
Abstract
SUMMARY: When the cornea of the eye dissolves, most commonly secondary to infection or trauma, the ventral wall of the anterior chamber of the eye is no longer supported and thus bulges forward, enlarging the anterior chamber volume. This is referred to as a corneal melt, and it has a unique CT appearance that has not been previously described.
Acorneal melt is a complete breakdown of the corneal structure, which can be initiated by a variety of conditions most commonly related to infections, prior surgery, systemic or localized autoimmune diseases, or trauma. When a corneal melt occurs, it results in an enlarged anterior chamber of the eye and it has a unique CT morphology, which does not appear to have been previously described, to our knowledge. The purpose of this article is to report 2 cases of corneal melt: 1 related to herpes simplex infection and 1 related to trauma after cataract surgery and a corneal transplant.
Case Reports
Case 1
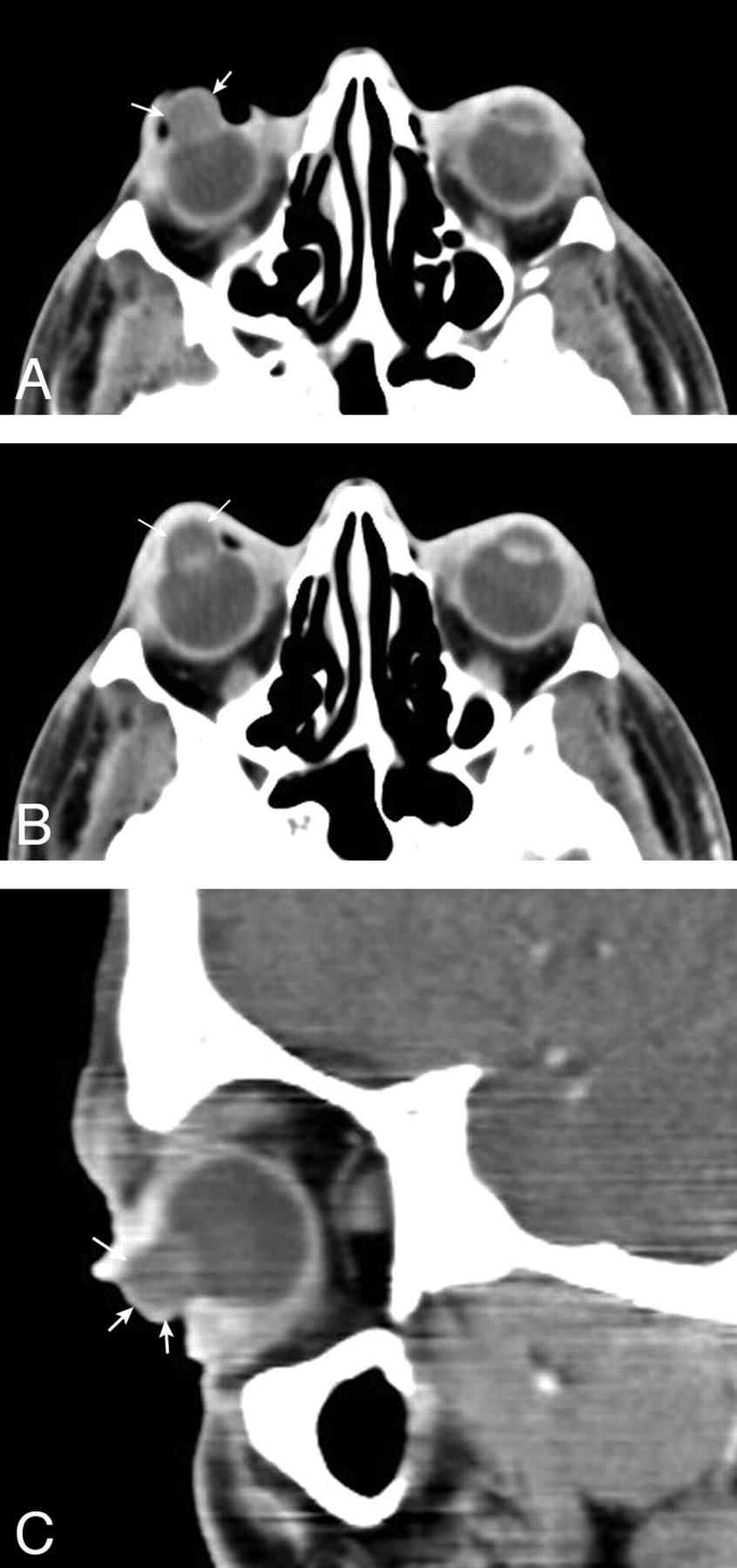
The patient was a 51-year-old man with no significant medical history. His ocular history was significant for herpetic keratitis treated at an outside institution. The patient reportedly had a neurotrophic ulcer secondary to herpetic eye disease, which he said resolved 4 months earlier. Approximately 3 months before his present admission, he noted progressively worsening vision associated with ocular pain. At the time of presentation, he had no light perception in the right eye and was 20/40 in the left eye. He was noted to have a tension of 76 in the affected eye. The anterior segment of the eye was disorganized with opacification, and no corneal layers could be identified. There was no view to the posterior pole. On B-scan sonography, the retina was flat without any significant vitritis. The lens was noted to be thickened and slightly displaced anteriorly. A CT scan of the orbits showed a grossly enlarged anterior chamber in an otherwise unremarkable eye (Fig 1). Five days later, the patient had an enucleation of the right eye.

Serial axial CT scans (A and B) and a sagittal CT scan (C) in patient 1 show a considerably enlarged anterior chamber (arrows) of the right eye. The lens can be seen in a grossly normal position. This patient had a corneal melt.
Case 2
The patient was a 90-year-old woman with a medical history significant for migraines and gait imbalance, and an ocular history significant for bilateral cataract extractions 20 years ago and corneal transplantation in the left eye 9 years ago, with a limbal relaxing incision performed 1 year later for a residual refractive error. On presentation to the emergency department for a fall, she had decreased vision in her left eye, and an examination revealed multiple facial lacerations. Her ophthalmic examination showed a flat anterior chamber with prolapsed uveal tissue. Her CT of the head and orbits showed no evidence of acute orbital fracture. However, there was an enlarged anterior chamber in her left eye (Fig 2). After appropriate antibiotic and tetanus vaccine prophylaxis, she was taken to the operating room where it was found that her corneal transplant wound had dehisced and the intraocular lens placed at the time of cataract surgery had extruded from the eye and was found in the inferior fornix.

Axial (A) and sagittal (B) CT scans in patient 2 show a grossly enlarged anterior chamber (arrows). No lens is seen. This patient had a posttraumatic corneal melt.
Discussion
The corneal epithelium is important in maintaining the health of the corneal surface due to its ability to rapidly duplicate and to repair corneal damage. In addition, progenitor limbal stem cells, which are located at the limbus, can quickly mobilize and migrate to a site of corneal injury.1
The term corneal melt refers to complete disorganization of the cornea, and it usually begins with a defect of the corneal epithelium followed by a failure to re-epithelialize the cornea. This can lead either to a direct infection or to a trophic process, in which proteases and collagenases as well as other immune modulators attack the exposed stroma. This trophic process is compounded by inflammatory cells that result in further ulcerative melting of the cornea.
A corneal melt may be associated with infections, inflammation,2⇓–4 autoimmune diseases, or structural or mechanical abnormalities of the eyelid. The most common causes of corneal melt are herpes simplex virus keratitis5 and retained lenticular material in the postsurgical setting.6
Among all corneal insults, chronic inflammation at the limbus appears to be a common factor for postoperative corneal melting. Conditions that severely damage the limbal stem cells can result in an invasion of conjunctival epithelium onto the corneal surface because the barrier between these surfaces is lost. This invasion results in a thickened irregular unstable epithelium often with secondary neovascularization and inflammatory cell infiltration called “conjunctivalization.”7 Epithelial defects are common in a conjunctivalized corneal surface and may lead to corneal ulceration and melting.
In addition, a cornea stripped of its epithelium is less resistant to normal collagenase-induced cell lysis. This delay in re-epithelialization can favor corneal melting. If the limbal vascular routes are no longer functional because of massive thrombosis, then the integrity of the cornea is threatened and sterile necrosis leading to a melt syndrome may occur.8
Akpek et al9 discovered that the body can launch an attack on cornea-associated antigen, located only in the cornea, which can also lead to corneal melt.
The final common pathway for corneal melt suggests that the corneal tissue is weakened or inflamed around the corneal inserts, and there is evidence of decreased keratocyte attenuation. These findings suggest increased keratocyte apoptosis and tissue digestion.
With the destruction of the cornea, the ventral border of the anterior chamber is no longer supported and it bulges forward, enlarging the anterior chamber. This can occur with or without a lens in place. The now patulous anterior chamber is filled with material of a similar attenuation to the vitreous chamber.
The differential diagnosis for an enlarged anterior chamber includes, in the setting of trauma, hyphema and a posterior ruptured globe,10 with the former causing enlargement of the anterior chamber secondary to hemorrhage (increased attenuation in the anterior chamber (Fig 3), while the latter produces a pseudoenlargement of the anterior chamber secondary to retropulsion of the lens due to leakage of the vitreous fluid (deformed contour of the globe). In addition to a corneal melt, nontraumatic causes of anterior chamber enlargement include a uveal melanoma arising from the ciliary body or the iris,11 an ocular metastasis,12 and congenital glaucoma.13

Axial CT scan in a 54-year-old woman with a high-attenuation enlarged left anterior chamber (arrows). She had a hyphema.
In summary, the uncommon occurrence of a corneal melt has a unique CT appearance that should allow its imaging diagnosis.
References
- Received March 16, 2012.
- Accepted after revision March 25, 2012.
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.