
Article Figures & Data
Figures
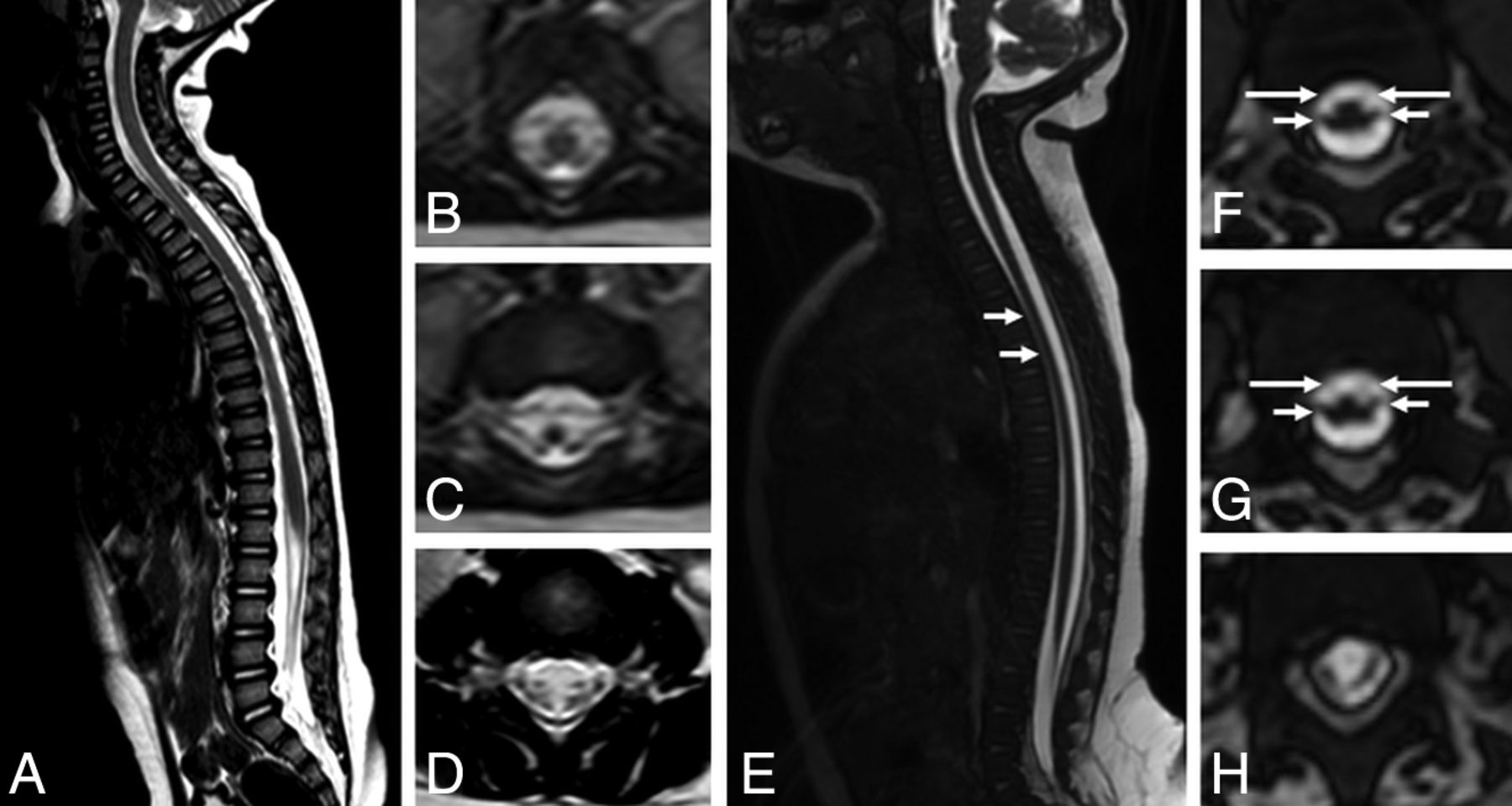
- Fig 1.
Comparison of spinal cord MR imaging between a control 12-month-old child (A–D) and a 4-month-old infant with presumed congenital Zika syndrome and arthrogryposis (E–H). Sagittal T2 (A) shows a normal-sized spinal cord and conus medullaris and no abnormal signal. Axial reformatted T2 reveals symmetric and normal-sized anterior and posterior nerve roots in the conus medullaris (B and C) and cauda equina (D). Meanwhile, sagittal T2-weighted volumetric GRE image (E) shows reduced spinal cord thickness, especially in the thoracic region (short white arrows). On the axial reconstruction of T2-weighted volumetric GRE (F–H), we can observe reduction of the conus medullaris anterior roots (long arrows) compared with posterior roots (short arrows).
- Fig 2.
An infant with congenital Zika syndrome and arthrogryposis (A and B), with flexion contracture of the superior limbs, mainly of the wrists, hyperextension contracture of the lower limbs, and right hip deformity. Spinal cord MR imaging of an infant with arthrogryposis, showing spinal cord measurements (C–E). Sagittal T2-weighted fast imaging using steady-state acquisition (volumetric GRE) shows the cervical (C, from superior to inferior, vertebral canal diameter, largest cervical cord diameter, and smallest cervical cord diameter), lumbar (D, from superior to inferior, vertebral canal diameter, largest lumbar cord diameter, and smallest lumbar cord diameter), and thoracic (E, from superior to inferior, vertebral canal diameter and smallest thoracic cord diameter) segments. There is apparently reduced spinal cord thickness, especially in the thoracic region (E), and an enlarged cisterna magna (C).
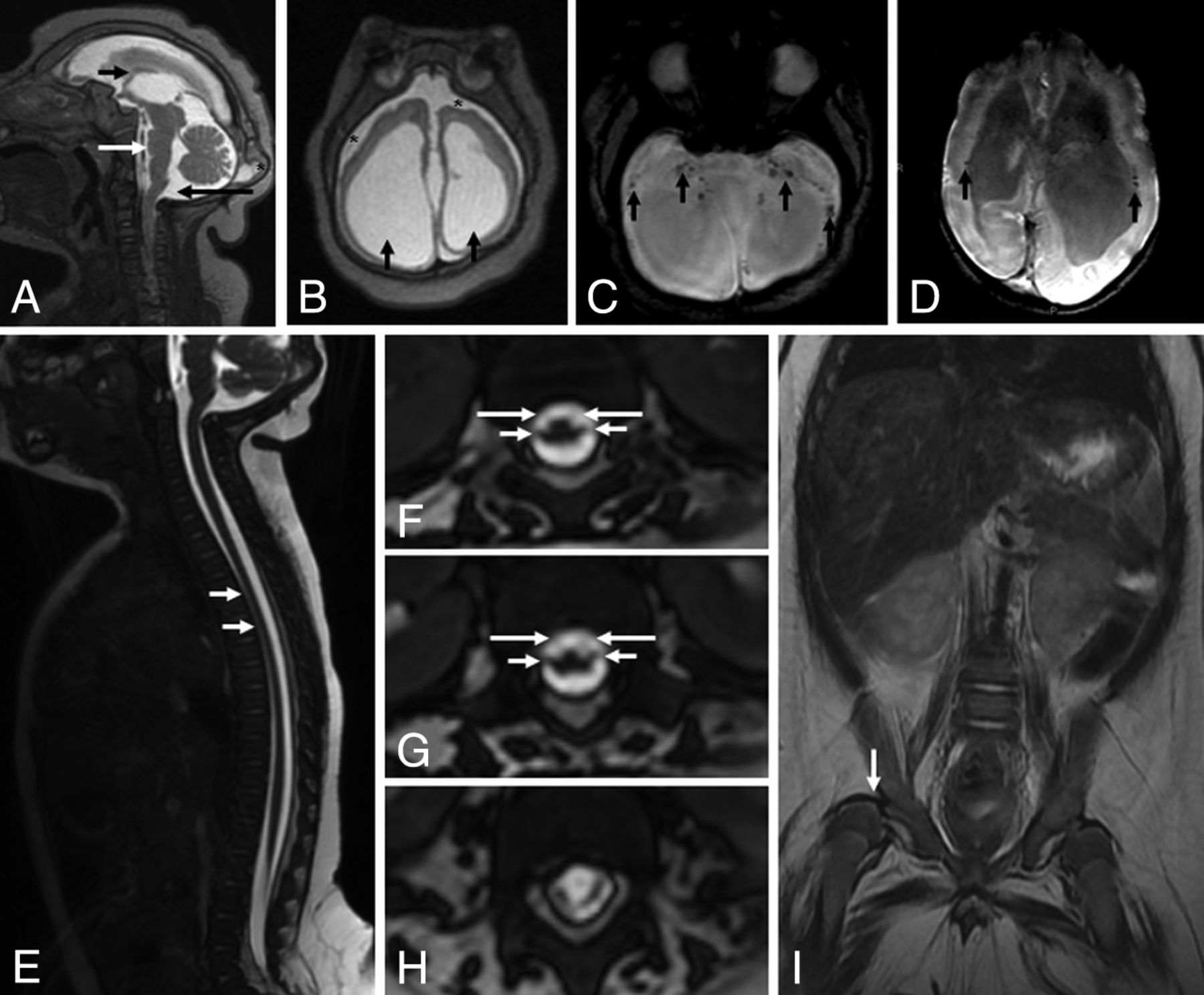
- Fig 3.
MR imaging of the brain and the spinal cord of an infant with microcephaly probably caused by congenital Zika virus infection, who has arthrogryposis. Sagittal T2-weighted image (A) shows craniofacial disproportion, a hypogenetic corpus callosum (short black arrow), pons hypoplasia (white arrow), and a slightly enlarged cisterna magna (long black arrow). Note the lush external occipital protuberance (star). Axial T2-weighted image (B) shows an extremely simplified gyral pattern, a thin cortex with minimal sulcation, enlargement of the subarachnoid space (stars), and severe ventriculomegaly, mainly at the posterior horn (black arrows). Note small dystrophic calcifications, mainly at the basal ganglia and thalamus and in the junction between the cortical and subcortical white matter, and periventricular calcifications (black arrows) on T2-weighted SWI (C and D). Sagittal T2-weighted volumetric GRE (E) shows reduced spinal cord thickness, especially in the thoracic region (white arrows). On the axial reconstruction of T2-weighted volumetric GRE (F–H), we can observe reduction of the conus medullaris anterior roots (long arrows) compared with the posterior roots (short arrows), suggesting increased damage in the anterior-versus-posterior horns of the spinal cord. Coronal T2-weighted imaging (I) reveals congenital hip dysplasia, especially on the right side (white arrow).
- Fig 4.
MR imaging of the brain and the spinal cord of an infant with microcephaly probably caused by congenital Zika virus infection who has arthrogryposis. Sagittal T1-weighted image (A) shows severe microcephaly, brain stem (short black arrow) and severe cerebellar (long black arrow) hypoplasia, and an enlarged posterior fossa with a very enlarged cisterna magna communicating with the fourth ventricle (long white arrow). Note the extremely hypogenetic corpus callosum (small white arrow). Axial T2-weighted images (B and C) show severe ventriculomegaly and enlargement of temporal horns (stars) and other parts of the lateral ventricles, mainly at the posterior horn and ventricular atrium (short black arrows). Note the bulging walls of the ventricle and a simplified gyral pattern with minimal sulcation and slight enlargement of the subarachnoid space (long black arrows). Also, note small dystrophic calcifications mainly seen at the basal ganglia and thalamus (black arrows) on T2-weighted SWI (D). Sagittal T2-weighted volumetric GRE (E) shows thin spinal cord thickness, and axial reconstruction of T2-weighted volumetric GRE reveals a prominent anterior median fissure of the spinal cord (F) and symmetric reduction of the conus medullaris anterior roots (long arrows) compared with posterior roots (short arrows), with damage affecting the anterior cord, preferentially (G and H).
- Fig 5.
MR imaging of the brain and the spinal cord of an infant with microcephaly confirmed to be caused by the Zika virus without arthrogryposis. Sagittal T2-weighted images (A) shows hypogenesis of the corpus callosum (white arrow) and an enlarged cisterna magna (black arrow). Coronal T2-weighted image (B) shows left cerebellar hemisphere hypoplasia, with cortical malformation and microcysts (white arrows). Axial SWI (C) shows small dystrophic calcifications in the junction between the cortical and subcortical white matter and in the basal ganglia (black arrows). Axial T2-weighted image (D) shows a simplified gyral pattern, bilateral cortical thickness in the pachygyric frontal lobe (white arrows), and ventriculomegaly (black arrows). The spinal cord and conus medullaris are normal-sized and show no abnormal signal on the sagittal T2-weighted volumetric GRE (E). Axial reformatted T2-weighted volumetric GRE reveals normal-sized anterior and posterior nerve roots in the conus medullaris (F and G) and cauda equina (H).





Tables
- Table 1:
MR imaging parameters for brain and spinal cord image acquisition for all of the participants
MRI Parameters Brain Spinal Cord Axial 3D SWAN Axial 3D FSPGR Axial T2*GRE Sagittal 3D Volumetric GRE Coronal T2 Axial T2 TE (ms) 50 Minimum 645 Minimum 120 110 TR (ms) 78.3 – 25 – 3700 5934 Flip angle 15° 12° 15° 45° – – Bandwidth (kHz) 41.67 31.25 31.25 50 41 31.25 FOV (cm) 20 20 24 30 25 18 Section thickness (mm) 3 2 5 0.8 4.5 4 Spacing (mm) – – 0.5 – 0.5 1 Frequency (Hz) 288 256 288 320 384 320 Phase 224 256 192 320 224 224 NEX – 1 1 1 1 3 Frequency direction AP AP AP AP R-L AP Note:—AP indicates anteroposterior; R-L, right-left; FSPGR, fast-spoiled gradient recalled; SWAN, susceptibility-weighted angiography.
- Table 2:
Individual clinical data of the 12 infants, 8 without and 4 with arthrogryposis, included in the study
No. Sex Gestational Age (wk) HC at Birth (cm) Mother's Rash during Pregnancy Joints Affected IgM ZIKV CSF Statusa Congenital Zika syndrome without arthrogryposis 1 F 35 29.5 2 mo Positive 2 M 36 31.5 4 mo No data 3 F 40 30 No rash No data 4 M 39 26 3 mo Positive 5 M 39 31 3 mo Positive 6 F 39 28.5 2.5 mo Positive 7 M 39 wk 5 days 32 4 mo Positive 8 M 39 wk 5 days 28 3 mo Positive Congenital Zika syndrome with arthrogryposis 9 F 37 29 No rash Feet, knees, hips, elbows, wrists, fingers Positive 10 M 37 26 4 mo Feet, knees, hips, wrists, fingers No data 11 M 40 27 No rash Feet, knees, hips No data 12 F 38 30 2 mo Feet, hips, wrists, fingers Positive Note:—HC indicates head circumference; ZIKV, Zika virus.
↵a Test performed on the infant.
- Table 3:
Comparison between groups with and without arthrogryposis of features identified on MRI by visual inspectiona
Ag (n = 4) No Ag (n = 8) Pb Sites with spinal cord reduction Absent 0 (0.0%) 2 (25.0%) .002c Thoracic 0 (0.0%) 5 (62.5%) Cervical, thoracic 0 (0.0%) 1 (12.5%) Cervical, thoracic, conus medullaris 4 (100.0%) 0 (0.0%) Site of most severe spinal cord reduction Absent 0 (0.0%) 2 (25.0%) <.999 Thoracic 4 (100.0%) 6 (75.0%) Prominence of the anterior median fissure of the spinal cord Absent 2 (50.0%) 8 (100.0%) .091 Present 2 (50.0%) 0 (0.0%) Reduction of the anterior nerve roots of the conus medullaris No reduction 0 (0.0%) 2 (25.0%) .007c Mild 0 (0.0%) 4 (50.0%) Moderate 0 (0.0%) 2 (25.0%) Severe 4 (100.0%) 0 (0.0%) Congenital hip dysplasia Absent 0 (0.0%) 2 (25.0%) .515 Present 4 (100.0%) 6 (75.0%) - Table 4:
Comparison between groups with and without arthrogryposis regarding the anteroposterior diameter at different levels of the spinal cord and as the ratio between the spinal cord and vertebral canal anteroposterior diametersa
AP Diameters (mm) Spinal Cord Measures Spinal Cord/Vertebral Canal Ratio Ag (n = 4) No Ag (n = 8) Pb Ag (n = 4) No Ag (n = 8) Pb Smallest spinal cord diameters Cervical 4.5 (4.4–4.9) 5.4 (4.7–5.9) .073 0.44 (0.41–0.47) 0.57 (0.44–0.60) .154 High thoracic 3.6 (2.8–4.2) 3.9 (3.6–4.5) .214 0.39 (0.29–0.41) 0.39 (0.34–0.46) .570 Conus medullaris base 4.3 (3.5–4.8) 6.3 (5.7–6.5) .008c 0.44 (0.41–0.47) 0.57 (0.44–0.60) .016c Largest spinal cord diameters Cervical intumescence 4.7 (4.5–5.0) 5.6 (5.4–6.2) .048c 0.46 (0.41–0.49) 0.58 (0.47–0.63) .109 Lumbar intumescence 5.0 (3.9–5.8) 7.3 (7.1–7.5) .008c 0.44 (0.32–0.51) 0.59 (0.56–0.64) .008c - Table 5:
Comparison between children with and without arthrogryposis regarding some of the brain abnormalities found on MRIa
Variables Arthrogryposis Pb No (n = 8) Yes (n = 4) Decreased brain volume 6 (75.0%) 4 (100.0%) .515 Grade of brain volume decrease Mild 1 (20.0%) 0 (0.0%) .876 Moderate/severe 4 (80.0%) 3 (100.0%) Degree of cerebral damage .394 Absent 1 (12.5%) 0 (0.0%) Mild 2 (25.0%) 0 (0.0%) Moderate 2 (25.0%) 0 (0.0%) Severe 3 (37.5%) 4 (100.0%) Symmetry 6 (75.0%) 3 (75.0%) >.999 Cortical development abnormalities Pachygyria 3 (37.5%) 3 (75.0%) .545 Polymicrogyria 2 (25.0%) 0 (0.0%) .515 Simplified gyral pattern 4 (50.0%) 3 (75.0%) .576 Corpus callosum >.999 Normal 2 (25.0%) 0 (0.0%) Hypogenesis 5 (62.5%) 3 (75.0%) Hypoplasia 1 (12.5%) 1 (25.0%) Cortical and subcortical junction calcifications 7 (85.5%) 4 (100.0%) >.999 Basal ganglia calcifications 3 (37.5%) 3 (75.0%) .545 Periventricular calcifications 0 (0.0%) 3 (75.0%) .018c Brain stem calcifications 1 (12.5%) 3 (75.0%) .067 Cerebellum calcifications 0 (0.0%) 2 (50.0%) .091 Cerebellum or brain stem hypoplasia 2 (25.0%) 4 (100.0%) .061 Increased cisterna magna 8 (100.0%) 4 (100.0%) – Delayed myelination 5 (50.0%) 4 (100.0%) .208





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}