
Abstract
BACKGROUND AND PURPOSE: Ultrasound has become widely accepted as the first imaging technique used for the assessment of cervical lymph node metastasis in patients with papillary thyroid cancer. In this systematic review and meta-analysis, we evaluate the performance of CT for the preoperative diagnosis of cervical lymph node metastasis in patients with papillary thyroid cancer compared with ultrasound.
MATERIALS AND METHODS: Ovid-MEDLINE and EMBASE data bases were searched for studies regarding the use of CT to diagnose cervical lymph node metastasis. The diagnostic performance of CT, ultrasound, and combined CT/ultrasound was assessed by using level-by-level and patient-based analyses. We also performed meta-analyses on the basis of the central and lateral neck levels.
RESULTS: Nine eligible studies, including a total sample size of 1691 patients, were included. CT showed a summary sensitivity of 62% (95% CI, 52%–70%) and specificity of 87% (95% CI, 80%–92%) for diagnosing cervical lymph node metastasis when using level-by-level analysis. There was a positive correlation between the sensitivity and the false-positive rate (correlation coefficient, 0.807) because of the threshold effect. The summary sensitivity of combined CT/ultrasound (69%; 95% CI, 61%–77%) was significantly higher than ultrasound (51%; 95% CI, 42%–60%), though the summary specificity did not differ.
CONCLUSIONS: The diagnostic performances of CT and ultrasound are similar, though CT and ultrasound combined are superior to ultrasound only. CT may be used as a complementary diagnostic method in addition to ultrasound for diagnosing cervical lymph node metastasis in patients with papillary thyroid cancer.
ABBREVIATIONS:
- HSROC
- hierarchic summary receiver operating characteristic
- QUADAS-2
- Quality Assessment of Diagnostic Accuracy Studies-2
- US
- ultrasound
Papillary thyroid cancer involves metastasis to cervical lymph nodes in up to 60%–70% of patients.1,2 The presence of cervical lymph node metastasis is also highly associated with local recurrence and cancer-specific mortality.3,4 Several studies have demonstrated that cervical lymph node metastasis had an unfavorable prognostic effect on survival in patients 45 years of age and older.5,6 According to the new American Thyroid Association guidelines,7 ultrasound (US) has become widely accepted as the first imaging technique used for the assessment of cervical lymph node metastasis in patients with papillary thyroid cancer. A recent meta-analysis demonstrated that the sensitivity of US was 63% (95% CI, 47%–76%), the specificity was 93% (95% CI, 73%–99%), and the area under the curve was 0.81 (95% CI, 0.77–0.84) by level-by-level analysis.8
However, because US is an operator-dependent technique, it is often difficult to evaluate the entire neck. Several US studies have reported variable and relatively low sensitivity for the assessment of central cervical lymph node metastasis.9⇓–11 Normal anatomic structures, including the larynx, trachea, and areas deep in the clavicles, jaw, and sternum, cause significant acoustic shadowing.12 This results in limited US evaluation of the mediastinum and retropharyngeal area, regardless of clinical experience of the operator.
Contrast-enhanced CT is a standard imaging technique used for the assessment of cervical lymph node metastasis in head and neck cancer; however, CT was not recommended as a routine imaging technique for patients with papillary thyroid cancer.13 Nevertheless, several recent studies have reported the possibility of the complementary role of CT for the preoperative evaluation of cervical lymph node metastasis.14⇓⇓⇓⇓⇓⇓⇓–22 According to the new American Thyroid Association guidelines,7 CT is currently recommended as an adjunct to US for patients with clinical suspicion of advanced disease, such as invasive primary tumor or clinically apparent, multiple, or bulky lymph node metastasis. Because the US examination is operator-dependent and it is difficult to evaluate deep anatomic structures, CT with contrast enhancement may be useful in delineating the extent of tumor involvement in the airway or esophagus as well as delineating extranodal tumor extension. Preoperative knowledge of these features of the primary tumor or metastases could significantly influence the surgical plan.7,23 Therefore, it is timely and necessary to collect currently available data regarding the diagnostic performance of CT in the preoperative diagnosis of cervical lymph node metastasis.
A meta-analysis is part of the systematic review and uses statistical methods to integrate the results of multiple original studies.24 Recently, the use of systematic review with meta-analyses is increasing in the field of radiology academic research (ie, diagnostic test accuracy). The main objectives of systematic review with meta-analyses are to obtain more valid, generalizable summary estimates and to identify and provide information on covariates that affect diagnostic accuracy tests.25⇓–27 To the best of our knowledge, no systematic review with meta-analyses has assessed the role of using CT to diagnose cervical lymph node metastasis in patients with papillary thyroid cancer. Therefore, this systematic review with a meta-analysis evaluates the diagnostic performance of CT in the preoperative diagnosis of cervical lymph node metastasis in patients with papillary thyroid cancer compared with US.
Materials and Methods
Literature Search Strategy
A computerized search of the MEDLINE and EMBASE data bases was performed to find relevant, original literature reports on the use of CT to diagnose cervical lymph node metastasis in patients with papillary thyroid cancer. We used the following search terms: (“thyroid cancer” OR “thyroid cancers” OR “thyroid carcinoma” OR “thyroid carcinomas”) AND (cervical lymph node metastasis OR cervical metastatic lymph node OR cervical metastatic lymphadenopathy) AND (ultrasonography OR sonography OR US OR “CT” OR CT). The beginning search date was not limited. Our search was limited to human patients and English language studies. We continued updating the literature search until November 29, 2015. To expand the search, we perused the bibliographies of the articles to identify other appropriate articles.
Inclusion Criteria
Studies that investigated the performance of CT in the preoperative diagnosis of cervical lymph node metastasis in patients with papillary thyroid cancer were eligible for inclusion. We included studies that satisfied all of the following criteria:
Population.
Studies included >10 patients who underwent CT for papillary thyroid cancer before surgery. None of these patients had undergone previous operations of the head and neck.
Reference Standard.
The level of cervical lymph nodes was determined according to the American Joint Committee on Cancer Cancer Staging Manual.28 Assignment of cervical lymph nodes was based on compartments, including the lateral compartment (levels I–V) and the central compartment (level VI). The CT criteria for cervical lymph node metastasis were as follows: strong enhancement without hilar vessel enhancement, heterogeneous enhancement, calcification, and cystic or necrotic change.29 The US criteria for cervical lymph node metastasis were as follows: focal or diffuse hyperechogenicity, micro- or macrocalcification, cystic change; an abnormal vascular pattern (a chaotic or peripheral vascular pattern), and a round shape (long-transverse diameter ratio, <1.5).30⇓–32 The final diagnoses of lymph nodes at each level were determined on the basis of the pathology reports regarding surgical specimens.
Study Design.
Observational studies (retrospective or prospective) were included.
Outcomes.
Results were reported in sufficient detail to evaluate the diagnostic performance of CT.
Exclusion Criteria
The exclusion criteria were the following: 1) case reports and series with a sample size of <10 patients and studies with a potential selection bias (eg, nonconsecutive series); 2) review articles, editorials, letters, comments, and conference proceedings; 3) studies on topics other than using CT to diagnose cervical lymph node metastasis in patients with papillary thyroid cancer; 4) studies with insufficient data to construct a 2 × 2 table; and 5) studies with overlapping patients and data. Two reviewers (C.H.S. and J.H.B.) independently selected the studies from the literature.
Data Extraction
We extracted the following data from the selected literature studies onto standardized data forms: 1) study characteristics: authors, year of publication, hospital or medical school, duration of patient recruitment, study design, and sample size; 2) demographic and clinical characteristics of the patients: mean age, analysis methods, and criteria of CT and US for diagnosing cervical lymph node metastasis; and 3) the diagnostic performance of CT and US. One reviewer (C.H.S.) extracted data from the studies, and the second reviewer (J.H.B.) double-checked the accuracy of the extracted data.
Quality Assessment
The methodologic quality of the included studies was independently assessed by 2 reviewers (C.H.S. and J.H.B.) by using tailored questionnaires and criteria provided by Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2).33
Data Synthesis and Analyses
The diagnostic performances of CT and US were assessed as the main indices for this meta-analysis. First, a meta-analysis for all of the included studies was performed by using level-by-level and patient-based analyses. Second, we performed meta-analyses on the basis of the central and lateral neck levels.
Heterogeneity among the studies was determined by using the Higgins I2 statistics (0%–40%, might not be significant; 30%–60%, may represent moderate heterogeneity; 50%–90%, may represent substantial heterogeneity; and 75%–100%, may represent considerable heterogeneity).34 When heterogeneity was noted, heterogeneity caused by a “threshold effect” was analyzed by visual assessment of the coupled forest plots of the sensitivity and the specificity. A meta-analysis of diagnostic test accuracy studies jointly analyzes a pair of outcomes (ie, sensitivity and specificity). Sensitivity and specificity are generally inversely correlated and affected by the threshold effect.25⇓–27 Additionally, the Spearman correlation coefficient between the sensitivity and the false-positive rate was also obtained. A Spearman correlation coefficient of >0.6 indicates a considerable threshold effect.35
The summary sensitivity and specificity values were calculated by the using hierarchic summary receiver operating characteristic (HSROC) and bivariate random-effects modeling.25⇓–27 We obtained the diagnostic odds ratio, which is a single parameter of diagnostic accuracy.27 The HSROC curve with a 95% confidence region and prediction region was also plotted to graphically present the results. Summarizing the results of original studies with the HSROC curve rather than by using summary points, including summary sensitivity or summary specificity, is recommended.27 We obtained the area under the curve from the HSROC curve. If a test is perfectly accurate, the value of the area under the curve is 1.0 and decreases toward 0.5 as the diagnostic accuracy of the test decreases.
Publication bias was visually assessed by using the Deeks funnel plot, and the statistical significance was tested by using the Deeks asymmetry test. We used the MIDAS and METANDI modules in STATA 10.0 (StataCorp, College Station, Texas) to perform the statistical analyses.
Results
Literature Search
Our study selection process is described in Fig 1. The literature search of the Ovid-MEDLINE and EMBASE data bases initially generated 718 articles, and 610 articles were screened for eligibility after removing 108 duplicates. Of the remaining articles, 582 were excluded after reviewing the titles and abstracts, including 493 articles that were not in the field of interest (ie, they did not discuss the diagnostic performance of CT for evaluating cervical lymph node metastasis in patients with papillary thyroid cancer), 63 case reports or series containing <10 relevant patients, and 26 review articles. The full texts of the remaining 28 articles were then retrieved. Searches of the bibliographies of articles identified 2 additional, eligible studies.14,22 Of these 30 articles, 21 were further excluded after reviewing the full text (ie, 13 studies that only used US, 2 studies that used US and PET/CT, 1 study that used US and MR imaging, 2 studies that were not in the field of interest, 2 studies that reported insufficient data to construct a diagnostic 2-by-2 table, and 1 study with a partially overlapping patient cohort). Finally, 9 eligible studies, including a total sample size of 1691 patients, were included in this meta-analysis.14⇓⇓⇓⇓⇓⇓⇓–22

Flow diagram of the study selection process.
Characteristics of the Included Studies
The detailed characteristics of the 9 included studies are summarized in the On-line Table. Three of the included studies were prospective,14,20,21 and the remaining 6 were retrospective.15⇓⇓⇓–19,22 The CT criteria for cervical lymph node metastasis were similar in studies using morphologic criteria, though 4 studies added size criteria.14,15,20,21 The US criteria for cervical lymph node metastasis were variable. The final diagnoses of cervical lymph nodes were determined on the basis of the pathology reports of surgical specimens in all of the included studies.14⇓⇓⇓⇓⇓⇓⇓–22 The quality of the included studies, as assessed by using QUADAS-2, was moderate overall, and all the studies satisfied ≥6 of the 7 items (Fig 2).33

Quality Assessment of the Diagnostic Accuracy Studies-2 criteria for the included studies.
Diagnostic Performance of CT and US for All Cervical Lymph Nodes by Level-by-Level Analysis
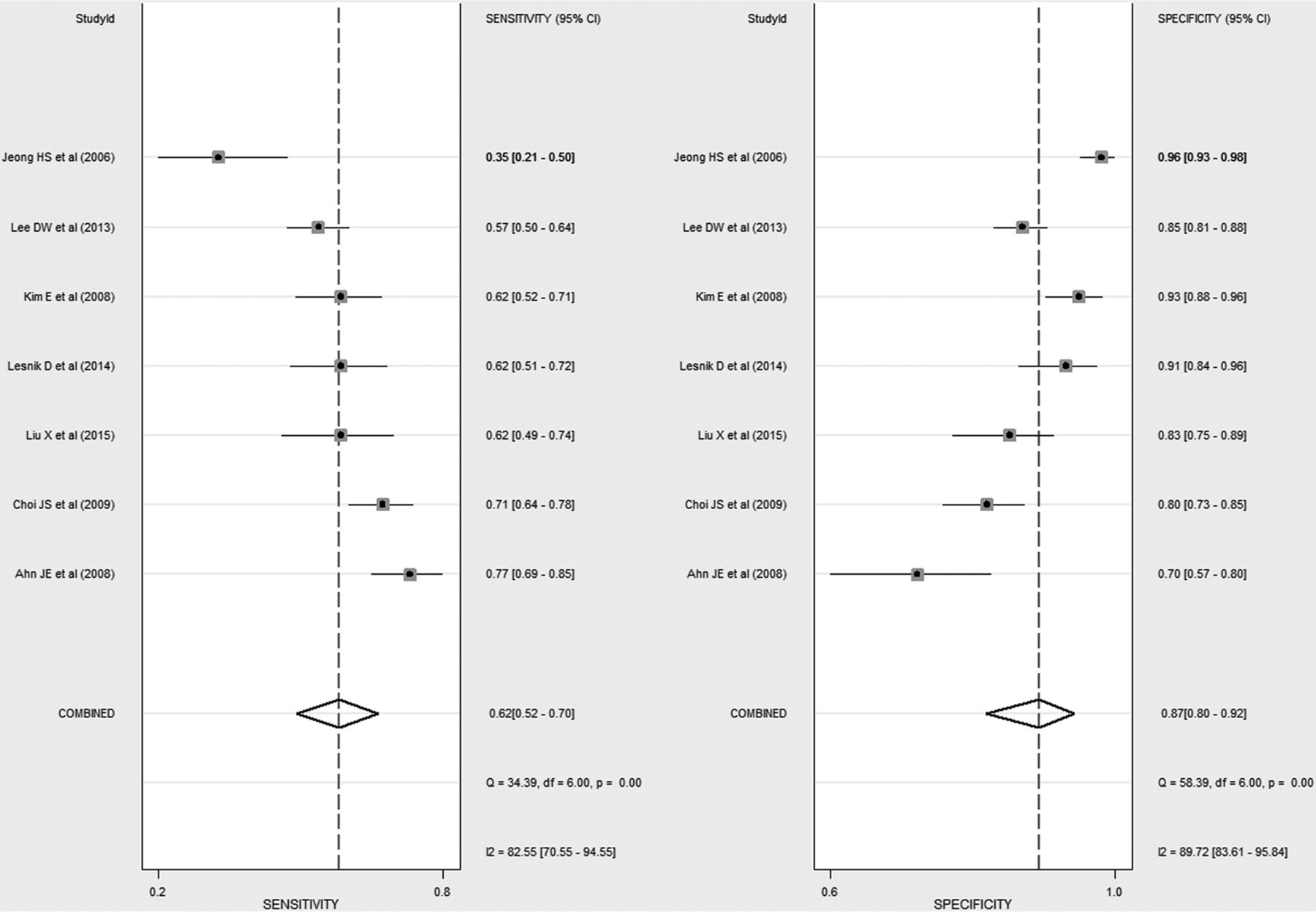
Data were collected from 7 CT studies with 926 patients concerning the diagnostic performance of CT.14⇓⇓–17,19⇓–21 The sensitivities and specificities of the individual studies were 35%–77% and 70%–96%, respectively. The Higgins I2 statistics demonstrated a substantial heterogeneity regarding both sensitivity (I2 = 82.6%) and specificity (I2 = 89.7%). The coupled forest plots of the sensitivity and specificity revealed a threshold effect (Fig 3), and the Spearman correlation coefficient between the sensitivity and the false-positive rate was 0.807 (95% CI, 0.136–0.970), thus also indicating the presence of the threshold effect.

Coupled forest plots of the sensitivity and specificity of CT for diagnosing cervical lymph node metastasis in patients with papillary thyroid cancer. Horizontal lines indicate 95% CIs of the individual studies.
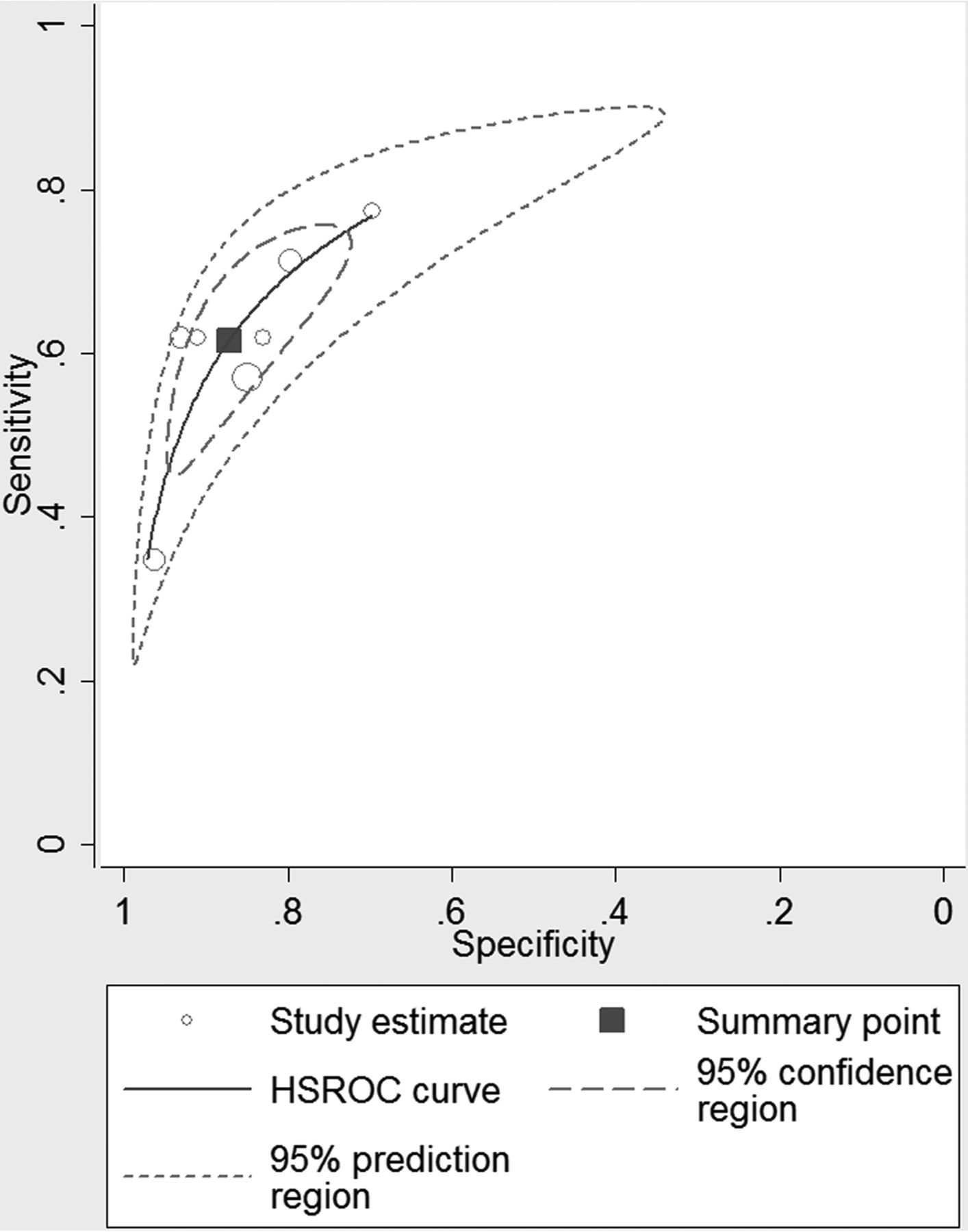
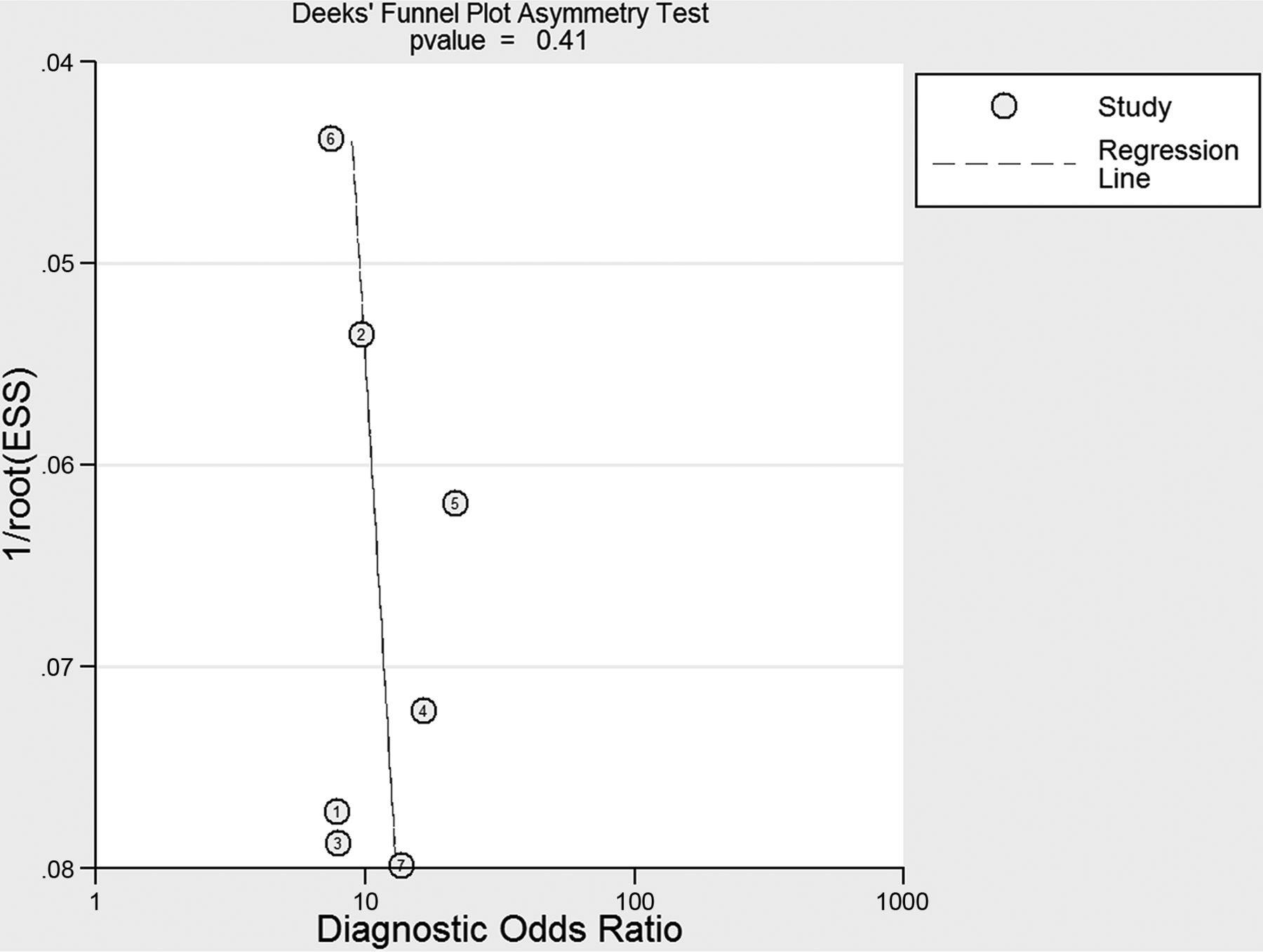
The pooled sensitivities and specificities of CT and US are summarized in the Table. CT demonstrated a summary sensitivity of 62% (95% CI, 52%–70%) and a specificity of 87% (95% CI, 80%–92%). The diagnostic odds ratio was 11 (95% CI, 8–15). The HSROC curve was symmetric, and there was only a small difference between the 95% confidence region and the 95% prediction region, thus indicating little heterogeneity between the studies (Fig 4). The area under the HSROC curve was 0.80 (95% CI, 0.77–0.84). No significant publication bias existed among the studies (P = .41) (Fig 5).
Results of meta-analytic summary estimates of CT and US for diagnosing cervical lymph node metastasis in patients with papillary thyroid cancer by level-by-level analysis

Hierarchic summary receiver operating characteristic curve of the performance of CT for diagnosing cervical lymph node metastasis in patients with papillary thyroid cancer.

The Deeks funnel plot to evaluate publication bias.
Data were collected from 6 US studies with 874 patients.14⇓⇓–17,19,20 The sensitivities and specificities of the individual studies were 40%–66% and 79%–96%, respectively. The Spearman correlation coefficient between the sensitivity and false-positive rate was 0.960 (95% CI, 0.675–0.996), thus indicating the presence of the threshold effect. US demonstrated a summary sensitivity of 51% (95% CI, 42%–60%) and a specificity of 91% (95% CI, 85%–95%). The diagnostic odds ratio was 11 (95% CI, 7–16). The area under the HSROC curve was 0.74. The summary estimates of sensitivity (P = .127) and specificity (P = .351) did not differ between CT and US.
Comparison of CT and US according to Lateral and Central Cervical Lymph Nodes by Level-by-Level Analysis
Concerning the lateral cervical lymph nodes, CT demonstrated a summary sensitivity of 70% (95% CI, 59%–80%) and a specificity of 89% (95% CI, 81%–94%) and US demonstrated a summary sensitivity of 71% (95% CI, 57%–82%) and a specificity of 85% (95% CI, 64%–95%) (Table). The summary estimates of sensitivity (P = .858) and specificity (P = .792) did not differ between CT and US. Regarding central cervical lymph nodes, CT demonstrated a summary sensitivity of 57% (95% CI, 43%–69%) and a specificity of 85% (95% CI, 72%–92%), and US demonstrated a summary sensitivity of 38% (95% CI, 27%–52%) and a specificity of 91% (95% CI, 81%–96%). Although the summary sensitivity of CT was higher than that of US, there was no significant difference (P = .088). The summary specificity (P = .368) did not differ between CT and US.
Added Value of Combined CT/US by Level-by-Level Analysis
Four studies reported combined CT/US for diagnosing cervical lymph node metastasis.16,17,19,20 The sensitivity ranged from 61% to 80%, and the lower margin of the 95% CI reached 54%. The specificity ranged from 69% to 88%, and the lower margin of the 95% CI reached 62%. Combined CT/US demonstrated a summary sensitivity of 69% (95% CI, 61%–77%) and a specificity of 81% (95% CI, 74%–87%). The summary sensitivity of combined CT/US was significantly higher than that of US (P = .011), though the summary specificity did not differ (P = .074).
Performance of CT and US for Diagnosing Cervical Lymph Node Metastasis by Patient-Based Analysis
Pooling was not performed due to the relatively small number of studies (n = 4) used for these analyses.16,18,19,22 The sensitivity of CT was variable, ranging from 31% to 59%; and the lower margin of the 95% CI reached 22%. The specificity of CT ranged from 84% to 94%, and the lower margin of the 95% CI reached 77%. The sensitivity of US was variable, ranging from 24% to 47%, and the lower margin of the 95% CI reached 17%. The specificity of US ranged from 80% to 92%, and the lower margin of the 95% CI reached 74%.
Discussion
Our current systematic review with a meta-analysis demonstrated that CT showed a summary sensitivity of 62% and a specificity of 87% for diagnosing cervical lymph node metastasis in patients with papillary thyroid cancer by a level-by-level analysis. There was a positive correlation between the sensitivity and the false-positive rate (correlation coefficient of 0.807) because of the threshold effect. In terms of the comparison of CT and US, the summary estimates of the sensitivity and specificity did not differ between CT and US for all cervical lymph nodes and lateral/central lymph nodes. However, the summary sensitivity of combined CT/US (69%) was significantly higher than that of US (51%), though the summary specificity did not differ. These results suggest that the diagnostic performances of CT and US are similar but that CT and US combined are superior to US only for the detection of cervical lymph node metastasis in patients with papillary thyroid cancer by a level-by-level analysis.
During the past decade, many studies have described the diagnostic performance of CT for cervical lymph node metastasis in patients with papillary thyroid cancer.14⇓⇓⇓⇓⇓⇓⇓–22 CT is a standardized, objective imaging technique that is less operator-dependent compared with US. In addition, CT provides detailed axial anatomic information systematically from the base of the skull to the mediastinum, which is familiar to most thyroid surgeons. Moreover, CT can evaluate lymph nodes in the retropharyngeal, retrosternal, and mediastinal areas.20 As the new American Thyroid Association guidelines suggest, CT can also be useful for evaluating the tumor extent involving the larynx, trachea, or esophagus as well as showing extranodal extension involving surrounding critical structures.7 Our meta-analysis revealed that the summary sensitivity of combined CT/US (69%) was significantly higher than that of US (51%) (P = .011). This improved sensitivity of combined CT/US allows better surgical planning and a better chance for removing all suspected cervical lymph node metastasis during surgery. Therefore, we believe that combined CT/US may have a supportive role, especially for preoperative surgical planning in patients with suspected lymph node metastasis or a high-risk of lymph node metastasis.16,23
The use of iodine-based contrast materials was strongly restricted before the operation due to the concern for disturbed radioactive iodine uptake for months and the delay of radioiodine treatment.36 Therefore, contrast-enhanced CT has not been recommended for the preoperative diagnosis of cervical lymph node metastasis. However, several recent studies have reported the supposition that the delay of radioiodine therapy was not necessary in patients who underwent contrast-enhanced CT because the iodine is generally cleared within 4–8 weeks in most patients, and the body iodine content is not an essential determinant of thyroid ablation.37⇓⇓⇓–41 Therefore, the benefit gained from improved anatomic imaging generally outweighs any potential risk regarding a several-week delay in radioactive iodine imaging or therapy.
In our meta-analysis, our summary estimates demonstrate consistent results despite heterogeneity. The Higgins I2 statistic demonstrated a substantial heterogeneity in both the sensitivity (I2 = 82.6%) and specificity (I2 = 89.7%) of CT. However, there was a positive correlation between and sensitivity and the false-positive rate (correlation coefficient of 0.807), which would be expected in a meta-analysis of diagnostic test accuracy studies due to the threshold effect. This correlation indicates that our heterogeneity was mainly caused by the threshold effect. CT criteria for cervical lymph node metastasis in our included studies were similar, though several studies used not only morphologic criteria but also size criteria, which may cause the threshold effect.26,27 Morphologic criteria include central necrosis or cystic change, strong enhancement without hilar vessel enhancement, calcification, and round shape with loss of the fatty hilum (On-line Table). The possibility of a node with only mild enhancement would be very low for lymph node metastasis. In addition, the US criteria for cervical lymph node metastasis were also variable between studies. The US criteria included cystic change, the absence of a hilum, microcalcification, heterogeneity, and size.
We used validated systematic review methods and reported our data according to standard reporting guidelines, including the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA),42 the guidelines of the Handbook for Systematic Reviews of Diagnostic Test Accuracy by the Cochrane Collaboration,43 and the guidelines of the Agency for Healthcare Research and Quality.44 We determined the diagnostic performance of CT by using more recently developed robust methodology (ie, the HSROC model or the bivariate random-effects model).25⇓–27 Therefore, this study, which gathered currently available evidence, was needed and will help to advance daily clinical practice.
Our study had several limitations. First, it included relatively few studies (ie, 9). In addition, the sample size of the number of included studies in the meta-analysis according to the central/lateral lymph nodes was small. Nonetheless, a small number of statistically significant differences were elucidated. Second, as addressed earlier, the CT or US criteria for cervical lymph node metastasis were similar but somewhat variable between studies because no consistent criteria have been established regarding cervical lymph node metastasis. The threshold effect is probably caused by these variable criteria. Third, 7 of 9 studies included reflect single-country data; however, these are the only available studies.14⇓⇓⇓⇓–19,22 Fourth, the specificity of combined CT/US is lower than that of US alone; however, it is not statistically significant.
Conclusions
The diagnostic performances of CT and US are similar, though CT and US combined are superior to US only for the detection of cervical lymph node metastasis in patients with papillary thyroid cancer by a level-by-level analysis. CT may be used as a complementary method in addition to US for diagnosing cervical lymph node metastasis in patients with papillary thyroid cancer.
References
- Received April 1, 2016.
- Accepted after revision August 22, 2016.
- © 2017 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Diagnostic accuracy of ultrasound, CT and their combination in detecting cervical lymph node metastasis in patients with papillary thyroid cancer: a systematic review and meta-analysis
- A Scoring System for Prediction of Cervical Lymph Node Metastasis in Patients with Head and Neck Squamous Cell Carcinoma