHD groups compared with controls. Also supporting the hypoxemia hypothesis, Mahle et al4 used MR imaging to show that neonates with a variety of CHDs had ischemic lesions in the form of periventricular leukomalacia and infarcts as well as elevated lactate levels before surgery. Kaltman et al6 examined the cerebrovascular blood flow in fetuses with right- and left-sided obstructive congenital heart diseases using a Doppler echocardiogram. They showed differences in middle cerebral and umbilical artery resistance in fetuses with CHD compared with normal values. These changes may result from a primary unknown etiology or can represent a functioning autoregulatory mechanism of the brain vasculature reacting to hypoxia.
Our objective was to compare volumetric measurements of different structures in the fetal brain between healthy fetuses and those with CHD using a new 3D MR imaging method. We hypothesized that brain volume would be smaller in the CHD group compared with healthy controls.
Materials and Methods
Subjects
The subjects of this retrospective study were women who underwent MR imaging scans in the third trimester of pregnancy for fetal evaluation after a suspected CHD. Scans were obtained between 2011 and 2014 at the tertiary Chaim Sheba medical center. Performing MR imaging is now the routine practice in fetuses with suspected CHD, used for structural and biometric 2D examination of the brain. An estimated diagnosis of CHD was made during pregnancy and was made final after postnatal tests.
The measurements were compared with percentile tables derived from healthy fetuses in a previous study.21 Measurements and calculation methods in the current and the aforementioned study are identical and are described below.
MR Imaging
This study was based on the routine fetal MR imaging procedure performed in our institution. Fetal brain MR imaging was performed using a 1.5T system (Optima scanner; GE Healthcare, Milwaukee, Wisconsin). Single-shot fast spin-echo T2-weighted sequences in 3 orthogonal planes were obtained using a half-Fourier technique (NEX = 0.53) with the following parameters: section thickness = 3 or 4 mm, no gap, flexible coil (8-channel cardiac coil). FOV was determined by the size of the fetal head, with a range of 24 × 24 cm to 30 × 30 cm, acquisition time = 40–45 seconds, matrix = 320/224, TE = 90 ms, TR = 1298 ms, pixel bandwidth = 122 Hz/pixel. Specific absorption rate values were between 1.1 and 1.7 W/kg.22
Measurements
All measurements were obtained in the coronal plane. For each fetus, we measured 6 structures: the supratentorial brain, right and left cerebral hemispheres, right and left lateral ventricles, and cerebellum. Of the volumes measured, 5 structures were assessed in the study: supratentorial brain volume (STV), right hemisphere volume (RHV), left hemisphere volume (LHV), cerebellar volume (CV), and the ratio between the cerebellar volume and the supratentorial volume (CV/STV). Measurements were used as follows:
Supratentorial Brain.
For measurement of the supratentorial brain volume, we included the parenchyma of the frontal, parietal, occipital, and temporal lobes (including the third ventricle) and excluded the lateral ventricles (measured separately and subtracted), brain stem, cerebellum, and fourth ventricle. Anterior, posterior, superior, and lateral boundaries were defined as the outer edge of the cerebral cortex. The inferior border matched the cortex and an imaginary line crossing the brain stem between the edges of the tentorium cerebelli.
Hemispheres.
The left and right hemisphere volumes were measured separately using the same lateral boundaries with the longitudinal fissure as a medial boundary.
Cerebellum.
Cerebellar hemispheres were drawn with the cerebellar peduncles and vermis. Brain stem and the fourth ventricle were excluded.
Delineation was made by a semiautomated algorithm implemented using Matlab computing environment (MathWorks, Natick, Massachusetts). In this method, the first step includes tracing the ROI manually in the brain parenchyma of the midcoronal slice through cursor-guided freehand traces. On the basis of the intensity of the pixels included in the initial contour, the contour is then automatically propagated by a level-set-based active contour algorithm until convergence into a new, more accurate contour. The next step is forward and backward propagation, starting at the midcoronal slice, achieving contours automatically for every slice. Each new contour is based on the previous one; with a prefixed downsized volume for every slice. When it is completed, the user can manually adjust the resulted contour to achieve maximal accuracy (Fig 1). The volume is computed as the total number of voxels enclosed by the contours multiplied by the size of the voxel.21

A, The initial contour drawn manually on the midcoronal slice. B, Converged contour automatically propagated by a level-set-based active contour algorithm. C, The contour after manual adjustment.
The reliability of the semiautomated method was assessed. Interobserver variability was tested comparing measurements of 15 fetuses made by 2 independent observers. Intraobserver variability was checked by 1 observer who measured a sample of 15 fetuses twice. The intraclass correlation coefficient (ICC) was calculated. Medium agreement is defined as 0.4 < ICC < 0.6; good agreement, as 0.6 < ICC < 0.8; and very good agreement, as ICC > 0.8.14
Statistics
Our main purpose was to see whether our sample was different from the normal population. The sample size of 46 was estimated to give a power of 80%, with α = .05, to assess an average difference of 0.6% between our study groups.
Fetal brain volumes (STV, RHV, LHV, CV, CV/STV) from the CHD group were assigned to percentiles according to the normal fetal brain volume distribution; then, using a t test, the mean was compared with a population with a mean of 50. For each structure that was measured, fetuses were also classified into 4 categories according to their percentiles: <15%, 15%–50%, 50%–85%, and >85%. They were then compared with expected values from normal distributions using the χ2 test. Statistical analysis was performed using SPSS Statistics for Windows, Version 23.0 (IBM, Armonk, New York).
To see whether there was a difference among different types of congenital heart defects, we subdivided the group of CHDs into 3 subgroups according to a division by Bruneau in 2008.23 Thirty-six of 46 fetuses fell into 1 of 3 subcategories: cyanotic heart disease (n = 19), left-sided obstruction defects (n = 9), and septation defects (n = 8). The groups' means were compared to each other and to the normal population using a t test.
We also addressed the effect of brain pathology on the volume measurements. As described in the “Results” section, some fetuses were diagnosed with various brain pathologies according to the official MR imaging report. To understand whether there is a difference in the measured volumes between fetuses with and without brain pathology, we subdivided the CHD group into 2 subgroups according to the official MR imaging report: group A for fetuses with a diagnosed brain pathology (n = 11) and group B for fetuses without one (n = 35). For each structure measured, we then performed a comparison between the percentile distributions of the 2 groups using a t test for equal variances. A result of no difference between the groups would mean that brain pathology has no impact on the volume measurements.
Results
Clinical Characteristics of the Study Population
Fifty-six fetuses with CHD were identified; 10 cases were excluded due to lack of sufficient information. Demographic details on the CHD group are shown in Table 1. Of the whole CHD group, 2 pregnancies were terminated due to parental decisions. Nuchal translucency was obtained in 39 of 46 pregnancies (85%) and had abnormal findings in 3 (8%). Thirty-three of 46 (72%) had undergone amniocentesis; one had abnormal findings (3%). One of 46 fetuses (2%) was diagnosed with intrauterine growth restriction on fetal ultrasound. Diagnosis of heart defects was determined according to postnatal imaging for 44 of 46 fetuses and according to the prenatal echocardiography for the 2 pregnancies that were terminated. Diagnoses are shown in Table 2. More than half of the fetuses had >1 defect.
Demographic characteristics of the CHD group
CHD typesa
Variability Assessment Results
Estimations are shown in Table 3. Volumetric estimations show between good and very good interobserver and intraobserver reliability.
Interobserver reliability of measurements expressed as ICCs
Official MR Imaging Report
In 10 of 46 fetuses (22%), brain fetal MR imaging demonstrated variable findings. The brain pathologies are shown in Table 4.
Fetal brain pathology according to the official MRI report
Volumetric MR Imaging Measurements and Analysis
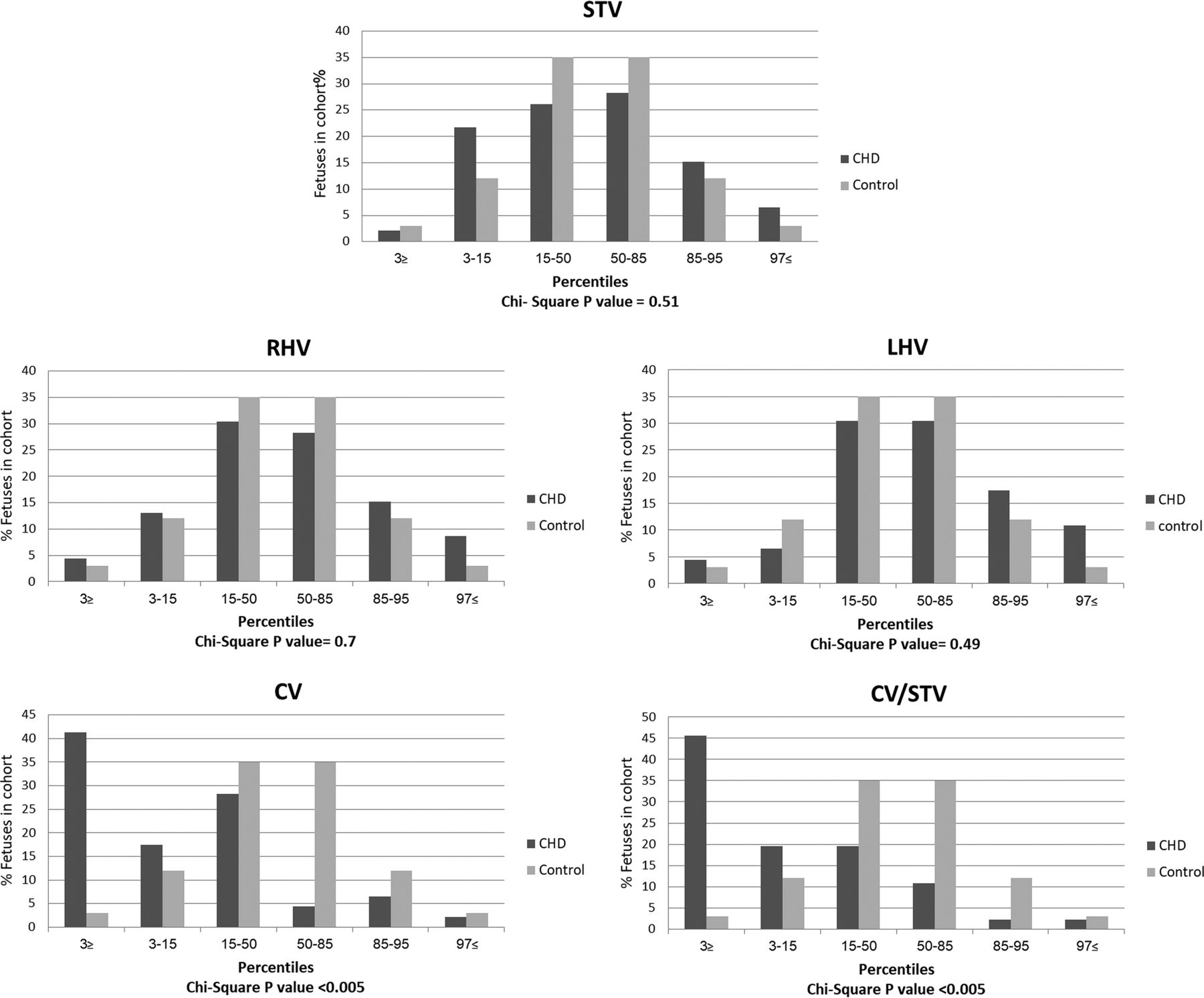
Analysis of the comparison among different brain structures using a t test is shown in Table 5. For each brain structure measured, subjects were divided according to their percentiles in relation to the normal distribution. One fetus had STV below the third percentile, 2 had RHV below the third percentile, 2 had LHV below the third percentile, 19 (41%) had CV below the third percentile, and in 21 (46%) fetuses, the CV/STV ratio was below the third percentile. Distributions are shown in Fig 2, and χ2 P values are given for each structure. Results show that the cerebellar volume is significantly lower in the CHD group compared with healthy fetuses (P < .005, Table 5), as well as the ratio between the cerebellum and the supratentorial brain (P < .005). We did not find any differences in other structures measured.
Comparison between the CHD and reference groups using a t test analysis

Brain volumes of the CHD group distributed by percentiles derived from the reference group: STV, RHV/LHV, and CV.
When analyzing the different types of defects, we found a significantly smaller cerebellar volume in the cyanotic heart disease group compared with healthy fetuses and the same for the group of left-sided heart obstruction defects. However, we did not find any difference between the septation defects group and healthy fetuses. This group had defects such as atrial septal defect and ventricular septal defect.
Analysis of the effect of brain pathology on volume measurements was also made. For each structure, we compared the percentile distribution between groups A and B and found no difference between the groups. We infer that the existence of a brain pathology diagnosis has no impact on those measurements.
Discussion
In our study, we attempted to investigate brain volume disturbances in fetuses with CHD. While our results do not show lower volumes of the RHV, LHV, and STV among fetuses with CHD, we did find a significant decrease in CV and in CV/STV compared with healthy fetuses. When analyzing the CHD type, we found that this difference did not exist in septal defects.
Our study adds evidence to increasing reports on brain growth and volume disturbances in fetuses with CHD. Limperopoulos et al11 used 3D MR imaging and MR spectroscopy to compare brain volumes and metabolism between healthy fetuses and those with CHD. They found progressively smaller total brain volumes in the CHD group compared with controls. Masoller et al17 also studied brain volumes in fetuses with CHD and found a reduction in brain volume compared with fetuses without CHD. Our results are not comparable with theirs because we measured different structures; we divided the total brain volume into supratentorial and infratentorial structures. This division enabled us to reveal that in fact, the cerebellum was the major contributor to the significant decrease in volume.
This finding is congruent with the findings of a recent study by Wong et al,19 who used MR imaging to measure the cerebellum of fetuses with CHD in 3 planes. They found a significant decrease in the sagittal vermis height in the CHD group versus controls. Vermian hypoplasia was also reported by Brossard-Racine et al24 as one of the possible findings in MR imaging of fetuses with CHD. Zeng et al16 used ultrasound to evaluate volumes of different structures in the brains of fetuses with CHD. They found a reduction in all brain volumes in fetuses with CHD, yet in their study, the reduction was larger in the frontal lobes than in the cerebellum. Ortinau et al13 also evaluated different brain structure volumes using 2D measurements in 3 cross-sections. They found that fetuses with CHD had smaller frontal, parietal, cerebellar, and brain stem measurements than healthy controls. In accord with Zeng et al, they also found that the frontal lobes showed the greatest alteration in growth.
Fetal cerebellar volumes were studied in different diseases. A volumetric MR imaging study on fetuses with intrauterine growth restriction demonstrated a reduction in cerebellar volume compared with other brain structures.22 A cerebellar growth restriction was also demonstrated in preterm fetuses.25 Most interesting, both of these conditions are associated with hypoxemia.26,27 Studies in sheep showed that a prolonged period of placental insufficiency, resulting in fetal hypoxemia, can affect the growth of the cerebellum, with a reduction in cell number and size.28,29 The cerebellum is considered particularly vulnerable to the negative effects of an insult due to its rapid growth during gestation.30 Cerebellar injury is associated with a broad spectrum of functional neurodevelopmental sequelae, including cognitive, language, behavioral, and social deficits as well as the well-known motor effect attributed to cerebellar injuries.31 Children with CHD exhibit a range of disabilities in these areas1; hence, cerebellar injury is a relatively less recognized but possibly important cause of neurodevelopmental delay in children with CHD.
Another aspect of the contribution of our study is that so far, results on brain volume reduction mainly focused on HLHS and TGA.2,6,8⇓–10,20 In our study, we demonstrated these effects in various types of CHD because our cohort comprised only 4 cases of HLHS (∼9%) and 9 cases of TGA (∼20%). Masoller et al18 addressed this question and compared the fetal neurodevelopment between 2 groups of fetuses with CHD divided according to the expected blood supply to the brain, with group A containing only HLHS, TGA, critical aortic stenosis, and hypoplastic aortic arch. They found that both groups had significant abnormal neurodevelopment (including brain volumes) compared with healthy control fetuses, but a linear tendency across the 3 subgroups was observed, with CHD group A fetuses showing more pronounced differences.18 When we tried to find differences among the types of CHD, we found that only defects considered mild such as atrial septal defect and ventricular septal defect do not affect the volume, while all the others do.
The presence of preoperative brain abnormalities in fetuses with CHD is well-established, showing disturbances in metabolism, blood flow, growth, and maturation. There is growing evidence that hypoxia is a major mechanism. This theory is based on the hypothesis that circulatory disturbances, especially occurring in HLHS and TGA, disrupt the oxygen supply to the brain and thus impact its growth and maturation. In healthy neonates, blood is oxygenated in the lungs and flows to the body through the left ventricle and aorta. In certain defects, this circulation is disturbed. For example, in HLHS, blood does not flow to the body through the left ventricle because it is hypoplastic, and in TGA, the left ventricle is connected to the lungs. In both defects, the neonate is dependent on the fetal shunts (foramen ovale, ductus arteriosus, or a ventricular septal defect) and pumps blood to the body using the right ventricle. Under those conditions, tissue oxygen supply is compromised, first due to inefficient circulatory architecture, and secondly due to systemic delivery of deoxygenated blood.
We acknowledge some limitations of this study. First, normal curves were derived from healthy fetuses undergoing MRI for suspected fetal abnormalities, allowing for a possible selection bias in the reference group. Lack of women with healthy pregnancies for reference is a common limitation in this research field.32,33 Another limitation is a lack of postnatal follow-up to assess whether findings are associated with neurodevelopmental outcomes.
Conclusions
We found that fetuses with CHD have smaller CV and CV/STV than healthy fetuses. Although further research is needed to assess the extent of damage among the different CHD types and to investigate the association with neurodevelopmental sequelae, this finding can provide deeper insight into the pathophysiology of the neurodevelopmental sequelae of children with CHD and influence important decision-making.
REFERENCES
- Received December 23, 2017.
- Accepted after revision February 14, 2018.
- © 2018 by American Journal of Neuroradiology





{kind=link}
{kind=link}