
Abstract
BACKGROUND AND PURPOSE: The morphologic features of brain arteriovenous malformations differ between children and adults; therefore, our aim was to analyze various features of brain arteriovenous malformations to assess the risk of hemorrhage in children.
MATERIALS AND METHODS: We identified all consecutive children admitted to Beijing Tiantan Hospital for brain arteriovenous malformations between July 2009 and April 2014. The effects of demographic characteristics and brain arteriovenous malformation morphology on hemorrhage presentation, annual bleeding rates, postnatal hemorrhage, and immediate posthemorrhagic neurologic outcomes were studied by using univariate and multivariable regression analyses.
RESULTS: A total of 108 pediatric brain arteriovenous malformation cases were identified, 66 (61.1%) of which presented with hemorrhage. Of these, 69.7% of ruptured brain arteriovenous malformations were in a periventricular location. Periventricular nidus location (OR, 3.443; 95% CI, 1.328–8.926; P = .011) and nidus size (OR, 0.965; 95% CI, 0.941–0.989; P = .005) were independent predictors of hemorrhagic presentation. The annual hemorrhage rates in children with periventricular brain arteriovenous malformations were higher at 6.88% (OR, 1.965; 95% CI, 1.155–3.341; P < .05). The hemorrhage-free survival rates were also lower for children with periventricular brain arteriovenous malformations (log-rank, P = .01). Periventricular location (hazard ratio, 1.917; 95% CI, 1.131–3.250; P = .016) and nidus size (hazard ratio, 0.983; 95% CI, 0.969–0.997; P = .015) were associated with hemorrhage after birth in pediatric brain arteriovenous malformations. An ordinal analysis showed lower immediate posthemorrhage mRS in patients with periventricular brain arteriovenous malformations (OR for greater disability, 2.71; 95% CI, 1.03–7.11; P = .043).
CONCLUSIONS: Small periventricular brain arteriovenous malformations were associated with increased hemorrhage risk in pediatric patients. Cautious follow-up of children with untreated periventricular brain arteriovenous malformations is recommended because of a higher hemorrhage risk and potentially more severe neurologic outcomes.
ABBREVIATIONS:
- BAVM
- brain arteriovenous malformations
- ICH
- intracranial hemorrhage
- IVH
- intraventricular hemorrhage
Hemorrhagic stroke accounts for half of pediatric strokes and is a life-threatening disease with a mortality rate of >30% and permanent deficits in up to 40% of patients.1⇓–3 Brain arteriovenous malformations (BAVMs) have been proved to be the underlying cause of most intracranial hemorrhage (ICH) in children.4 In contrast to adult patients, children with BAVMs are more likely to present initially with ICH, while the overall annual hemorrhage rate for pediatric BAVM does not exceed that of adults.5 A long-term follow-up study revealed that childhood presentation may provide relative protection against subsequent ICH.6 Recent studies have indicated that the angioarchitectural features of BAVM differed between children and adults, but specific studies of hemorrhagic risk assessment in children have been limited.7
Previous studies have been performed primarily in adults or patients of all ages and have shown that presentation with hemorrhage is the most important and widely accepted risk factor for future bleeding from BAVMs.8⇓–10 Meta-analyses of natural history studies and large-scale cohort studies failed to reach a consensus regarding the role of other factors such as nidus size, exclusive deep venous drainage, associated arterial aneurysm, and deep location.11⇓–13 A periventricular location has also been found to correlate positively with the risk of hemorrhage before the treatment of BAVMs.14,15 However, this feature, although amenable to analysis with imaging, has not been studied carefully in the risk assessment of interventional-versus-observational treatment.
This study was based on the hypothesis that a periventricular location, along with other morphologic features such as deep location, posterior fossa location, nidus size, exclusively deep venous drainage, and associated aneurysm, is a potential risk factor for BAVM rupture and unfavorable outcomes in pediatric patients. The study aimed to accomplish the following objectives: 1) to assess the association of these factors with the risk of hemorrhage in children with BAVMs; 2) to evaluate the hemorrhage-free survival of children with and without these factors, assuming that the BAVM had been present from birth; 3) to study the associations of these factors with the time from birth to first hemorrhage; and 4) to compare the hemorrhage site, severity of the acute presentation, and the type of intervention in ruptured periventricular and nonperiventricular BAVMs.
Materials and Methods
The study protocol was approved by the institutional review board of Beijing Tiantan Hospital. Written informed consent was obtained from all participants and/or their guardians at admission.
Patients and Study Design
The Tiantan BAVM data base has been previously described and is a prospectively maintained data base collecting demographic, clinical, and neuroradiologic data for all patients with a confirmed angiographic or histologic diagnosis of BAVM treated at Beijing Tiantan Hospital, Capital Medical University.16 This data base was retrospectively queried to identify all consecutive children diagnosed with BAVMs between July 2009 and April 2014. Pediatric patients were defined as patients who were 18 years of age or younger at the first angiographic diagnosis of BAVM (excluding dural and pial arteriovenous fistulas and vein of Galen malformations).
BAVM hemorrhage was defined as a symptomatic clinical event with signs of fresh intracranial blood on CT or MR imaging and/or in the CSF, with no easily identifiable alternative source that was more likely to be the cause than the BAVM. All hemorrhages before treatment for BAVM were documented. Annual hemorrhage rates were calculated as the ratio of the number of hemorrhages to the total number of patient-years of follow-up. We calculated patient-years of follow-up, assuming that the BAVM was present from birth until the first treatment for BAVM. For the BAVM hemorrhage-free survival analysis, the primary outcome was the first hemorrhage from BAVM, and patients were censored at the time of any interventional treatment for the BAVM or at the time of the last follow-up.
Neurologic function at hemorrhage onset was assessed by using the mRS and Glasgow Coma Scale. The immediate posthemorrhage mRS and Glasgow Coma Scale scores were recorded within 24 hours of the presenting hemorrhage. A clinician who was not directly involved in the care of these patients performed all scale assessments. Emergency intervention for ICH evacuation or drainage was considered in patients with a Glasgow Coma Scale score of ≤8, ICH with neurologic deficit, or intraventricular hemorrhage (IVH) with hydrocephalus.
Neuroradiologic Review
MR imaging, CT, and angiographic images available for each patient were evaluated by consensus between 2 neuroradiologists (J.M., with 24 years of experience, and W.B.G., with 10 years of experience) who were blinded to the clinical information. A structured list of angiographic and MR imaging features was retrospectively scored by using a protocol that generally conformed to the consensus recommended by a Joint Writing Group for BAVM research reporting terminology.17 Variants that were reported to be predictive of BAVM rupture but were not expanded in the recommended protocol were defined with reference to previous studies.18⇓–20
BAVM location was dichotomized into deep (basal ganglia, thalamus, cerebellum, and corpus callosum) and superficial (all other locations). A posterior fossa location was defined as brain stem, cerebellum, or both. BAVMs were also classified as having a periventricular location if the nidus (with a contrast-enhancement or flow void) contacted the ependymal lining of the ventricle on contrast-enhanced T1- and T2-weighted images.14,21,22 To reduce the confounding effects of hematoma on the imaging analysis for patients with hemorrhages, we evaluated all MR images available before treatment (Fig 1). For the few patients who underwent emergency treatment but had no MR images obtained before the BAVM rupture, the BAVM location was identified on CT according to the consensus of the 2 neuroradiologists.

Ruptured BAVMs having a periventricular location. Patient A was diagnosed with right occipital BAVM. Axial T2WI on posthemorrhage day 3 (A and B) and 1 month later (C and D). The relationship between the ventricle and BAVM lesion is explicit at 1 month after hemorrhage. Patient B was diagnosed with right temporal BAVM. Axial T2WI (E and F) and postcontrast T1WI (G and H) on posthemorrhage day 14. The hematoma does not obscure the nidus edge contacting the ventricle.
ICHs were classified as intraparenchymal hemorrhage, IVH, SAH, or a combination of the above 2 or 3 locations. Hematoma volume was evaluated with an ellipsoid method.23 Hematomas were defined as deep if the basal ganglia, thalamus, brain stem, cerebellum, or corpus callosum was involved.
Venous drainage was dichotomized into exclusively deep venous drainage or nonexclusively deep venous drainage (superficial-only drainage or superficial and deep drainage). An aneurysm was defined as a saccular dilation of the lumen >2 times the width of the arterial vessel that carried the dilation. An aneurysm was diagnosed when dilation was evident with no obvious overlap of neighboring vessels on 2 orthogonal (both coronal and sagittal) angiographic views. Associated aneurysms included only aneurysms related to shunt flow. For statistical analysis, the associated aneurysm variable was dichotomized into absent or present.
Each nidus was measured in 3 dimensions on the latest contrast-enhanced MR imaging and angiogram before BAVM rupture. The largest diameter (in millimeters) among the 3 dimensions was recorded as the maximal AVM size for further analysis.
Statistical Analysis
Data were analyzed by using SPSS Statistics, Version 20.0 (IBM, Armonk, New York). Statistical significance was set at P < .05. For the neuroradiologic and clinical data, patients with and without periventricular BAVMs were compared by using descriptive statistics, including t tests for continuous variables and χ2 tests for categoric variables. The κ coefficient was used to analyze the interobserver agreement between the 2 neuroradiologists.
We first examined the association of periventricular location with the time to hemorrhage, before any treatment. We performed Cox proportional hazards analysis of the time from birth to the first hemorrhage, censoring patients at the time of treatment or last follow-up. Kaplan-Meier survival curves and log-rank tests were used to evaluate hemorrhage-free survival for patients with and without periventricular BAVMs. Both univariate and multivariable Cox proportional hazards analyses were performed, including all potential risk factors for hemorrhage.
The second stage of the analysis examined the relationship between BAVM hemorrhage outcomes at presentation and periventricular location. Both univariate and multivariable logistic regression analyses were performed by using hemorrhage presentation and severe posthemorrhage presentation (mRS >3) as the outcomes, respectively, and periventricular location as the primary predictor. We created a multivariable model that included all the potential risk factors, regardless of whether they were significant on univariate analysis. The mRS scores were also analyzed by using both an unadjusted proportional-odds regression model across all levels of the scale and a proportional-odds regression model that adjusted for other baseline demographic and morphologic variables.
Results
Characteristics of the Study Population
A total of 108 pediatric patients with BAVM were identified. None of the patients had familial BAVM or hereditary hemorrhagic telangiectasia. Baseline characteristics are shown in Table 1. The age at diagnosis ranged from 1 to 18 years (mean age, 10.95 ± 4.13 years). Of these, 66 of 108 patients (61.1%) initially presented with ICH. Most patients experienced their first BAVM rupture during their first 12 years (48/66, 72.7%). The most common initial hemorrhage type was intraparenchymal hemorrhage (34/66, 51.5%), followed by intraparenchymal hemorrhage with IVH (19/66, 28.8%) and IVH (5/66, 7.6%). Exclusively deep venous drainage was found in 9.3% of the BAVMs, and associated aneurysm, in 13%. A deep location was encountered in 34.3%, and 7.4% involved the posterior fossa. Notably, 65 of 108 BAVMs (60.2%) were classified as periventricular, 70.8% of which presented with ICH. In significant contrast, 46.5% of BAVMs without ventricular involvement ruptured (P = .011). The periventricular BAVMs were more likely to have a deep location (P < .001) and to be diagnosed early (P = .022). However, these lesions were not more likely to have distinct venous drainage, and there was no significant difference in supra-/infratentorial distribution, associated aneurysm incidence, or nidus size in this series of patients (P > .05) (Table 1).
Baseline characteristics of periventricular and nonperiventricular BAVMsa
Association of Periventricular Location with Hemorrhage Presentation
Univariate analysis revealed that BAVMs with hemorrhage were more likely to be periventricular (69.7% versus 30.3%, P = .011). Moreover, the nidus size was significantly smaller in BAVMs that presented with hemorrhage (35.64 ± 18.54 mm versus 45.33 ± 18.25 mm, P = .009). BAVMs with hemorrhagic presentation were not different from the unruptured BAVMs with respect to demographic and morphologic factors, including exclusively deep venous drainage, deep location, infratentorial location, and associated aneurysm (Table 2).
Factors associated with hemorrhagic presentation by univariate analysisa
The multivariable model that adjusted for other potential risk factors showed that a periventricular location was highly predictive of hemorrhagic presentation (OR, 3.443; 95% CI, 1.328–8.926; P = .011) and that increased nidus size was relatively protective (OR, 0.965; 95% CI, 0.941–0.989; P = .005) in children with BAVMs. Age, sex, deep location, posterior fossa involvement, exclusively deep venous drainage, and associated aneurysms did not predict hemorrhagic presentations in these pediatric patients (On-line Table 1).
Association of Periventricular Location with Hemorrhage-Free Survival
If one assumes that the BAVM had been present since birth, there were 1279 patient-years of follow-up for this population of 108 patients (mean, 11.8 years). A total of 70 hemorrhages occurred in 66 patients with ruptured BAVMs, yielding an overall annual BAVM hemorrhage rate of 5.47% for pediatric patients. A total of 50 hemorrhages occurred in 46 patients with ruptured periventricular BAVMs during 727 patient-years of follow-up, yielding an annual hemorrhage rate of 6.88%. In contrast, of the 552 patient-years of follow-up in 20 patients with ruptured nonperiventricular BAVMs, only 20 hemorrhages occurred, yielding an annual hemorrhage rate of 3.62%. The odds ratio for rupture of periventricular BAVMs, compared with nonperiventricular BAVMs, was 1.965 (95% CI, 1.155–3.341).
There was a significant difference between the time to hemorrhage for patients with periventricular and nonperiventricular BAVMs (log-rank, P = .01). Periventricular BAVMs ruptured earlier before treatment, with a median hemorrhage-free survival of 11.00 years (95% CI, 9.31–12.69) for periventricular BAVMs and 16.00 years (95% CI, 14.29–17.71) for nonperiventricular BAVMs (Fig 2). There was a borderline significant association between the presence of an aneurysm and hemorrhage-free survival (log-rank, P = .052). We do not have sufficient data to support an association of deep location (log-rank, P = .488) or exclusively deep venous drainage (log-rank, P = .101) with earlier BAVM rupture in childhood before any treatment.

Kaplan-Meier curves demonstrating the hemorrhage-free survival difference between BAVMs with and without certain morphologic features.
Both univariate and multivariable Cox regression analyses were performed on the 108 pediatric patients (On-line Table 1). Although the univariate analysis identified a periventricular nidus location (hazard ratio, 1.917; 95% CI, 1.131–3.250; P = .016) and nidus size (hazard ratio, 0.983; 95% CI, 0.969–0.997; P = .015) as predictors of future hemorrhage risk in pediatric BAVMs, neither of these variables was significantly associated with earlier BAVM rupture independent of other characteristics in the multivariable model. Most unsurprising, the later the BAVM was diagnosed, the later the lesion ruptured, according to this follow-up approach.
Associations of Periventricular Location with Severe Presentation in Ruptured BAVMs
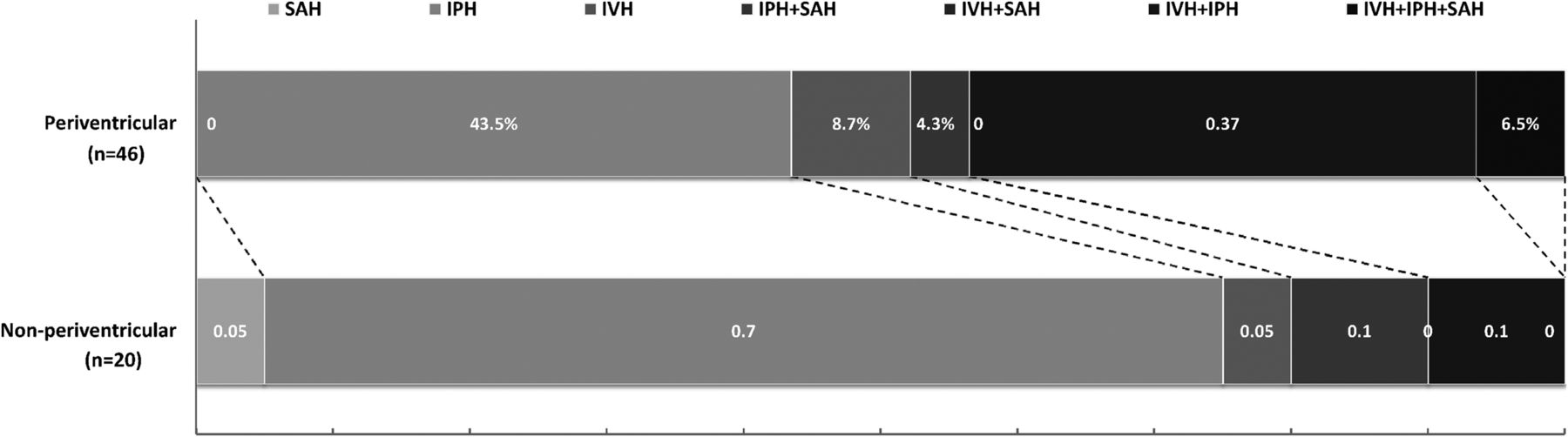
In the 66 pediatric patients with ruptured BAVMs, deep, large (>30 mL) hematomas and acute hydrocephalus were associated with a severe posthemorrhage presentation (On-line Table 2). There was a trend toward a higher risk of having an immediate posthemorrhage mRS of >3 in patients with periventricular BAVMs than in patients with nonperiventricular BAVMs (50% versus 25%, P = .059) (On-line Table 2 and On-line Fig 1). The unadjusted ordinal analysis showed a significant unfavorable shift in the distribution of immediate posthemorrhage mRS scores in patients with a periventricular nidus location (pooled odds ratio for a shift to a higher mRS score, 2.71; 95% CI, 1.03–7.11) (Table 3). In addition, periventricular BAVMs were significantly associated with ICH involving the ventricles (pure IVH, IVH with intraparenchymal hemorrhage, IVH with SAH, IVH with intraparenchymal hemorrhage and SAH) (52.17% versus 15.00%, P = .005). IVH with intraparenchymal hemorrhage was present in 17/46 (37%) ruptured periventricular BAVMs in contrast to only 2/20 (10%) nonperiventricular BAVMs (Fig 3 and On-line Fig 1). Further analysis revealed a higher frequency of deep (30.4%), large (26.1%) hematomas and acute hydrocephalus (21.7%) in ruptured periventricular BAVMs than in nonperiventricular BAVMs (On-line Fig 2).
Immediate posthemorrhage presentation severity according to different methods of analysis of scores on the mRS

Hemorrhage location of ruptured periventricular BAVMs and nonperiventricular BAVMs.
Immediate posthemorrhage Glasgow Coma Scale score of ≤8 occurred in 26.1% of children with periventricular BAVMs and 20.0% with BAVMs in other locations. Emergent interventions (craniotomy or external ventricular drainage for blood evacuation with or without decompressive craniectomy) were performed in 34.8% of children with periventricular BAVMs and in 20.0% with BAVMs in other locations. However, these differences were not statistically significant (On-line Fig 1).
Discussion
BAVM Hemorrhage Risk Predictors in Pediatric Patients
Many studies aimed at identifying morphologic features associated with BAVM hemorrhagic presentations and the risk of subsequent hemorrhage have been performed, mainly in adult patients.8⇓⇓⇓⇓–13 A recent angiographic study revealed that the angioarchitectural features of BAVM, some of which confer a higher risk for future hemorrhage in adults, differ between children and adults.7 However, only a few studies have specifically been conducted to assess the risk of pediatric BAVM hemorrhage and provide a prognosis before treatment (On-line Table 3).
Previous studies have reported the following factors to be associated with hemorrhage at presentation in children with BAVMs: smaller AVM nidus size, deep/exclusively deep venous drainage, single draining vein, and eloquent nidus location.24⇓⇓⇓–28 Most of these factors and results were obtained from a retrospective cohort (younger than 22 years of age) at Columbia University Medical Center.24,26,28 Two larger studies reported results with a relatively distinct bias (a wide range of odds ratio or only radiosurgery patients), suggesting that these studies might have been underpowered to assess the impact of certain features on BAVM hemorrhage.25,27
In this exclusively pediatric cohort (18 years old or younger) of patients with BAVMs referred to a high-volume Chinese neurosurgery center during the past 5 years, we identified periventricular nidus location and smaller nidus size as independent predictors of hemorrhagic presentation. In contrast to adult patients, deep location, exclusively deep venous drainage, and associated aneurysms were not significantly correlated with the appearance of hemorrhage in these children. A recent study of the Columbia pediatric BAVM cohort (of 81 children) identified deep venous drainage, rather than exclusively deep venous drainage, as a predictor for hemorrhage presentation.28 Another report on 135 children with BAVMs indicated the presence of an association of exclusively deep venous drainage with hemorrhage.25 The role of exclusively deep venous drainage should be analyzed in further studies with larger sample sizes by using standard angiographic methods, because only 9.3% of children with BAVMs had exclusively deep venous drainage in our study, which is much less than the 17%–28% rate reported in other studies.7 The presence of an associated aneurysm and deep nidus location has failed to correlate with BAVM hemorrhage in all previous pediatric studies, and our data corroborate these findings.24⇓⇓–27
Periventricular Nidus with Higher Hemorrhage Risk and More Severe Presentation
More than one-third (34%–37%) of BAVMs in patients of all ages have been found to be periventricular.14,15 Our data showed a higher frequency of periventricular BAVMs in pediatric patients (60.2%). This heterogeneity related to patient age is congruent with another finding that periventricular BAVMs were more likely to present at a young age than nonperiventricular lesions. In previous studies (On-line Table 4), a periventricular location correlated with an increased risk of BAVM hemorrhage.14,15,21,22,29 In general, 70%–90% of periventricular BAVMs presented with hemorrhage initially.14,29 The underlying mechanism may be related to silent intralesional hemorrhage and clot breakdown in CSF, as reported in previous studies.14 Our data partially verified this theory, indicating that periventricular locations were associated with more intraventricular hemorrhages (52.2%). However, periventricular BAVMs were, as expected, more often located deep within the brain, raising the possibility that a deep location and venous drainage might play confounding roles in periventricular BAVM hemorrhages. Nonetheless, the present study in children did not reveal a significantly increased frequency of exclusively deep venous drainage in periventricular BAVMs, and the multivariable analysis indicated that periventricular location was a risk factor for hemorrhage, independent of deep location or venous drainage pattern.
Previous studies have identified some morphologic factors that are significant at presentation but do not necessarily predict future hemorrhages in pediatric patients with BAVMs.24⇓⇓⇓–28 While the long-term follow-up of prospective studies such as A Randomized Trial of Unruptured Brain Arteriovenous Malformations will clarify features that predict future hemorrhage in adults with BAVMs, these studies are less likely to be performed in pediatric patients, a group in which most patients present with hemorrhage; ethical dilemmas could arise during conservative treatment with observation of known BAVMs.30 Assuming that the BAVM had been present since birth, thereby accumulating a large number of patient-years of follow-up, we found an overall annual hemorrhage rate of 5.47% in children with BAVMs, which is much higher than the 2.0% reported in a previous study.6 The annual hemorrhage rate of periventricular BAVMs (6.88%) was almost twice that of nonperiventricular BAVMs. The differences in hemorrhage-free survival between patients with periventricular and nonperiventricular BAVMs were also pronounced. This follow-up approach has been used in many previous studies of BAVMs (On-line Table 5). To consolidate this result, we also reanalyzed the data with an assumption-free follow-up approach (On-line Appendix); this analysis also indicated that periventricular BAVMs had a higher hemorrhage rate (On-line Table 6).
Furthermore, our data indicated a potential association between a periventricular nidus location and a severe clinical presentation after hemorrhage. Further analysis revealed that the poor outcome at presentation of patients with periventricular BAVMs might be associated with deep, large hematomas and acute hydrocephalus. However, <40% of the periventricular BAVMs with unfavorable outcomes presented with hydrocephalus that could be reversed with external ventricular drainage.
Study Limitations
This study was limited by its sample size, single-institutional population, and the assumptions used in the follow-up method. For the BAVM natural history study, the most valid follow-up model is to use the time from diagnosis to an event.8,9,31 However, investigators from our study group and other institutes have also reported the hemorrhage rate on the basis of a follow-up method that assumes that the lesion is present from birth and has a subsequent constant annual hemorrhage risk (On-line Table 5).16,32⇓⇓–35 A recent study comparing the 2 approaches suggested that the latter follow-up method is a valid alternative for a BAVM natural history study.36
Conclusions
Small periventricular BAVMs were associated with an increased hemorrhage risk in pediatric patients. Cautious follow-up of children with untreated periventricular BAVMs is recommended due to the higher hemorrhage risk and the likelihood of severe neurologic outcomes at the time of hemorrhage onset.
Acknowledgments
The authors thank Dr Gu Wei-Bin of the Department of Neuroradiology at Beijing Tiantan Hospital for his assistance with the image analysis; and Dr Wang Chen-Xi of the Department of Surgery, West China School of Medicine, at Sichuan University, and Dr Yuan Lian-Xiong of the Department of Statistics and Epidemiology, School of Public Health, at Sun Yat-Sen University for their assistance with the manuscript preparation and data analysis.
Footnotes
Disclosures: Li Ma—RELATED: Grant: The Ministry of Science and Technology of China, Beijing Institute for Brain Disorders, National Natural Science Foundation of China,* Comments: This project was supported by the Ministry of Science and Technology of China, National Key Technology Research and Development Program (2013BAI09B03); Beijing Institute for Brain Disorders grant (BIBD-PXM2013_014226_07_000084); and the National Natural Science Foundation of China (H0906 81271313 to Y.-L. Zhao). *Money paid to the institution.
This work was supported by the Ministry of Science and Technology of China, National Key Technology Research and Development Program (2013BAI09B03); Beijing Institute for Brain Disorders grant (BIBD-PXM2013_014226_07_000084); and the National Natural Science Foundation of China (H0906 81271313 to Y.-L. Zhao).
Indicates open access to non-subscribers at www.ajnr.org
References
- Received October 20, 2014.
- Accepted after revision December 16, 2014.
- © 2015 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}