
Fetal goiter is a rare potential cause of airway obstruction and neonatal hypoxic-ischemic brain injury or death.1 MR imaging evaluation of the enlarged gland and airway can provide information crucial to perinatal management. Because the neuroradiologist may be required to apply expertise in MR imaging and in head and neck anatomy to these cases, we describe imaging findings in fetal goiter and discuss fetal MR imaging protocol optimization.
Screening sonography of the 33-week fetus of a woman with Graves disease on propylthiouracil (PTU) therapy revealed a homogeneous 5.3-cm bilobed anterior neck mass suspicious for goiter and mild polyhydramnios. The distal femoral ossification center was not seen, and fetal heart rate was normal. The PTU dose was reduced, and subsequent fetal MR imaging (Fig 1) at 34.5 weeks' gestation demonstrated a T1 hyperintense and T2 low-intensity bilobed anterior neck mass consistent with goiter, slightly decreased in size. The airway was poorly visualized at the level of the oropharynx but was otherwise well-defined to the level of the carina, with ∼1 cm left-to-right midline tracheal shift. Due to potential airway compromise, the ex utero intrapartum treatment procedure was performed during cesarean delivery at 36 weeks to secure the neonatal airway. American Pediatric Gross Assessment Records (APGARs) were 3 at 1 minute and 8 at 5 minutes. Sonography on day 2 of life demonstrated decreasing enlargement of the thyroid with mild hyperemia. By day 3 of life, the patient was extubated and did well on room air, with occasional stridor at 1-month follow-up. Results of thyroid function and hormonal studies remained normal during the first 2 months of life.

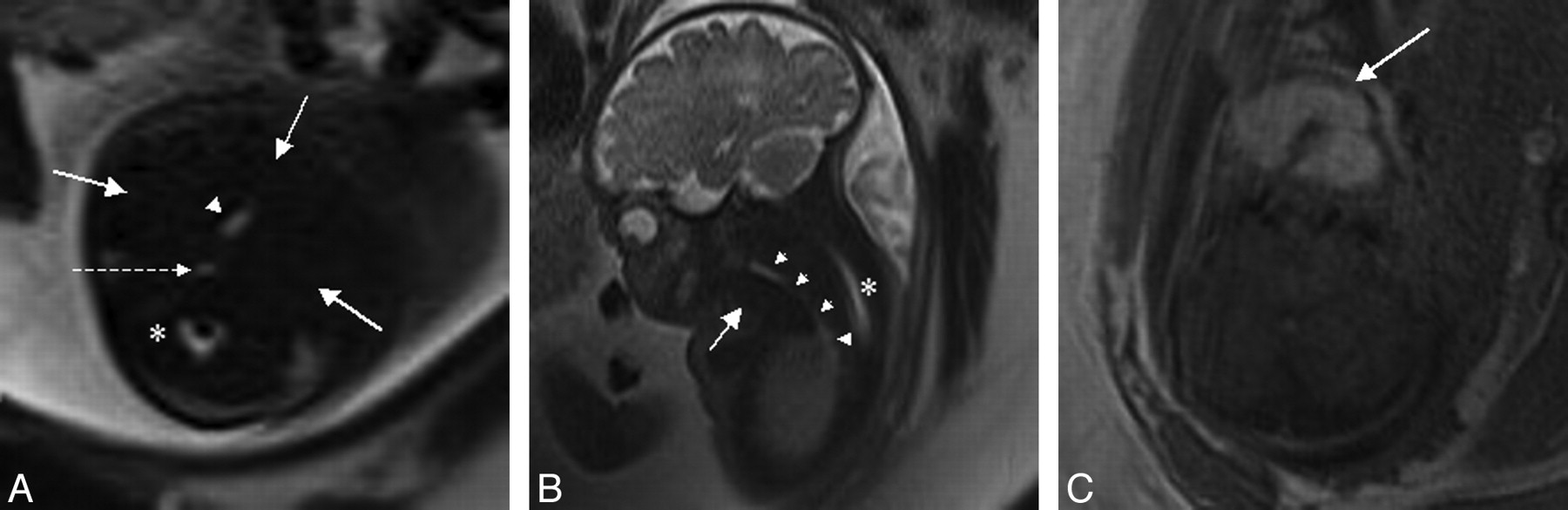
MR imaging of fetal goiter at 34.5 weeks' gestation. A and B, The fluid-filled airway (arrowheads) is well-evaluated on axial (A) and sagittal (B) T2-weighted images to the level of the carina, with poor visualization at the level of the oropharynx. The fluid-filled esophagus (dashed arrow) and spinal canal (asterisk) are also seen. Goitrous fetal thyroid (solid arrows) is isointense to muscle on T2-weighted images, limiting delineation. C, Hyperintensity on T1-weighted images better defines the enlarged fetal thyroid.
Fetal goiter occurs in ∼8% of fetuses of hyperthyroid mothers on antithyroid therapy and manifests as a symmetric homogeneous solid bilobed anterior neck mass on sonography after the fetal thyroid begins to function late in the first trimester.2,3 Depending on the mother's antibody and medication status, the fetus may be hyperthyroid, euthyroid, or hypothyroid. Fetal tachycardia suggests a hyperthyroid state, and hypoplasia of the distal femoral ossification center may indicate hypothyroidism.2
Although neonatal thyroid status generally normalizes within 1 month of birth,3 fetal goiter may result in significant complications at delivery due to airway obstruction, including hypoxic-ischemic brain injury and death.1 Fixed hyperextension of the neck due to mass effect may necessitate cesarean delivery; polyhydramnios due to poor fetal swallowing indicates potential airway obstruction and should prompt MR imaging.2 Although MR imaging may be performed at any time after the first trimester, MR imaging performed closer to delivery will best predict peripartum anatomy. The rapidity of the T2-weighted single-shot fast spin-echo (SS-FSE) acquisition enables imaging of the moving fetus without significant motion degradation and provides excellent delineation of the fluid-filled fetal airway. Although thyroid T2 signal intensity varies with functional status, hypointense if protein and iodine concentration are high and hyperintense if they are low, T1 hyperintensity is more consistent.4 T1-weighted images to better define the thyroid are, therefore, recommended to complement visualization of the airway on standard T2-weighted SS-FSE fetal MR images.
- © 2011 by American Journal of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.