
Abstract
BACKGROUND AND PURPOSE: SCD has been reported to involve the inner ear and result in LH and LO. Our purpose was to examine the prevalence of inner ear involvement and to assess the relationship between clinical and imaging findings in patients with SCD.
MATERIALS AND METHODS: Review of our institution's imaging data base for patients with SCD who underwent imaging of the brain or head and neck region or both by CT, MR, or both from 2004 to 2008 was performed. Presenting symptoms, type of SCD, sex, imaging studies performed, and imaging findings were documented.
RESULTS: Among 89 patients with SCD identified (41 males, 48 females), 17 patients (14 males, 3 females; 10–48 years old) underwent imaging evaluation for inner ear complaints, including SNHL, dizziness, vertigo, and tinnitus. LH was identified in 3 patients (3 males) and LO was identified in another 3 patients (2 males, 1 female). All patients with LH had sickle-hemoglobin C disease, whereas those with LO consisted of 2 patients homozygous for HbS (2) and 1 with HbS/β-thalassemia. Patients with LH presented with vestibular symptoms (2 vertigo, 1 dizziness), whereas patients with LO presented with SNHL. LH was seen in the basal turn of cochlea and vestibule, whereas LO involved the lateral semicircular canal.
CONCLUSIONS: LH and LO were found in approximately one-third of patients with SCD with inner ear symptoms and preferentially affected males.
ABBREVIATIONS
- DRIVE
- driven equilibrium radio-frequency pulse sequence
- Hb
- hemoglobin
- HbSC
- sickle-hemoglobin C disease
- LSC
- lateral semicircular canal
- LH
- labyrinthine hemorrhage
- LO
- labyrinthitis ossificans
- PSC
- posterior semicircular canal
- RBC
- red blood cell
- SCD
- sickle cell disease
- SNHL
- sensorineural hearing loss
- SSC
- superior semicircular canal
SCD is an autosomal recessive disease characterized by an abnormal Hb molecule, HbS, that polymerizes when deoxygenated, initiating a complex pathophysiology, that results in vaso-occlusion and hemolytic anemia.1,2 The spectrum of clinical manifestations is broad and can involve virtually any organ system, including inner ear.3 SNHL is a well-recognized complication of SCD.4⇓⇓⇓⇓⇓⇓–11
LH and LO have been reported to affect the inner ear in SCD; however, the association between inner ear involvement and imaging findings has not been fully described. Our purpose was to examine the prevalence of inner ear involvement of LH and LO and to assess the relationship between clinical and imaging findings of LH and LO in SCD.
Materials and Methods
Following our institutional review board approval, a retrospective review of our imaging data base was performed to identify patients with SCD who underwent imaging of the brain or head and neck region or both by CT, MR, or both between January 1, 2004, and December 31, 2008.
Each identified patient's clinical chart was reviewed. Data regarding age, sex, Hb phenotype, past medical history, and initial presenting symptoms prompting imaging examinations were collected and recorded. Given that LH is known to occur as a complication of bleeding disorders, the most common being leukemia,4 and that LO can result from suppurative bacterial or viral labyrinthitis, advanced otosclerosis, trauma, autoimmune inner ear disease, and tumors of the temporal bone,12 patients were excluded if they had a past medical history of these conditions.
All patients were scanned with a 16 or 64 multidetector CT (LightSpeed or VCT; G.E., Milwaukee, Wisconsin) and/or a 1.5T MR imaging scanner (Achieva or Intera; Philips Medical Systems, Cleveland, Ohio), with or without intravenous contrast media. High-resolution CT of the temporal bone was performed with 1.25- or 0.625-mm contiguous axial images reviewed with 1-mm coronal recontructions. Temporal bone MR imaging consistently included axial and coronal T1-weighted spin-echo sequences (3.0-mm section thickness with 0.3-mm intersection gap) and an axial T2-weighted DRIVE sequence (1.4-mm-thick sections with 0.7-mm interval reconstruction).
The CT and MR imaging performed were re-reviewed by 2 neuroradiologists who where blinded to initial formal radiologic interpretation for the presence of the inner ear abnormalities (LH and LO) and their sites of involvement. Any discrepancies were resolved by consensus.
Results
Review of our imaging data base revealed 89 patients with SCD (41 males, 48 females; age, 1–53 years). Of these 89 patients with SCD identified, 17 patients (14 males, 3 females; age, 10–48 years) presented with inner ear symptoms and were evaluated by imaging of the brain or head and neck region or both. Presenting symptoms included SNHL (6 patients), dizziness,6 vertigo,5 and tinnitus,3 or combination of multiple symptoms.
Eleven temporal bone MR, 1 temporal bone CT, 17 brain MR, and 4 brain CT (including 1 CT angiogram) imaging examinations were performed in the work-up of these complaints. Of 11 patients who were evaluated by dedicated temporal bone MR imaging, CT, or both, LH was identified in 3 patients and LO was identified in another 3 patients. No temporal bone imaging abnormalities were found in the remaining 5 patients. There were no clinically relevant abnormalities that might explain presenting symptoms on the routine brain CT imaging studies and MR imaging studies performed, though these were not performed as dedicated skull base imaging studies.
The demographic information for these patients with LH and LO is given in Table 1. Patients with LH (3 males; 13–18 years old) had HbSC and presented with vestibular symptoms, including dizziness (1) and vertigo (2). All patients with LH complained of headache and ear pain as well. One patient complained of SNHL 1 week after the initial onset. Patients with LO (2 males, 1 female; 12–26 years old) presented with SNHL and had sickle cell anemia or (2) or HbS/β-thalassemia (1).
Clinical details of the patients with LH and LO
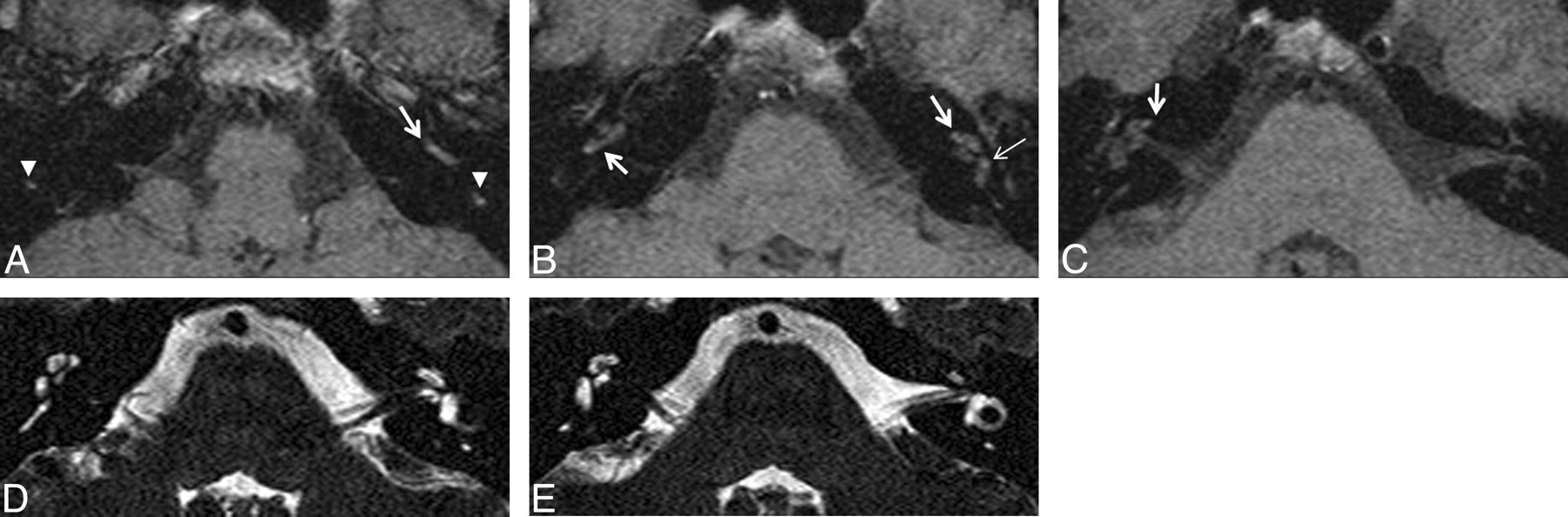
The imaging findings for the patients with LH and LO are listed in Table 2. On T1-weighted temporal bone MR imaging, high signal intensity in the inner ear structure was a characteristic finding for LH (Fig 1). Postcontrast-enhanced T1-weighted imaging did not show any abnormal enhancement, and T2-weighted imaging did not demonstrate any abnormality in the inner ear. LH was always seen in the basal turn of the cochlea and vestibule with bilateral (1/3) or unilateral (2/3) involvement. In 1 patient, the posterior semicircular canals also were involved bilaterally.
Imaging findings of the patients with LH and LO

LH (patient 1). An 18-year-old man (HbSC) presented with dizziness. He also complained of headache and ear pain. A–C, Axial unenhanced T1-weighted MR imaging demonstrates high signal intensity areas in the bilateral basal and middle turns of the cochlea (arrows), PSCs (arrowheads), and left vestibule (thin arrow). D and E, Axial T2-weighted DRIVE MR imaging shows no abnormal signal intensity is in these regions. Postcontrast-enhanced T1-weighted MR image demonstrated no abnormal enhancement (not shown).
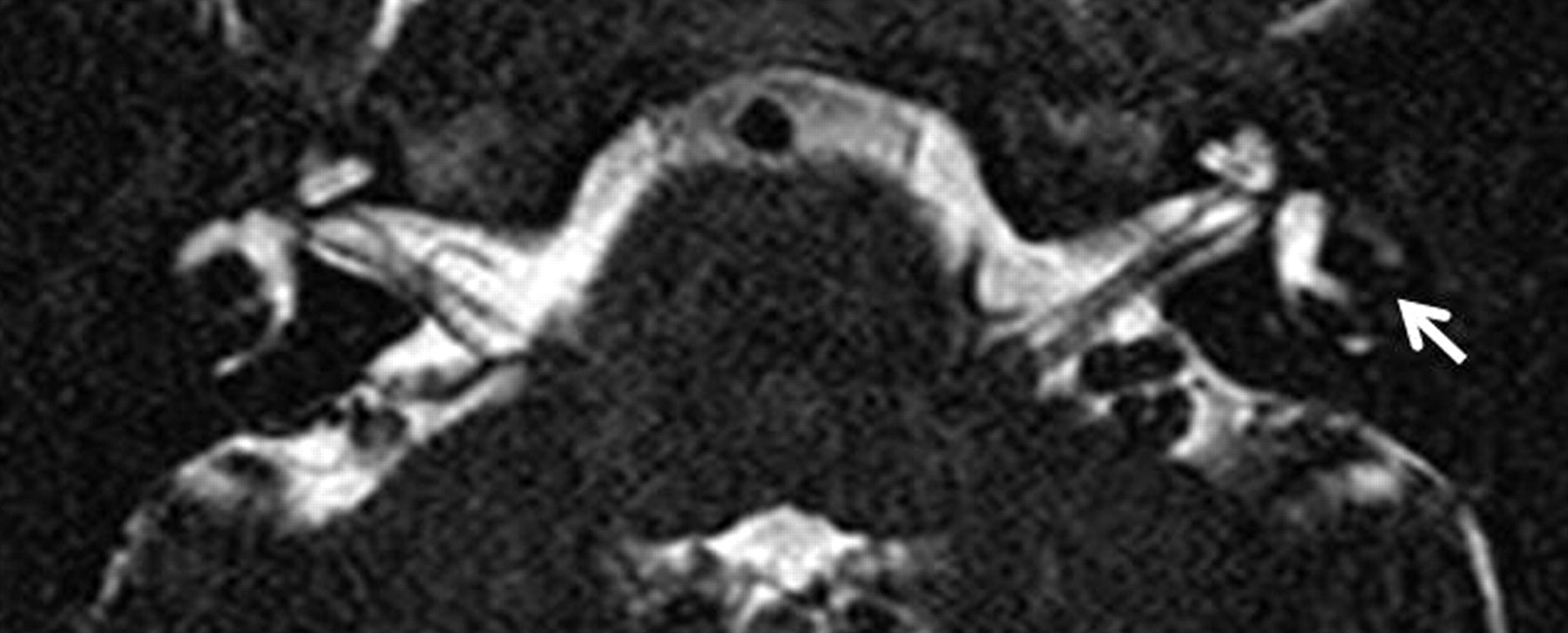
In patients with LO, on high-resolution T2-weighted DRIVE images, the normal T2 hyperintensity in the inner ear was lost (Fig 2). High-resolution temporal bone CT showed ossification of the membranous labyrinth (Fig 3). LO was always seen in the LSC with bilateral (2/3) and unilateral (1/3) involvement. In 1 patient, bilateral apical and middle turns of the cochlea and unilateral basal turn of the cochlea and the vestibule also were involved (1/3). Two patients with LO were scanned for their clinical follow-up evaluation, and we reviewed their initial studies (patients 5 and 6). Both showed progression to bilateral involvement consistent with worsening of bilateral hearing loss.

LO (patient 4). A 26-year-old man (HbS/β-thal) presented with tinnitus and left SNHL. Axial high-resolution T2-weighted DRIVE MR image demonstrates loss of the normal high signal intensity in the left LSC (arrow).

LO (patient 5). A 12-year-old boy (HbSS) presented with bilateral SNHL. A–C, Axial high-resolution temporal bone images from CT angiography demonstrate partial obliteration of the bilateral apical and middle turns of the cochleas and right basal turn of the cochlea (arrows), vestibule (arrowhead), and LSC (thin arrow).
Discussion
SCD is an autosomal recessive disease characterized by abnormal Hb. A single gene defect that is a point mutation at the sixth codon in the β globin gene (the short arm of chromosome 11) results in a single amino acid substitution (valine for glutamic acid) and abnormal Hb structure (HbS).1⇓–3 When a patient possesses 2 sickle cell hemoglobin genes (HbSS), SCD results; a heterozygote patient (with 1 normal and 1 sickle cell β globin chain) is designated HbSA and carries the sickle cell trait. The term SCD applies to all patients with at least a single HbS chain and 1 other abnormal β globin chain, which may be another sickle cell β chain (in which case the patient is homozygous HbSS and by definition has sickle cell anemia), HbC (HbSC), or 1 of the thalassemias (HbS/β-thalassemia).1,2
The spectrum of clinical manifestations of SCD is broad and can involve virtually any organ system. Pathologic changes of SCD are based on the 3 mechanisms: vaso-occlusion, chronic hemolytic anemia, and infection.1⇓–3 The most accepted pathogenesis of inner ear involvement is recurrent vaso-occlusion of the labyrinthine blood vessels, which can result in LH and LO.3⇓⇓⇓⇓⇓–9 LH is thought to result from altered capillary hemodynamics or reperfusion injury.9 The association between LH and LO has not been fully demonstrated, but it is theorized that LH incites a reparative response that cascades from fibrosis to sclerosis and ultimately ossification of the inner ear structures.13
SNHL is a well-recognized complication of SCD, and many previous studies reported high prevalence of SNHL.4⇓⇓⇓⇓⇓⇓–11 LH and LO are known conditions affecting the inner ear in patients with SCD.3,4,9 To our knowledge, the prevalence of inner ear involvement and the relationship between clinical and imaging findings in patients with SCD have not yet been reported.
In this investigation, 19.1% (17/89) of patients with SCD presented with inner ear symptoms and were evaluated by CT, MR imaging, or both during a 5-year period. Vestibular symptoms were most commonly seen, followed by SNHL. We identified 3 patients with LH and 3 other patients with LO. Of the patients evaluated by dedicated temporal bone imaging, 27.8% (3/11) of the patients with vestibular symptoms showed LH, and 50% (3/6) of the patients with sensorineural symptoms showed LO. LH and LO had similar rates of incidence and shared a male sex predominance; however, they presented with different symptoms. Regarding other initial symptoms, all patients with LH complained additionally of headache and ear pain.
LH seems to occur in HbSC predominantly. In the few cases of LH in patients with SCD that have been reported in the literature, patients were noted to have HbSC.4 HbSC comprises approximately 25% of all patients with SCD.1,2 Proliferative retinopathy is more prevalent in HbSC than in sickle cell anemia.14 Perhaps blood viscosity-related factors are important in LH because they are felt to be in HbSC disease with proliferative retinopathy.14 LO, by contrast, based on our observations, seems to be more prevalent among patients with sickle cell anemia. Patients with sickle cell anemia, the most severe type, may have more vaso-occlusive episodes in the inner ear structures and therefore a higher probability of acquiring LO. It is certainly difficult to make definitive conclusions of the pathophysiology of these entities, however, especially considering that LO may result from LH in some cases.
High signal intensity on unenhanced high resolution T1-weighted images is a characteristic finding for LH.3,4,13,15 Loss of water signal intensity in high resolution T2-weighted images (eg, DRIVE, constructive interference in the steady state) also is reported for LH;15 however, we did not detect abnormality on high-resolution T2-weighted images. Contrast-enhanced TI-weighted imaging can exclude tumors such as schwannomas and hemangiomas that show intense and localized enhancement. The characteristic imaging finding of LO is ossification of the membranous labyrinth on high resolution CT. On high resolution T2-weighted imaging, the normal T2 hyperintensity in the labyrinth is lost.3,9,12,16⇓⇓⇓–20 There was no LO case with gadolinium enhanced MR imaging in our study. Postcontrast-enhanced characteristics of LO has not been described well in the literature.3,9,16⇓⇓⇓–20 The enhancing labyrinth occurs most commonly in the acute and subacute stage of labyrinthitis due to accumulation of gadolinium within inflamed labyrinthine membrane. LO is the end-stage of labyrinthitis and characterized pathologically by proliferation of fibroblasts and finally osteoblasts. Therefore, LO may show faint or no enhancement in the labyrinth.
We observed that both LH and LO had a predilection for particular structures in the inner ear. LH was always identified in the basal turn of cochlea and vestibule, whereas LO was identified in LSC. The inner ear involvement is considered to result from vaso-occlusion of the labyrinthine blood vessels in SCD.3⇓⇓⇓⇓⇓–9 The membranous labyrinth is supplied by the labyrinthine artery that either arises from the anterior inferior cerebellar artery or as a direct branch of the basilar artery. The labyrinthine artery divides into the anterior vestibular, vestibulocochlear, and the proper cochlear arteries.21 The anterior vestibular artery provides the blood supply to most of the utricule and the superior and horizontal ampullae, as well as a small portion of the sacculus. The vestibulocochlear artery further divides into a cochlear ramus and a vestibular ramus, also known as the posterior vestibular artery. The posterior vestibular artery is the source of the blood supply to the posterior ampulla, the major part of the saccule.21 It is possible that LH and LO might result from vaso-occlusion from different vascular branches; however, the number of positive patients in this study is too small to confirm this postulation.
There have been numerous case reports of LO caused by other etiologies, such as meningitis, labyrinthitis, and trauma.12,16⇓⇓⇓–20 In postmeningitic LO, the most common location has been reported to be the scala tympani of the basal turn of cochlea due to the route of inflammation spread through the cochlear aqueduct.16⇓⇓⇓–20 The LSC also is reported to be affected frequently in the patients with more advanced ossification.18 The difference between LO in SCD and LO secondary to other etiologies may be the initially affected location.
Bilateral inner ear involvement was observed in 1 patient with LH and in 2 patients with LO. Two patients with LO were scanned for their clinical follow-up evaluation, and both showed progression to bilateral involvement consistent with clinical findings. In postmeningitic LO, the inner ear is sometimes affected bilaterally due to the spread of the infection by CSF.16⇓⇓⇓–20 Given that vaso-occlusion in patients with SCD can occur within any organ and that the labyrinthine artery has a higher chance of vaso-occlusion given the small caliber of this vessel, the observation of bilateral involvement by LO in patients with SCD is not surprising.
Comparing the efficacy of CT versus MR imaging for diagnosing inner ear disease in patients with SCD is difficult based on this retrospective study because of the small number of positive cases. One patient with LO (patient 5) underwent temporal bone CT and MR imaging, and the imaging findings are listed in the Table 2. In this case, MR imaging detected LO more clearly than CT especially in the semicircular canals. One study has shown a much higher sensitivity of MR imaging in detecting cochlear obstruction,19 whereas another study has reported no significant difference in the sensitivity and specificity of MR imaging and CT with respect to LO.22 Although it is well-known that T2-weighted imaging can be falsely positive in detecting abnormalities, thin-section unenhanced T1-weighted images demonstrate LH effectively.4 Therefore, we suggest that dedicated temporal bone MR imaging, including T1-weighted (≤3-mm section thickness) and T2-weighted sequences (≤1–2-mm section thickness), should be the first imaging study for the evaluation of inner ear complaints in patients with SCD. Temporal bone CT should be done when there is a discrepancy between the clinical findings and MR imaging.
Several limitations are present in this study. First, diagnosis of LH was made on the basis of imaging findings and clinical presentation, without histopathologic confirmation. However, obtaining tissue for imaging confirmation would not be ethically appropriate. Despite this limitation, we believe that T1-weighted images can reliably distinguish tumors, pus, or fat in the labyrinth; clinical parameters were used in distinguishing T1 hyperintense blood from pus in patients we diagnosed with LH. Second, this is a retrospective study and patients were selected on the basis of an electronic data base review. Some patients with inner ear symptoms may not have had any imaging evaluations and would not have been identified on our initial imaging data base review. Furthermore, in this retrospective study, not all patients were evaluated by dedicated temporal bone imaging, though since 2007, all patients with SCD at our institution are evaluated with both brain and temporal bone MR imaging to assess for the presence of brain and head and neck involvement. It is possible that inner ear abnormalities were present on routine imaging studies included in this investigation but were not detectable due to the routine (nonhigh-resolution) technique used. Furthermore, it is possible that the number of patients with LO was underestimated due to the small number of temporal bone CT examinations performed. Third, because our institution is a major referral center for patients with SCD, our patient population with SCD may be skewed toward more severely affected patients than other imaging centers. A final limitation of our study is the small number of positive cases due to the relatively rare presenting complaint of inner ear symptoms in this specific patient population.
Conclusions
LH and LO are not uncommon among symptomatic patients with SCD and were found in approximately one-third of patients with SCD with inner ear symptoms and males were preferentially affected. In patients with SCD presenting with inner ear complaints, dedicated temporal bone imaging should be performed, preferably by MR imaging.
Footnotes
-
Paper previously presented at: Annual Meeting of the American Society of Neuroradiology, May 15–20, 2010; Boston, Massachusetts. The title was “Inner Ear Imaging Findings in Patients with Sickle Cell Disease” (presentation 210).
References
- Received February 20, 2011.
- Accepted after revision April 28, 2011.
- © 2011 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}