
Abstract
BACKGROUND AND PURPOSE: Neurological manifestations, such as benign convulsions and encephalitis/encephalopathy have been reported in patients with rotavirus gastroenteritis. However, cerebellitis has not attracted much attention. The purpose of this study was to identify and report the clinical and radiologic features of rotavirus cerebellitis.
MATERIALS AND METHODS: Records of patients with rotavirus gastroenteritis exhibiting cerebellar lesions on MR imaging were collected from multiple centers in Japan. Their clinical, laboratory, and radiologic data were reviewed retrospectively.
RESULTS: A diagnosis of acute cerebellitis concurrent with encephalitis was made for 11 of 13 patients identified. Two patients who were diagnosed as having injury due to hypovolemic shock were excluded from the study. All 11 patients with acute cerebellitis had disorders of consciousness with onset on days 2 to 4, followed by mutism in 10 patients. Other cerebellar symptoms included dysarthria following the mutism, hypotonia, ataxia, tremor, nystagmus, and dysmetria. MR imaging lesions in the vermis or cerebellar cortex were seen at some point (day 5 to 1 year) in 10 patients. A reversible splenial lesion (3 isolated and 3 with concurrent cerebellar lesions) was found in 6 patients scanned between days 4 and 6. Transient lesions in the cerebellar white matter/nuclei manifesting reduced diffusion were seen in 6 patients during days 5 through 7. The final MR imaging performed after 1 month showed cerebellar atrophy in 10 patients.
CONCLUSIONS: The 11 patients with rotavirus cerebellitis exhibited nearly identical clinical and MR imaging features. Involvement of the cerebellar white matter/nuclei may be associated with the mutism. An isolated splenial lesion with homogeneously reduced diffusion is not always a benign sign indicative of complete clinical and radiologic recovery in patients with rotavirus gastroenteritis.
Abbreviations
- A
- ataxia
- AESD
- acute encephalopathy with biphasic seizures and late reduced diffusion
- ANE
- acute necrotizing encephalopathy
- C
- consciousness disturbance
- CC
- corpus callosum
- CNS
- central nervous system
- D
- day
- Dy
- dysarthria
- EEG
- electroencephalogram
- FLAIR
- fluid-attenuated inversion recovery
- G
- gray matter
- H
- hypotonia
- MeR
- mental retardation
- MERS
- clinically mild encephalitis/encephalopathy with a reversible splenial lesion
- Mu
- mutism
- Ny
- nystagmus
- N
- cerebellar nucleus
- PCR
- polymerase chain reaction
- Pt
- patient
- S
- seizures
- T
- tremor
- V
- vermis
- W
- white matter
Rotavirus is one of the most common pathogens causing gastroenteritis among children. Neurologic manifestations, ranging from benign convulsions with gastroenteritis to lethal encephalitis or encephalopathy, occur in approximately 2%–5% of patients with rotavirus gastroenteritis.1,2 In addition, rotavirus is reported to be a causative pathogen for MERS,3–5 ANE,6 and AESD3 in Japanese children. Cerebellar involvement in rotavirus gastroenteritis has not attracted much attention, having been reported in few patients.2,7 Our experience with several affected patients stimulated our curiosity about this disorder and instigated this study to determine the clinical and radiologic features of rotavirus cerebellitis.
Materials and Methods
Clinical and radiologic information of patients with rotavirus gastroenteritis exhibiting cerebellar lesions on MR imaging was collected retrospectively by sending out a questionnaire to the members of the Annual Zao Conference on Pediatric Neurology after approval by the institutional review board of the Kameda Medical Center. We reviewed MR images and charts of these patients, including information about symptoms, clinical diagnosis, medication, treatments, outcomes, and results of CSF analysis and EEG. The diagnosis of acute cerebellitis was defined as acute or subacute onset of cerebellar symptoms as well as nausea, headache, and altered mental status, following infection, with cerebellar involvement on MR imaging.8
Results
Thirteen patients were identified with rotavirus gastroenteritis and cerebellar lesions on MR imaging. A diagnosis of acute cerebellitis concurrent with encephalitis was made for 11 of the 13 patients (patients 1–11); the other 2 patients were excluded from this study because they were diagnosed with cerebral and cerebellar injury due to severe dehydration and consequent hypotension. A stool sample was positive for rotavirus antigen in 10 of the 11 patients with cerebellitis, and 1 patient (patient 5) had a clinical diagnosis based on clinical presentation in the setting of a rotavirus gastroenteritis epidemic. No patient with a clinicoradiologic diagnosis of ANE or AESD associated with rotavirus gastroenteritis was identified. The clinical records and radiologic examination results of the 11 patients are summarized in the Table. The 11 patients (3 male and 8 female, from 2 to 4 years of age) developed normally until the onset of neurologic symptoms, except for patient 5 who had a history of febrile seizures. All 11 patients exhibited clinical symptoms of gastroenteritis (fever, diarrhea, and vomiting) on day 1, before the onset of neurologic manifestations.
Clinical and radiologic findings of rotavirus cerebellitis
The 11 patients with acute cerebellitis had disorders of consciousness as the initial neurologic symptom (Table); the onset was on days 2 to 4. After their consciousness cleared on days 4 to 12, mutism became apparent in all patients except 1 (patient 10) within a duration of 4–20 days. Other cerebellar symptoms were seen in all and included slow speech or dysarthria following the mutism, hypotonia, ataxia, tremor, nystagmus, and dysmetria. Only 3 patients (patients 2, 3, and 6) had seizures. CSF analysis revealed pleocytosis (cell count, >10/mL) in 9 of the 11 patients but normal glucose and protein levels. EEG showed slow basic activity in 8 of the 11 patients. Treatments were variable and included corticosteroids in 10 patients and intravenous immunoglobulin administration in 5 patients. The outcome in the 11 patients varied; patients 8 and 10 were nearly healthy, while the other 9 had mild cerebellar symptoms (Table).
Initial MR imaging between days 4 and 6 revealed a splenial lesion with homogeneously reduced diffusion (Figs 1 A, -B and 2A) in 6 of the 11 patients; this finding completely disappeared at the time of the follow-up studies (Figs 1C and 2C). Three of the 6 patients had an isolated splenial lesion (patients 1–3); the other 3 had concurrent cerebellar lesions. The location and time course of the cerebellar lesions on MR imaging are shown in the Table. MR imaging revealed transient lesions with reduced diffusion in the cerebellar white matter/nuclei in 6 patients during the acute stage of the illness between days 5 and 7 (Fig 1D, -E); these disappeared on the follow-up MR imaging with an interval of 3–9 days. In contrast, lesions in the vermis or cerebellar cortex were seen in the acute-to-chronic stages (day 5 to 1 year) in 10 of the 11 patients (Figs 1E and 2D, -E). Reduced diffusion in the cerebellar cortical lesions was only observed in 2 patients scanned on day 5 (patients 4 and 9). No MR imaging in the acute stage showed severe cerebellar swelling that compressed the brain stem or caused tonsillar herniation, as is typically described in acute cerebellitis. The final MR imaging, performed >1 month after presentation, showed high signal intensity in the cerebellar cortex in 4 patients (patients 2, 3, 5, and 9) and cerebellar atrophy in 10 patients (Fig 2E) (it was sometimes difficult to detect cerebellar cortical T2 prolongation due to partial volume effect of CSF) (Fig 1F); the cerebellum was almost completely normal in 1 patient (patient 10). Those lesions found to have reduced diffusion (decreased apparent diffusion coefficient) in the cerebellar nuclei, cerebellar white matter, cerebellar cortex, and corpus callosum are identified by a footnote in the Table.

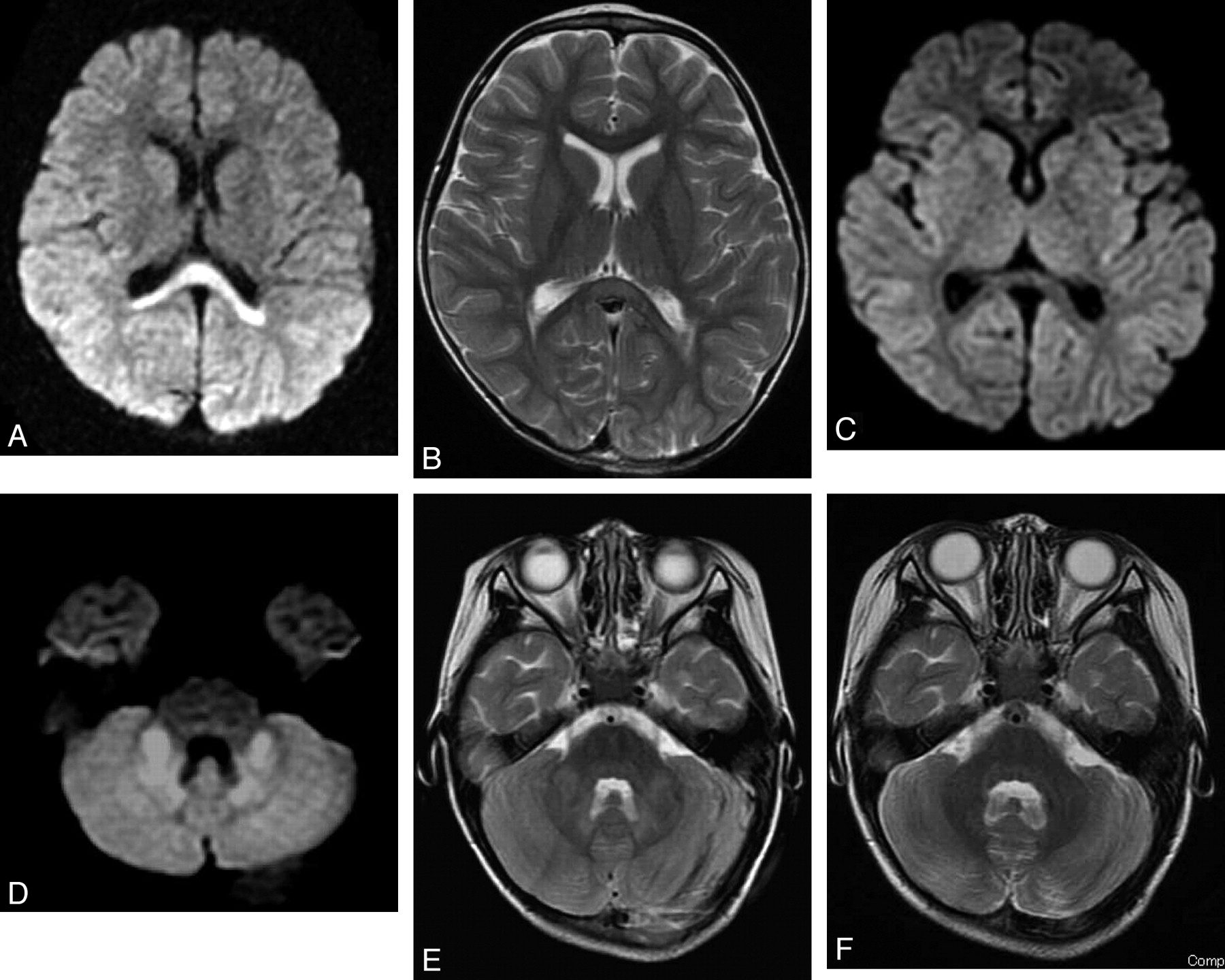
MR imaging of patient 1 on day 4 (A and B), day 6 (C−E), and day 65 (F). A and B, Axial diffusion-weighted image on day 4 (A) shows a high-signal-intensity lesion in the splenium of the corpus callosum with mild high signal intensity on the T2-weighted image (B). C, The splenial diffusion abnormality has disappeared on day 6. D, Diffusion-weighted image on day 6 shows abnormally reduced diffusion in the bilateral middle cerebellar peduncles and cerebellar nuclei. E, T2-weighted image shows mild hyperintensity in the cerebellar cortex, in addition to the middle cerebellar peduncle and nuclear lesions seen in D. F, MR imaging on day 65 shows an almost normal cerebellum other than mild atrophy.

MR imaging of patient 2 on days 6 (A and B) and 13 (C and D) and 1 month (E). A and B, Axial diffusion-weighted images on day 6 show reduced diffusion in the splenium of the corpus callosum with a normal-appearing cerebellum. C and D, FLAIR image on day 13 shows no splenial lesion, but high signal intensity in the cerebellar cortex (arrow). E, FLAIR image through the cerebellum at 1 month shows the development of atrophy.
Discussion
The most important finding in this series is that the clinical and radiologic features of the 11 patients with rotavirus cerebellitis were similar—consciousness disturbance after gastroenteric symptoms of fever, vomiting, and diarrhea, followed by mutism (10 of the 11 patients). MR imaging revealed a reversible splenial lesion in the acute stage, abnormal signal intensity in the cerebellar white matter/nuclei in the acute-to-subacute stages, followed by increased signal intensity in the cerebellar cortex and finally cerebellar atrophy.
Acute cerebellitis is considered an inflammatory syndrome and is clinically defined as fever, nausea, headache, and an altered mental status in conjunction with acute onset of cerebellar symptoms.8,9 Although pathologic investigation has been restricted to critically ill patients, it has been suggested that direct invasion by an etiologic pathogen is the main mechanism.8,10 Inflammatory swelling of the cerebellum is apt to compress the brain stem and may induce alterations of consciousness, which can mask the initial stage of cerebellar symptoms.8 This mechanism was, however, unlikely in our patients with rotavirus cerebellitis because severe cerebellar swelling was not seen in the acute phase; instead, the disease seemed to progress from cerebellar white matter/nuclear involvement to cerebellar cortical involvement. EEG revealed slow basic activity, and MR imaging showed a reversible splenial lesion in 8 and 6 of the 11 patients, respectively, suggesting that concurrent encephalitis may have been the cause of the disturbance of consciousness. Thus, we believe the more correct diagnosis was acute rotavirus cerebellitis concurrent with encephalitis.
Mutism with subsequent dysarthria following a disturbance of consciousness is the most interesting clinical finding in this series. Cerebellar mutism is most commonly described after cerebellar surgery in children; it is typically reversible within days to months, with recovery proceeding through a stage of ataxic dysarthria.11–13 It has been postulated that this mutism may represent an extreme form of dysarthria or anarthria, resulting from impaired coordination of the articulatory muscles due to the cerebellar injury.11,12
Severe speech disturbances, such as mutism, are unusual clinical symptoms in acute cerebellitis in children13; only 6 such patients have been reported.2,7,13–15 Two of those 6 patients were diagnosed as having rotavirus cerebellitis,2,7 and another one, as having cerebellitis following acute gastroenteritis due to an unknown pathogen (with no findings on rotavirus examination).12 On the basis of the present series and previously reported patients, it is reasonable to postulate that rotavirus cerebellitis has distinct clinical features, being characterized by disturbance of consciousness a few days after gastroenteric symptoms, followed by cerebellar mutism. Pediatric neurologists should be aware of this clinical sequence for prompt diagnosis and management of such patients
In 6 of our 11 patients with rotavirus cerebellitis, MR imaging revealed transient lesions in the cerebellar white matter/nuclei with reduced diffusion between days 5 and 7. These lesions disappeared afterward, being followed in some patients by T2/FLAIR hyperintensity in the cerebellar cortex and, finally, cerebellar atrophy. Other reports of acute cerebellitis describe edema of the cerebellar cortex, usually bilateral, followed by cerebellar atrophy,2,8,13,14 rather than involvement of the cerebellar white matter or nuclei. Even the prior reports of MR imaging in patients with rotavirus cerebellitis2 have not described white matter or nuclear involvement; however, those MR imaging studies were performed in the chronic stage of the illness (days 29 and 180), which may explain why the earlier deep lesions were not seen. Stereotactic ablation of the dentate nucleus and superior cerebellar peduncle has been reported to cause reversible mutism, as has trauma to the dentate nucleus and/or its outflow tract.9,16,17 These findings suggest that bilateral involvement of the dentatorubrothalamic tract from the dentate nucleus to the brain stem may cause transient cerebellar mutism. It is, therefore, possible that the lesions in the cerebellar white matter/nuclei observed on MR imaging in the present series may be the cause of their cerebellar mutism. It is not clear why the lesions in the cerebellar white matter/nuclei (seen between days 5 and 7) disappear by the time mutism is observed. It is possible that the mutism is masked by the disturbance of consciousness (encephalitis) in the acute stage and that the functional abnormalities, perhaps biochemical in nature, last longer than the imaging abnormalities.
The pathophysiology of CNS involvement in patients with rotavirus gastroenteritis is not fully understood. It is often explained as direct CNS invasion by the rotavirus.2 Supporting this explanation, rotavirus ribonucleic acid or antigen has been detected in the blood and CSF of patients with rotavirus gastroenteritis, with or without neurologic manifestations,1,2,18 and extraintestinal rotavirus replication has been detected in mice.19 However, neither rotavirus antigen nor PCR of the CSF is always positive in patients with the encephalitis/encephalopathy that is associated with rotavirus gastroenteritis; rotavirus PCR was positive in only 3 of 8 patients reported by Nagatomi and Nakagomi20 and in neither of the 2 patients so examined in the present series (patients 1 and 2).
It is not clear how rotavirus would affect the CNS without direct invasion. Rotavirus could damage enterocytes through toxinlike activity, such as viral nonstructural protein 4.21 Nonstructural protein 4 alone or with rotavirus infection induces nitric oxide metabolites, which are highly reactive free radicals. Serum and CSF nitric metabolites have been reported to be elevated in patients with rotavirus gastroenteritis-induced convulsions.22 Marked elevation of interleukin-6 was reported in the CSF of a patient with rotavirus cerebellitis,2 suggesting CNS inflammation with or without rotavirus direct invasion. There have been, however, no reports explaining why rotavirus might affect the cerebellum more than the cerebrum.
The MR imaging finding of reversible splenial lesions with homogeneously reduced diffusion in the acute stage between days 4 and 6 in this series was also interesting. An isolated splenial lesion with homogeneously reduced diffusion (sometimes associated with symmetric white matter lesions) is a key finding for the diagnosis of MERS.3,4 The clinical symptoms of MERS consist of delirious behavior, disturbance of consciousness, and seizures, all of which completely resolve within a month.3,4 Although several patients have been reported having MERS associated with rotavirus gastroenteritis,5 there has been no report of patients presenting with both acute cerebellitis and a reversible splenial lesion. Splenial lesions were recognized between days 4 and 6 in 6 of the 11 patients in this series; these were identical to those reported in MERS in location, signal intensity, and complete reversibility. Three of the 6 patients had an isolated splenial lesion that, in patients with MERS, would suggest probable clinical and radiologic reversibility. Although there was complete resolution of the splenial lesion in all 6 patients, follow-up MR imaging showed cerebellar involvement, and the 6 patients developed disturbance of consciousness, mutism, and finally neurologic sequelae. It is, therefore, important to recognize that an isolated splenial lesion with homogeneously reduced diffusion is not always a benign sign predicting complete clinical and radiologic recovery, especially in pediatric patients with rotavirus gastroenteritis.
This study has some limitations. Patients were selected retrospectively on the basis of a diagnosis of rotavirus cerebellitis and associated MR imaging abnormalities. Some patients with rotavirus cerebellitis may not have any MR imaging abnormality, or some patients with other types of viral infections may develop this type of cerebellitis. PCR or antigens of rotavirus in the CNS, and cytokines of blood and CSF were not examined in most patients enrolled in this study. Such evaluations in the future, in addition to pathologic investigations, may lead to a better understanding of the pathophysiology of rotavirus cerebellitis.
Conclusions
This study suggests that rotavirus cerebellitis concurrent with encephalitis has characteristic clinical and radiologic features, in particular disturbance of consciousness after gastroenteric symptoms, followed by mutism, and MR imaging findings with a reversible splenial lesion in the acute stage, abnormal signal intensity in the cerebellar white matter/nuclei in the acute-to-subacute stages, followed by increased signal intensity in the cerebellar cortex, and finally cerebellar atrophy. Involvement of the cerebellar white matter/nuclei may be associated with the mutism characteristic of rotavirus cerebellitis. An isolated splenial lesion with homogeneously reduced diffusion is not always an indicator of complete clinical and radiologic recovery in patients with rotavirus gastroenteritis.
Acknowledgments
We thank the patients and families for their contribution to this study, and Shoko Yoshida, MD, at the Department of Radiology, Kyoto City Hospital, Kyoto, and Hideki Hoshino, MD, at the Department of Neurology, National Center for Child Health and Development, Tokyo, Japan, for referring patients and their valuable comments.
Footnotes
-
Indicates Fellows' Journal Club selection
-

-
This work was supported in part by the Research Grant (20A-14) for Nervous and Mental Disorders from the Ministry of Health, Labour and Welfare of Japan.

Indicates open access to non-subscribers at www.ajnr.org
References
- Received January 29, 2010.
- Accepted after revision March 9, 2010.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Molecular Analysis of Non-structural Protein 1 (NSP1) in Children Infected with Rotavirus in Babylon Province, Iraq: A Cross-Sectional Study
- Can MRI Differentiate between Infectious and Immune-Related Acute Cerebellitis? A Retrospective Imaging Study
- Febrile encephalopathy and diarrhoea in infancy: do not forget this culprit