
Abstract
BACKGROUND AND PURPOSE: Germinal matrix hemorrhage is a frequent complication of prematurity and can be associated with adverse neurodevelopmental outcome, depending on its severity. In addition to parenchymal damage, intraventricular residues of hemorrhage and hydrocephalus MR imaging findings include superficial siderosis. The purpose of this study was to investigate the prevalence and location of superficial siderosis in patients with a history of germinal matrix hemorrhage.
MATERIALS AND METHODS: We retrospectively identified patients with a history of germinal matrix hemorrhage who underwent MR imaging in our institution between 2008 and 2016. Imaging was evaluated for the presence and location of superficial siderosis. The presence of subependymal siderosis and evidence of hydrocephalus were assessed.
RESULTS: Thirty-seven patients with a history of germinal matrix hemorrhage were included; 86.5% had preterm births. The mean age at the first MR imaging was 386 days (range 2–5140 days). The prevalence of superficial siderosis was 67.6%. Superficial siderosis was detected significantly more often when MR imaging was performed within the first year of life (82.8% versus 12.5%, P < .000). When present, superficial siderosis was located infratentorially in all cases, while additional supratentorial superficial siderosis was detectable in 27%.
CONCLUSIONS: Here we report that superficial siderosis is a common MR imaging finding in the first year of life of patients with a history of germinal matrix hemorrhage, but it dissolves and has a low prevalence thereafter. A prospective analysis of its initial severity and speed of dissolution during this first year might add to our understanding of the pathophysiology of neurodevelopmental impairment after germinal matrix hemorrhages.
The germinal matrix is a highly cellular and vascularized layer between the thalamus and caudate nucleus. It is the origin of neurons and glial cells during fetal development and begins to involute at 28 weeks' gestational age. Due to the friability of its capillaries, it is vulnerable to bleeding when autoregulation of cerebral blood flow is not yet established as in preterm infants.1 Germinal matrix hemorrhage is a frequent complication of prematurity associated with developmental delay, cerebral palsy, neurosensory impairment, and deafness.2 The risk of neurodevelopmental impairment increases with the severity of the hemorrhage,3 which is graded according to the Papile classification.1,4 Grade I hemorrhages (restricted to germinal matrix without extension into ventricles) are not associated with developmental delay.
In addition to parenchymal damage, intraventricular residues of hemorrhage and hydrocephalus superficial siderosis is a finding that has been described in cases of germinal matrix hemorrhage.5,6 In adult neurology, superficial siderosis has been associated with gait ataxia, cerebellar dysarthria, and sensorineural hearing impairment.7 After germinal matrix hemorrhage however, it is assumed to be an incidental finding without neurodevelopmental implications.6 The purpose of this study was to investigate the prevalence and location of superficial siderosis in patients with a history of germinal matrix hemorrhage.
Materials and Methods
We retrospectively included all patients with a known history of germinal matrix hemorrhage who underwent MR imaging in our institution between 2008 and 2016. Patients were identified by a search in our electronic in-hospital data base (SAP, Walldorf, Germany) of clinical records for the key words “germinal matrix hemorrhage.”
Inclusion criteria were as follows:
A history of germinal matrix hemorrhage diagnosed by sonography or MR imaging.
MR imaging including a T2*-weighted sequence or SWI.
The exclusion criterion was imaging quality insufficient to recognize the presence of superficial siderosis.
Imaging was performed on a 1.5T scanner (Sonata; Siemens, Erlangen, Germany) between 2008 and 2011 and on either a 1.5T scanner (Symphony; Siemens) or a 3T scanner (Skyra; Siemens) between 2011 and 2016.
At our institution, MR imaging in children is routinely performed with the patient under deep sedation or general anesthesia. MR imaging was typically performed to confirm the finding of a germinal matrix hemorrhage in a sonography examination and to plan surgery in case of hydrocephalus.
Image interpretation was performed by 2 neuroradiologists in consensus. T2*-weighted images or SWI were evaluated for the presence and location of superficial siderosis. The presence of subependymal siderosis and evidence of hydrocephalus were also assessed. Gestational age at birth and age at MR imaging were noted. Statistical analysis was performed by using SPSS 20.0 (IBM, Armonk, New York). The χ2 test was applied to determine differences in frequencies.
P < .05 was considered statistically significant.
Results
Thirty-seven patients with a history of germinal matrix hemorrhage were included. Thirty-two (86.5%) had preterm births. The mean gestational age at birth was 30 weeks (range, 25–39 weeks). Data on the severity of the hemorrhage were available for 31 patients. Two patients had grade I hemorrhages according to the Papile classification and the initial sonography examinations. However, grades were corrected to grade II because MR imaging showed subependymal siderosis exceeding the germinal matrix in both cases. Frequencies according to the Papile classification were the following: grade I, 0%; grade II, 45.2% (12/31); grade III, 41.9% (13/31); and grade IV, 12.9% (4/31). The mean age at the first MR imaging investigation was 386 days (range, 2–5140 days). Subependymal siderosis was detectable in every case (37/37). Thirty-two patients (86.5%) had evidence of hydrocephalus. The prevalence of superficial siderosis was 67.6% (25/37). Superficial siderosis was located infratentorially in all of those cases, while additional supratentorial superficial siderosis was detectable in 27% (10/37).
Superficial siderosis was detected significantly more often when the first MR imaging was performed within the first year of life (82.8% [24/29] versus 12.5% [1/8], P < .000). The first MR imaging was performed within the first 6 months in 20 neonates. In this group, superficial siderosis was found in 90% (18/20). Follow-up MR imaging after their first year of life was available in 10 of those patients who had superficial siderosis on MR imaging in their first year of life. The mean age at the follow-up MR imaging investigation was 1013 days (range, 424–2371 days). Superficial siderosis was detected in 1 case on follow-up MR imaging (9.1%), whereas subependymal siderosis was present in all cases (11/11) (exemplary cases are shown in Figs 1 and 2). Two of the 5 patients without hydrocephalus had the first MR imaging within their first year of life (at 55 days and 56 days). Superficial siderosis was detected in both cases. Neither patient underwent follow-up MR imaging. The other 3 patients without hydrocephalus underwent MR imaging at 1 and 2 years of age. None of these MRIs showed superficial siderosis. Data on the severity of the hemorrhage were available for 4 patients without hydrocephalus. Two of them had grade II hemorrhages, and 2, grade III hemorrhages.

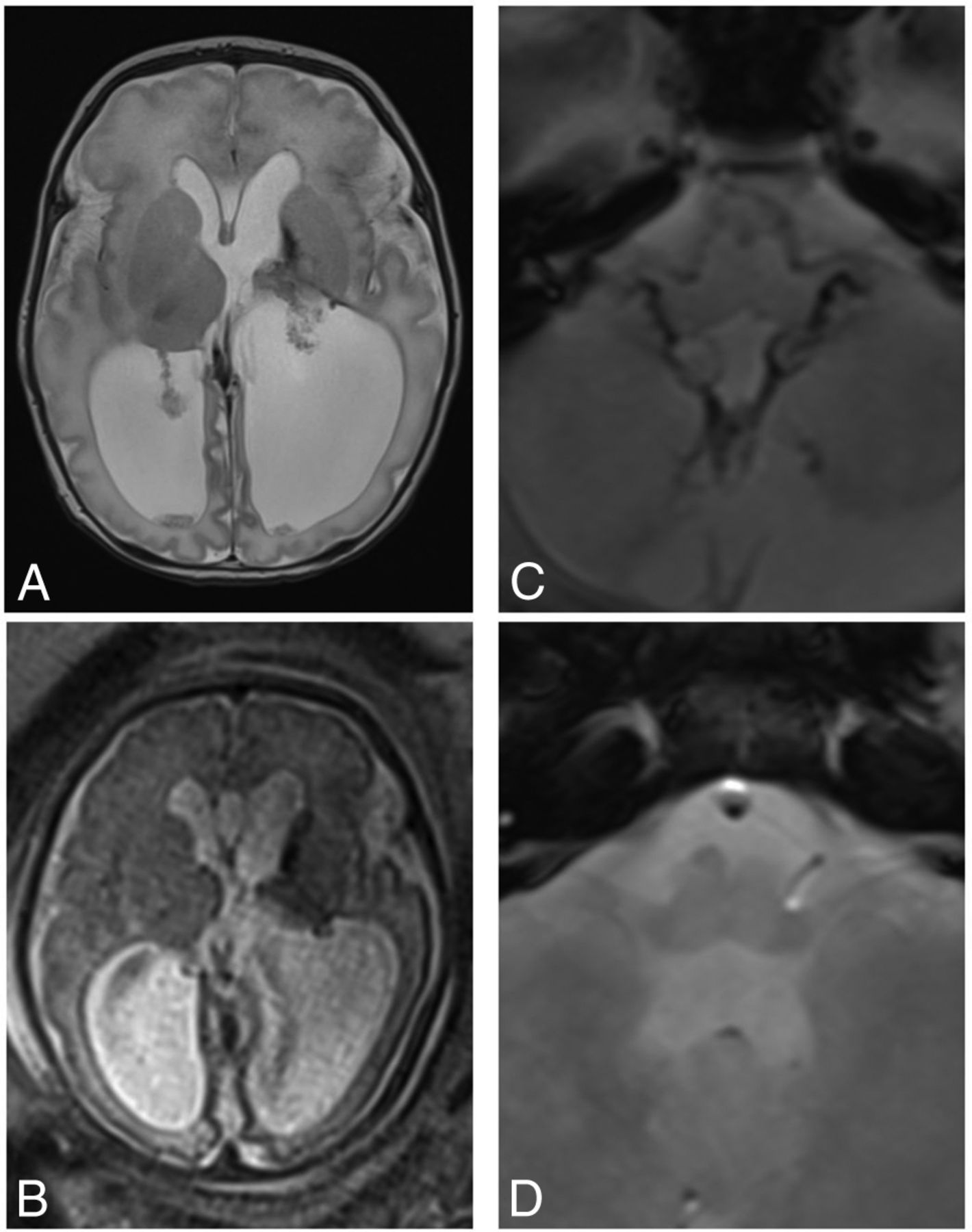
Superficial siderosis after germinal matrix hemorrhage. T2-weighted (A) image of a male neonate at 2 days of age shows residues of a left germinal matrix hemorrhage and secondary hydrocephalus. Gestational age at birth was 34 weeks. At the gestational age of 32 weeks, a fetal MR imaging had been performed (B) after hemorrhage had been suspected on a prenatal sonography examination. Postnatal T2*-weighted image (C) shows infratentorially located superficial siderosis, which had dissolved on the T2*-weighted image at 26 months of age (D).

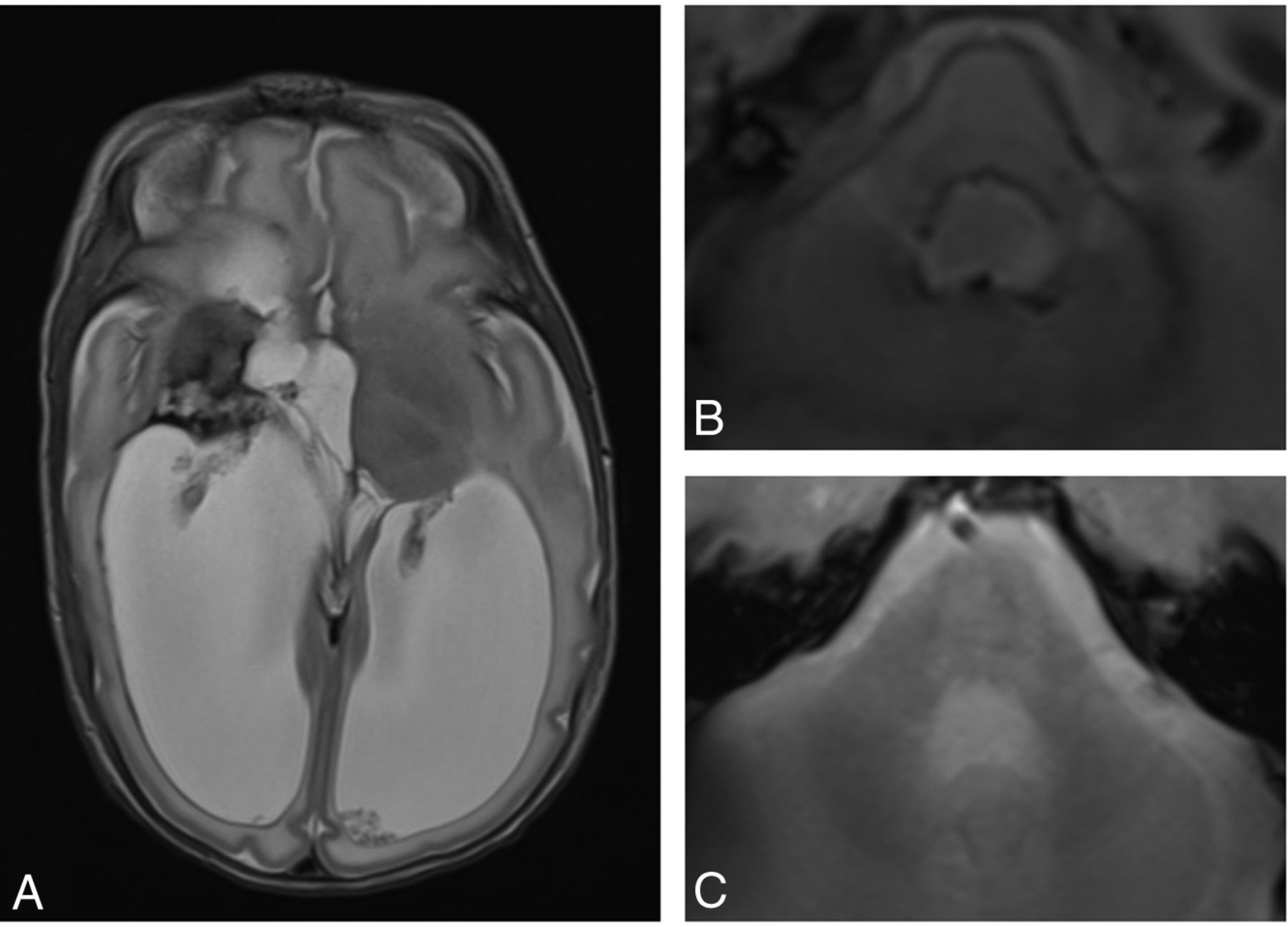
Superficial siderosis after germinal matrix hemorrhage. T2-weighted (A) image of a female infant at the age of 2 months shows residues of a right germinal matrix hemorrhage with parenchymal defects and secondary hydrocephalus. T2*-weighted image (B) shows infratentorially located superficial siderosis, which had dissolved on the T2*-weighted image at 3 years of age (C).
Discussion
In this study, we investigated superficial siderosis in patients with a history of germinal matrix hemorrhage. Gomori et al5 first described 2 cases of large germinal matrix hemorrhages with signs of superficial siderosis on MR imaging in 1987. Glasier et al6 later reported superficial siderosis in 7 infants with a history of intraventricular/periventricular hemorrhage. In addition, they retrospectively analyzed the neurodevelopmental outcomes of their patients with particular attention to cerebellar and auditory dysfunction and concluded that superficial siderosis is an incidental finding without neurodevelopmental implications. However very recently, a cohort study of extremely preterm infants2 reported higher rates of neurosensory impairment and hearing loss in infants with intraventricular hemorrhages compared with preterm controls at 2–3 years' corrected age. Increasing grades of hemorrhages were associated with higher rates of neurosensory impairment (12.1% in controls, 21.1% for grade I, 24% for grade II, 41% for grade III, and 46% for grade IV).2 The mechanism of brain injury is thought to result from parenchymal damage and impaired cortical development.2 In addition, Silva et al8 recently reported that peri-/intraventricular hemorrhages influence alterations in auditory brain stem responses in preterm infants.
In our study, superficial siderosis was commonly seen in patients with a history of germinal matrix hemorrhage when MR imaging was performed in the first year of life, with dissolution in >90% thereafter. To our knowledge, this is the first report of the age-dependent dissolution of superficial siderosis after germinal matrix hemorrhage. Because superficial siderosis has been associated with gait ataxia, cerebellar dysarthria, and sensorineural hearing impairment in adults,7 it may also have an impact on the neurodevelopmental outcome in infants with germinal matrix hemorrhages. In this context, it would be interesting to prospectively investigate the extent of the superficial siderosis, the gestational age at which it occurs, and the speed of its dissolution as potential modifying factors with regard to neurologic outcome.
Limitations
Our study has some limitations. Because the disappearance of superficial siderosis is probably a gradual process, it would be interesting to quantify its extent with time. However, because imaging quality was very divergent in our analysis due to different scanners with different field strengths and different section thicknesses, we decided not to attempt to quantify the siderosis but to restrict our analysis to its presence or absence. In this context, it would also be interesting to analyze factors that might influence the extent of superficial siderosis, such as the size of the initial hematoma. Because our study was retrospective in character, such information was not sufficiently available.
Conclusions
Superficial siderosis is a common MR imaging finding in the first year of life in neonates with a history of germinal matrix hemorrhage, but it dissolves and has a low prevalence thereafter. A prospective analysis of its initial severity and speed of dissolution during this first year may add to our understanding of the pathophysiology of neurodevelopmental impairment after germinal matrix hemorrhages.
References
- Received May 24, 2016.
- Accepted after revision July 20, 2016.
- © 2016 by American Journal of Neuroradiology





{kind=link}
{kind=link}