
Abstract
SUMMARY: The mortality of severe sepsis is still high, despite improved treatment modalities. It is known that treatment with DAA reduces mortality in this condition; however, major bleeding may occur as a complication. We present a patient with normal findings on platelet and coagulation tests who developed multiple cerebral hemorrhages after DAA infusion. Patients with septic shock who undergo DAA infusion should be followed closely for possible intracranial bleeding. When intracranial hemorrhage is detected in patients in the intensive care unit, treatment with DAA infusion should be questioned.
Abbreviations
- DAA
- drotrecogin alpha activated
Sepsis remains a common cause of death in intensive care units worldwide and challenges the clinician with a variety of management problems.1 The most important causes of mortality in sepsis are diffuse endovascular damage, coagulopathy, and multiple organ failure.1,2 Early infusion of recombinant human activated protein C (DAA) has been recently reported to reduce mortality in severe sepsis.3
There are only a few preliminary studies that mention the role of DAA (Xigris) in sepsis and complications of this treatment.4–6 These studies revealed that DAA treatment could increase gastrointestinal and intracranial bleeding risk.7 To the best of our knowledge, there is no information about the possible complications of this new treatment technique in the radiology literature. Here we report a patient with severe sepsis treated with DAA, which was complicated by multiple cerebral hemorrhages.
Case Report
A 24-year-old man was admitted to the emergency department with confusion, fever, nausea, and vomiting. The patient had received treatment for chronic otitis media before and had no concomitant disease.
On physical examination in the emergency department, neck stiffness, confusion, tachycardia, and tachypnea were detected. The patient's Glasgow Coma Scale score was 9, and his temperature was normal. Arterial blood gas analysis revealed metabolic acidosis. On the basis of a complete blood count test, leukocytosis was detected. Blood urea nitrogen and creatinine values were high. Cardiac and hepatic enzymes were increased. Non-contrast-enhanced CT was performed, and the findings were normal. Analysis of CSF favored meningitis. The patient was intubated and taken to the intensive care unit, and supporting treatment and antibiotherapy were started. In the 2-hour follow-up period, hypotension increased (75/30 mm Hg). Plasma replacement together with inotropic therapy was started, but there was no response. The Acute Physiology and Chronic Health Evaluation score was 34; and because of the rapid deterioration of his health status, DAA, 24-μg/kg per hour infusion, was introduced and continued for 96 hours. Dexamethazone was given for progressive hypotension, and pentaglobulin was given for septic shock therapy. Due to continuing deep metabolic acidosis, sedation and curarization were performed. Positive mechanical ventilation for lung failure and bedside dialysis for renal failure were performed as well. The patient received platelet and plasma replacement during the dialysis period.
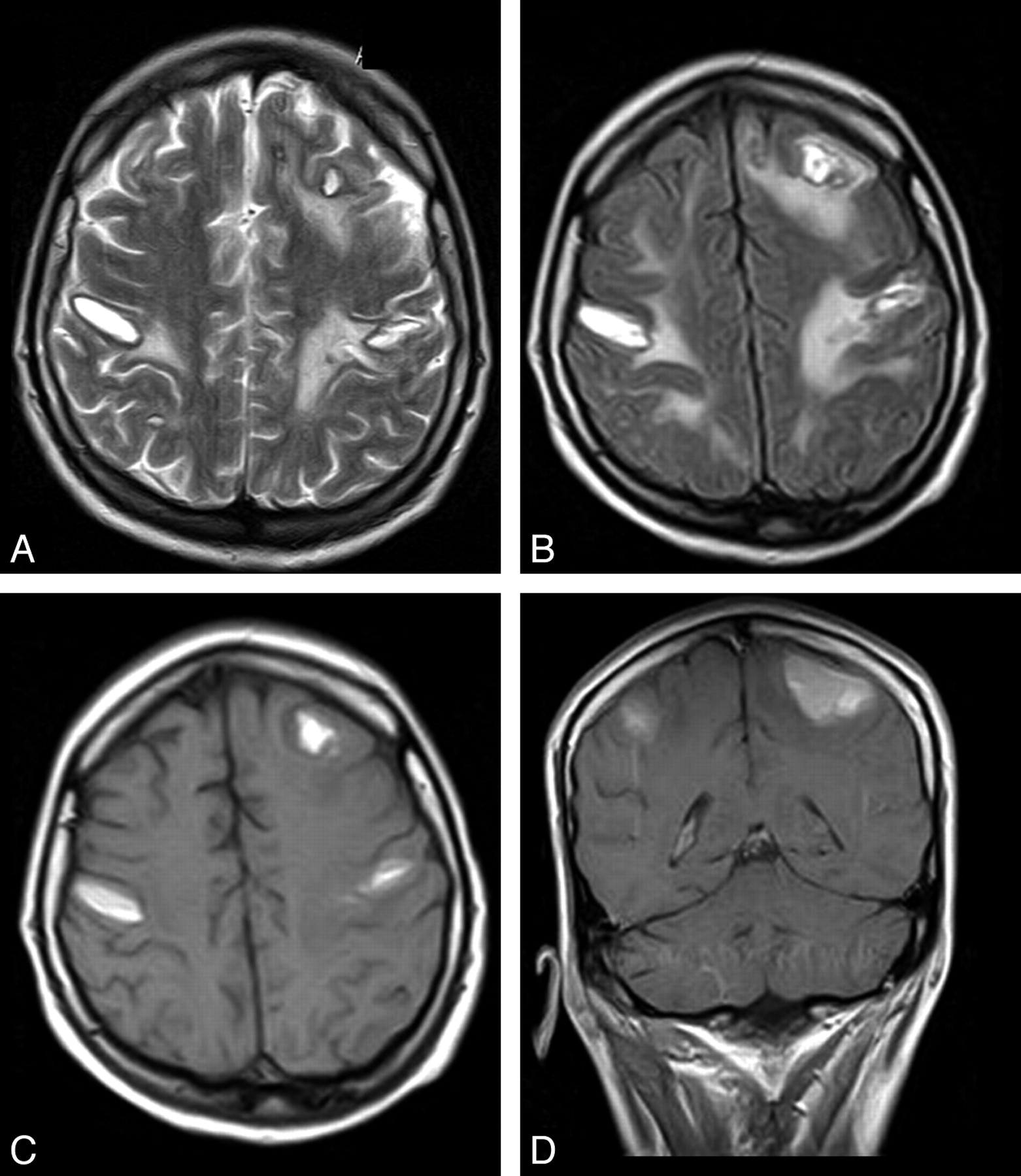
The patient was extubated on the 11th day. On neurologic examination, motor deficit was detected in the bilateral lower extremities; therefore, cranial MR imaging was planned. Multiple cerebral hemorrhages were observed on MR images (Fig 1). Mannitol was given for treatment of cerebral edema, and the patient's neurologic symptoms regressed thereafter. Control cranial MR imaging performed after 3 months revealed almost complete regression in cerebral hemorrhage foci. There was complete healing with no pathologic findings on the physical examination performed at 6 months.

Axial T2-weighted (A), fluid-attenuated inversion recovery (B), T1-weighted (C), and coronal T1-weighted (D) images of the patient. After DAA administration, all images display bilateral multiple cerebral hemorrhages in the gray-white matter junctions.
Discussion
It is assumed that DAA decreases the mortality rate in case of severe sepsis.4–6 The mechanisms of the improved survival with this new drug are not entirely clear.6 DAA could cause serious bleeding due to its anticoagulant and profibrinolytic effects.3 In a recently published study, it is suggested that 3K3A-APC (a nonanticoagulant variant of DAA) has a lower risk for bleeding compared with DAA; however, there is no single clinical study that compares these 2 agents.7 As far as we know, there are 3 reported intracranial bleeding cases due to DAA usage in the general literature.3–6 All 3 patients were reported to have died; however, our patient survived with proper treatment.
To our knowledge, there is no information about the possible complications of DAA treatment in the radiology literature. Knowing the possible complications of DAA is important for the radiologist to make a correct diagnosis in patients who are referred with sepsis and intracranial hemorrhage as the initial diagnosis. One should remember that intracranial bleeding could occur in patients under DAA treatment as in our patient, even though platelet number and bleeding test findings are normal. For early diagnosis and proper treatment, it is important to know whether the patient is under DAA treatment.
Conclusions
When intracranial hemorrhage is detected on a radiologic examination of a patient in the intensive care unit, DAA treatment should be kept in mind for the differential diagnosis. In addition, one should not forget that DAA treatment could cause serious intracranial bleeding, even though all coagulation parameters are in the normal ranges. It is very important to detect the complications of DAA treatment early and to know the radiologic manifestations for planning treatment and reducing mortality.
- Received February 13, 2010.
- Accepted after revision February 17, 2010.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.